
Abstract
Background
The increase in creatinine in patients on fibrate therapy is well-recognized, but its mechanism is not clearly understood. A study by Hottelart et al. suggested that fibrate-induced creatininaemia was due to the effect of fibrates on creatinine metabolism as opposed to a decline in renal function. To address this hypothesis, we have monitored renal function in a group of hyperlipidaemic patients before commencing fibrate treatment and after three months of therapy.
Methods
We studied 12 subjects (10 men, 2 women), median age 43.5 y (range 33–70 y). Serum creatinine, cystatin C, creatine kinase and fasting lipids were measured.
Results
We observed statistically significant increases in concentrations of serum creatinine (P < 0.005) and cystatin C(P < 0.01). Concentrations of both analytes increased in 10 (83.3%) of the patients. In these patients, the median increases were 15.1% (range 5.5–23.2%) for creatinine and 9.9% (range 1.1–26.1%) for cystatin C.
Conclusions
These results suggest that the decrease in estimated glomerular filtration rate, observed in patients undergoing fibrate therapy, is a genuine effect on kidney function rather than a change in creatