
Abstract
Background
It is vital to detect macroenzymes in patients’ plasma or serum since their presence may lead to spurious elevation of enzyme activity, thereby causing diagnostic confusion. Our service for macroenzyme detection has been made available to laboratories throughout the UK. This report describes our laboratory's experience with macro-creatine kinase (CK) detection over a 10-year period.
Methods
In each sample received, the presence of macro-CK was looked for by both polyethylene glycol percent precipitable activity (%PPA) and isoenzyme electrophoresis (IsoEP). The accumulated findings over 10 years were reviewed.
Results
Out of a total number of 255 requests received from throughout the UK, 30 patients (11.8%) were found to be positive for macro-CK (28 type 1 and 2 type 2). Among those found to be positive, the total CK elevation was relatively modest and the %PPA positively correlated with macro-CK by IsoEP and densitometry (Spearman r s = 0.631). The upper reference limit for %PPA of CK could be increased from 37% to 45% after assessment by both an International Federation of Clinical Chemistry-approved calculation and by receiver operating characteristic curve analysis.
Conclusions
Adoption of this change would allow for a more cost-effective investigation protocol. More than 80% of those positive for macro-CK type 1 (immunoglobulin bound) were female, which conforms to findings in many autoimmune processes.
Introduction
First described by Peter Wilding and his colleagues 1 in 1964, high-molecular-mass forms of serum enzymes have been observed for most enzymes routinely measured in clinical laboratories. Immunoglobulin-associated forms are described as type 1 macroenzymes; any others are termed as type 2. Their presence may result in the persistence of abnormally elevated activity in serum or plasma by mechanisms involving reduced inactivation, clearance or excretion. 1 Macroenzymes are indistinguishable from normal enzymes during a routine assay. It is most important that biochemists and clinicians are aware of the existence of this phenomenon. Failure to detect their presence when circulating enzyme activities are elevated can cause diagnostic confusion and potentially lead to invasive and unnecessary further investigative procedures. 2
Approximately 10 years ago, in order to investigate and detect possible cases of macroenzymes, techniques involving polyethylene glycol (PEG) precipitation and isoenzyme electrophoresis (IsoEP) were developed and set up at the laboratory at University Hospital Crosshouse for some commonly measured enzymes. 3 In the ensuing period, it turned out that approximately 80% of subsequent requests received were solely for the investigation of possible macro-creatine kinase (CK). The purpose of the present report was to review the findings for macro-CK investigation over the period; refine, if required, the reference range for PEG precipitable activity (PPA); update our investigative protocol in the light of experience gained; and, if possible, obtain further insight into the process of formation of macroenzymes.
Patients and methods
Over the period 2001–2011, samples of serum or lithium heparin plasma were received for investigation of the presence of CK macroenzymes. Those samples received from external laboratories were sent by post. On the day of receipt, or the next day, CK activity was measured by the International Federation of Clinical Chemistry (IFCC)-recommended method
4
on a Roche Modular analyser (Roche Diagnostics Ltd, West Sussex, UK). For measurement of percent (%) PPA of CK, 200 μL of patients' plasma or serum was added to either 200 μL of PEG 6000 solution (240 g/L in 9 g/L saline) or 200 μL saline (9 g/L), then vortex-mixed and held at room temperature for 10 min prior to centrifugation using a Heraeus Multifuge 3S (Heraeus Equipment Ltd, Essex, UK) for a further 10 min at 4500 rpm. CK activity was measured on both the supernatant and the saline dilution. The %PPA was calculated as

Subsequent CK isoenzyme analysis was also performed on every specimen received using the Sebia Hydrasys electrophoresis system (Sebia (UK) Ltd, Camberley, UK). In this system, macro-CK type 1, a complex between CK and immunoglobulins, is detectable as a band of activity occurring midway between the MM and MB fractions (M, muscle type, B, brain type). The mitochondrial macro-CK type 2 polymer is detectable as a band occurring on the cathodic side of the MM fraction (Figure 1). All results for macro-CK testing were obtained by searching our macroenzyme database at the University Hospital Crosshouse laboratory from mid-2001 to mid-2011. The data gathered included details of patient demographics, source of request, information supplied on request form, total CK activity, %PPA and IsoEP findings. A result was deemed to be positive for macro-CK if either a type 1 or a type 2 band was visually observable on the isoenzyme electrophoretogram.
Schematic representation of the creatine kinase (CK) isoenzyme electrophoretogram. Track 1: control serum displaying CK MM, CK MB and CK BB; track 2: example of serum or plasma containing both CK MM and macro-CK type 1; track 3: example of serum or plasma containing both CK MM and macro-CK type 2; Track 4: example of typical normal serum or plasma showing CK MM only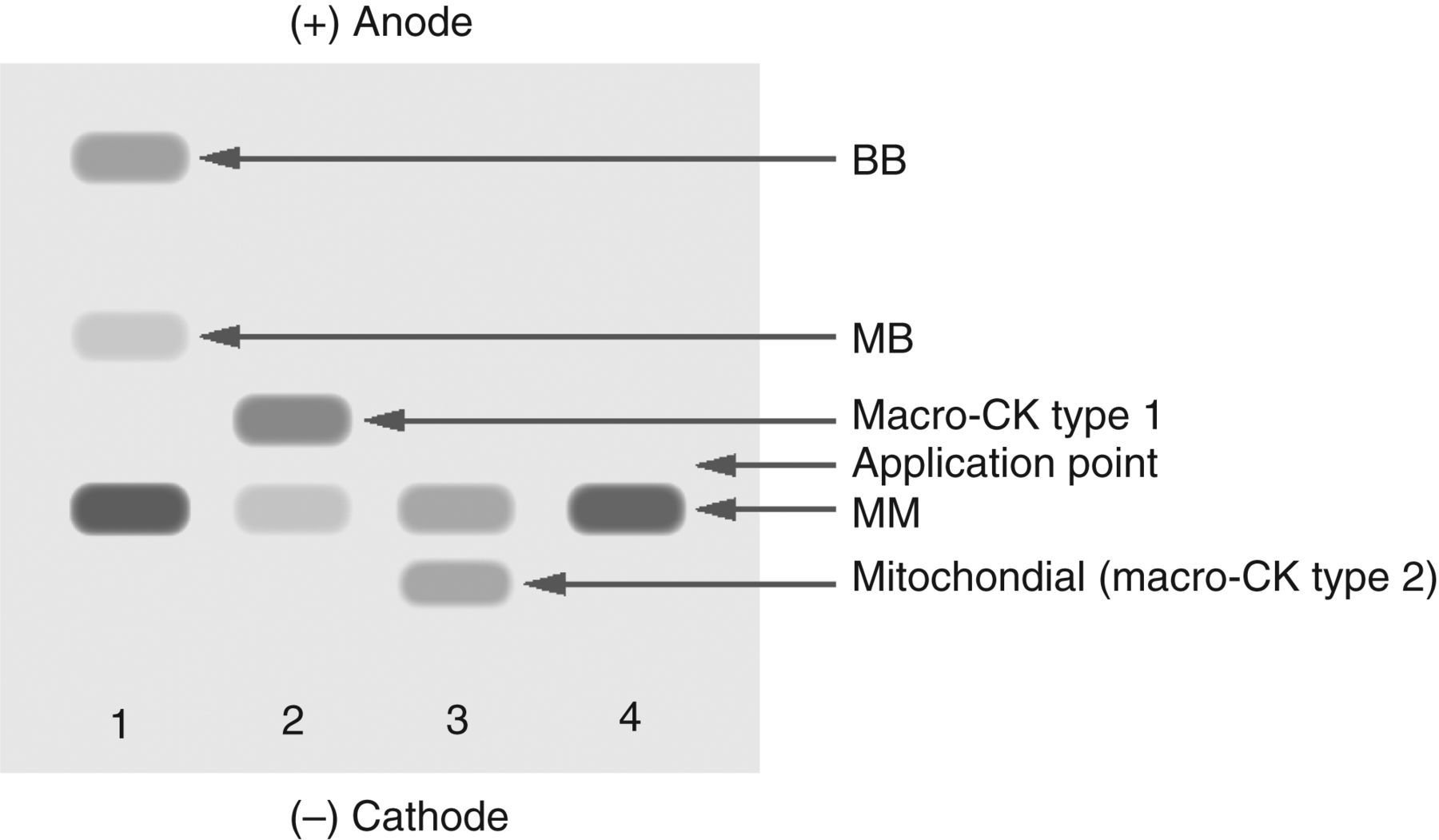
Data analysis
Statistical analysis was performed using the MedCalc statistical software package (version 11.3.3.; MedCalc Software, Mariakerke, Belgium). A redefined reference interval for %PPA was considered using the results from patients whose samples were negative for macro-CK by IsoEP. The calculation of reference interval was as described in the IFCC guidelines using the robust calculation. 5
Results
During the period of observation, one request for macro-CK analysis was received in 2001 and only three in 2002. Requests then rose gradually thereafter to reach an average of 30–40 requests per year. The total number of requests received during the 10-year review period was 255, and comprised 169 from Scottish laboratories, including 83 from our local health board area, and the remaining 86 were from hospital laboratories in England and Wales. Overall, the median patient age was 60 years and comprised 68 women and 187 men. Of the 255 patients tested during the evaluation period, 30 (11.8%) were found to be positive for the presence of macro-CK by IsoEP. Of these, 28 were identified as type 1 and only two as type 2 macro-CK.
Request form information
Review of the clinical details given on request forms showed that on 87 (34.1%), there was no information supplied. In 48 (18.8%), there was mention of ‘statin therapy’ or ‘hyperlipidaemia’. On a further 102 (40.0%), the only detail was ‘high CK’ while in the remaining 18 (7.1%), the information was varied and non-specific, e.g. ‘fatigue’, ‘weight loss’, ‘joint pains’ and ‘diabetes’.
Total CK activity
In our laboratory, the adult upper reference limits for plasma CK are 195 U/L for men and 170 U/L for women. Among the 30 patients positive for macro-CK, the total CK activity showed a median (range) of 686 U/L (241–1238 U/L) and conformed to a normal distribution as determined by the Kolmogorov–Smirnov test (P = 0.7213). On the other hand, the 225 patients deemed negative displayed a more skewed distribution with a number of outliers and a median (range) of 509 U/L (74–6424 U/L) which included seven patients with normal total CK activity (Figure 2). However, comparison of the median total CK activities for those with or without the presence of macro-CK (by the Mann–Whitney U test for unpaired observations) indicated that both groups were likely to derive from a similar population (P = 0.2533).
The distributions of total creatine kinase (CK) activity in those with and without the presence of macro-CK (macro-CK-negative = 0; macro-CK-positive = 1); horizontal lines indicate median values for total CK (U/L)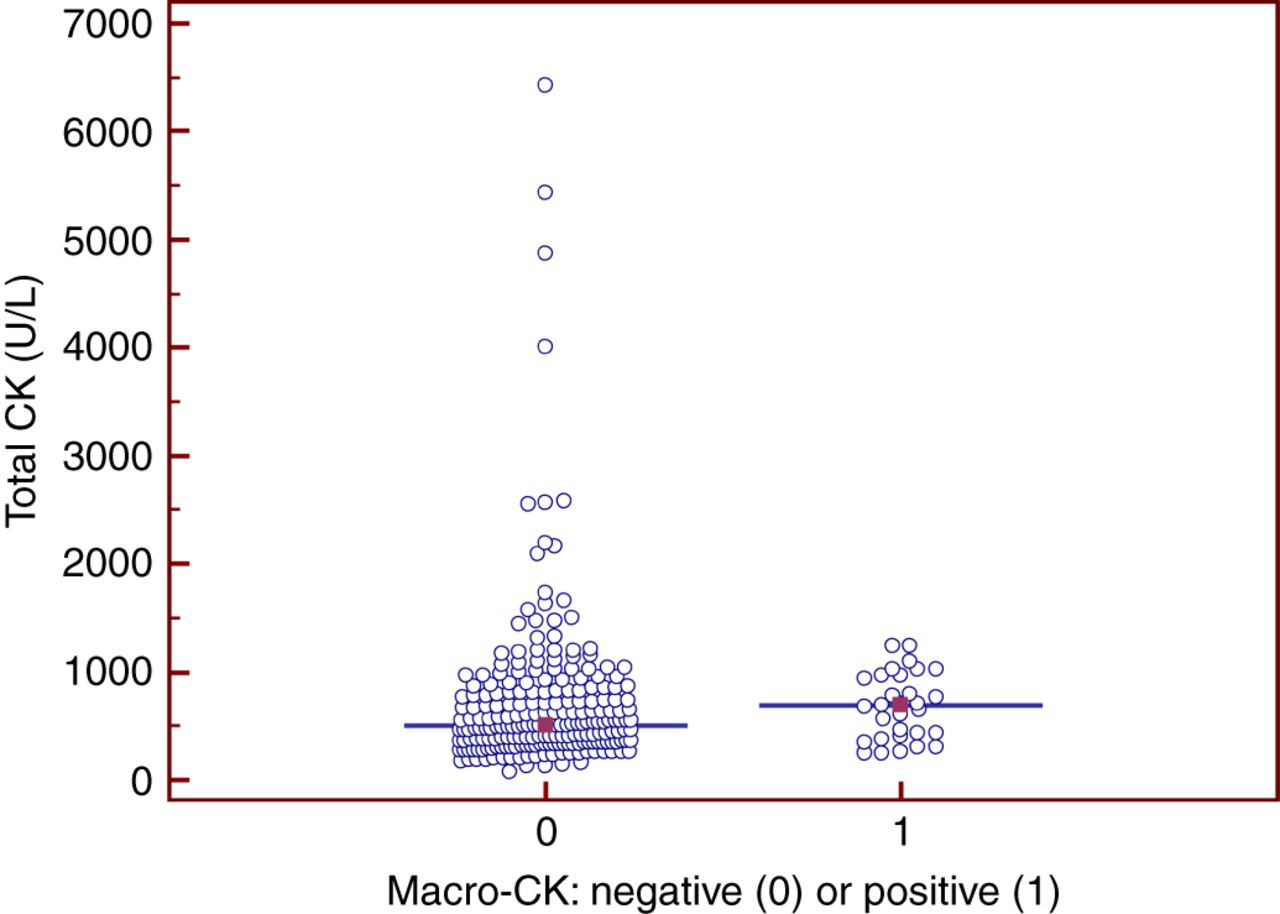
Relationship between %PPA and macro-CK by scanning densitometry
Among those positive for macro-CK by IsoEP, there were values for percentage of macroenzyme, obtained by scanning densitometry, and available for 25 of the 30 patients. Assessment of the association between %PPA and IsoEP for macro-CK for these 25 patients by Spearman rank correlation yielded a value of rs = 0.631 (P = 0.0007).
Reference range for CK %PPA
The original reference range proposed for %PPA for CK activity was 12–37% and was based on the observations from 40 patients following normalization of the data by logarithmic transform. 3 However, it was conceded in that report, that the number of subjects on which ranges were based may be considered to be relatively small, and, with the gradual accumulation of more data over time, that the reference range for %PPA for CK may require alteration. 3 In the present study, recalculation of the reference interval by the IFCC-approved robust method (CLSI C28-A3), using the data from the 225 patients who were negative for the presence of macro-CK by IsoEP, yielded an upper limit of 47%. Analysis of variance (Kruskal–Wallis test) indicated that there was no difference for %PPA among the results for this reference group between men and women (P = 0.9434).
Receiver operating characteristic curve analysis
It would be useful to determine if there is a particular value for %PPA below which further testing for the presence of macro-CK by IsoEP was unlikely to yield a positive result, i.e. a cut-off value representing 100% sensitivity at the expense of the highest value representing maximum specificity. After dividing the data into the 30 patients positive for macro-CK and 225 who were negative, receiver operating characteristic (ROC) curve analysis indicated that a cut-off point for %PPA of 46% was appropriate and yielded a sensitivity of 100% and a specificity of 96.4% (Figure 3).
Receiver operating characteristic curve for the percent precipitable activity (%PPA) test for the detection of macro-creatine kinase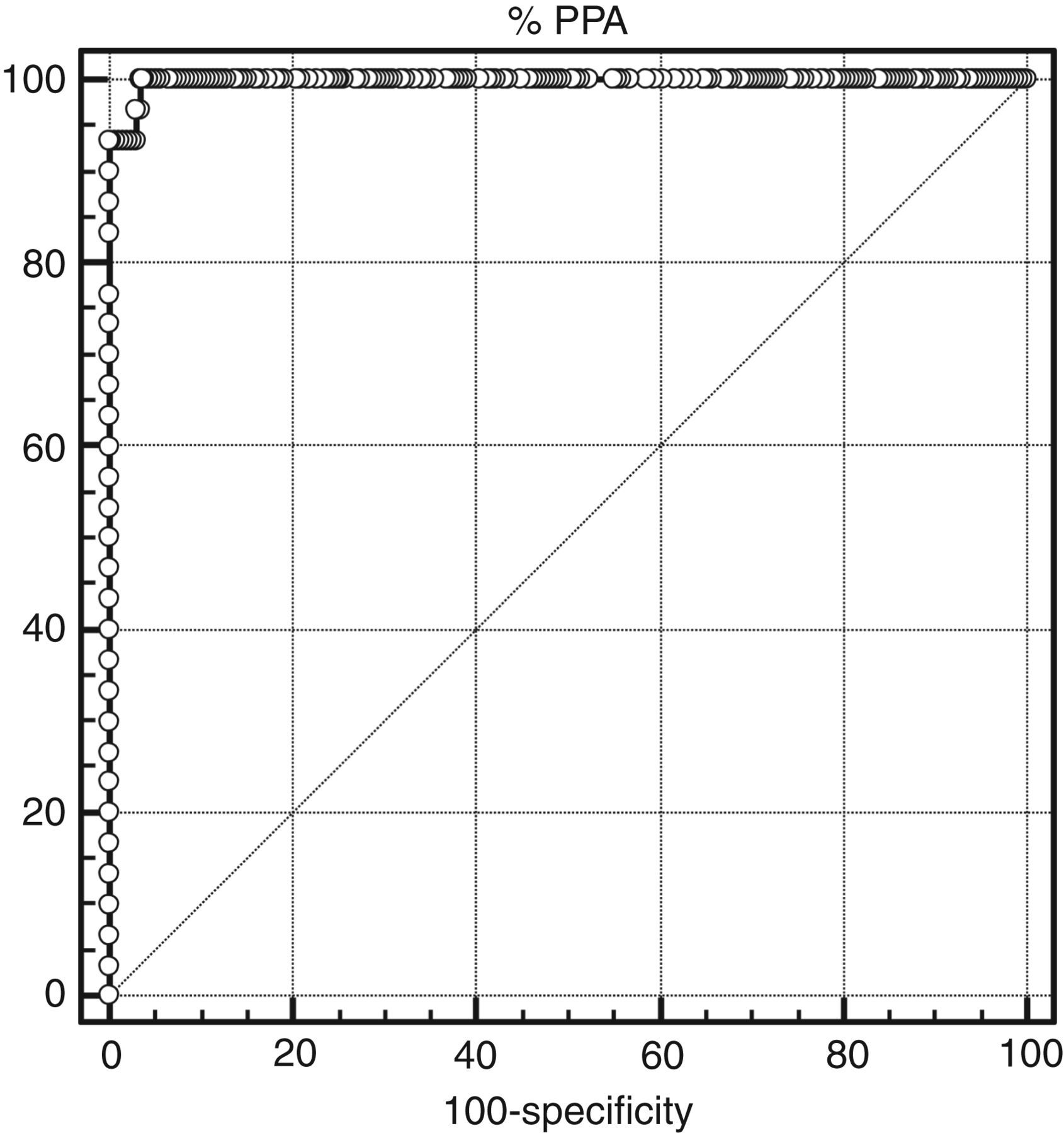
Gender
Of the 255 patients whom were invited to test for the presence of possible macro-CK, there was a disproportionate number of men (187/255; 73.3%) versus women (68/255; 26.7%). Both examples of those positive for macro-CK type 2 were male patients with CK (and %PPA) values of 567 U/L (%PPA 66.1%) and 706 U/L (%PPA 95.9%), respectively. However, on considering the 28 patients positive for type 1 macro-CK (immunoglobulin-bound), there were 24 women and only four men, thereby resulting in a female-to-male ratio of 6 to 1.
Summary of study findings
IsoEP, isoenzyme electrophoresis; CK, creatine kinase; n, number of patients; %PPA, percent precipitable activity
Discussion
The patients being investigated for the presence of macroenzymes as described in this study probably represent a highly disparate group. Consequently, the absence of useful information on accompanying request forms did not allow observation of any associations between clinical findings and macroenzyme findings of the kind noted either when the catchment area is from a single health authority, or where patients form a single clinical group, thereby allowing ready access to detailed patient records. 2,6–8 For example, in a retrospective study of patients manifesting type 1 macro alkaline phosphatase, Crofton et al. 6 were able to demonstrate a likely association with an autoimmune aetiology. Similarly, in a selective group of patients with liver disease, Wenham et al. 7 showed an association between the presence of lipoprotein-bound macro-γ-glutamyltransferase and extrahepatic obstructive jaundice; while others have screened for the presence of macro-CK from their own locally-obtained workload on the basis of a confirmed elevation of serum CK activity. 8
In the present study, the level of elevation of CK activity among those found to be positive for the presence of macro-CK was relatively modest, displaying a median of around four times our upper normal limit, and a range no more than approximately six or seven times this value. This finding is similar to that reported by Mapplebeck et al., 9 albeit in a screening study using gel filtration chromatography rather than IsoEP as a confirmatory test for the presence of macro-CK. In the present study, among those who were negative for the presence of macro-CK, there were samples from seven patients who exhibited total CK results which were within our normal reference ranges. One can only speculate as to why samples from such individuals were submitted for detection of a possible macro-CK. On examining the accompanying request form information, it seemed likely that these individuals had exhibited an elevated CK on a previous occasion.
Although %PPA and IsoEP do measure different properties of macro-CK, both parameters do increase in relative proportion to each other as assessed by Spearman rank correlation. It was assessed that in terms of reagent cost for macro-CK detection, IsoEP is approximately 10 times that of the measurement of %PPA. Hence, one way of saving cost would be to apply measurement of %PPA to all samples received, and only perform further IsoEP analysis on those samples exhibiting values above a predetermined cut-off point. The calculation of upper reference limit for %PPA in this study was 47%. Further analysis of the data by ROC curve analysis has indicated that a suitable cut-off point for %PPA could be a similar figure of 46%. Hence, we could change our investigation protocol based on the findings of this in-house review such that only those samples manifesting a %PPA greater than 45% would be subjected to further analysis by IsoEP, thereby making a considerable relative cost-saving.
It is something of a paradox that, in this study, despite the fact that the great majority of samples were from male patients, the relatively greater majority of positive findings arose in females. However, although macroenzyaemia is not a disease, it is possible that the formation of type 1 macroenzymes, including macro-CK type 1, is itself a manifestation of an autoimmune process. 10 Among autoimmune disorders, an important unifying theme is a high prevalence in women. 11 In many instances of systemic autoimmune disease, women tend to predominate and the magnitude of this often-observed, and quite striking, sex difference varies among different diseases. 12 Examples well known to biochemistry laboratories are autoimmune thyroid disease where the female:male ratio can be as high as 9:1, or insulin-dependent diabetes mellitus where the female predominance is very much less prominent (ratio < 2:1). 13 If this study is representative of the true prevalence of individuals manifesting a sustained yet unexplained increase in CK, then, of the 28 positive for the presence of CK type 1 (immunoglobulin-bound) macroenzyme, 24 were women, yielding a ratio of 6:1. For an up-to-date review of current research into the increased susceptibility of women to autoimmune diseases, the reader is referred to the recent article by Professor Voskuhl. 14
DECLARATIONS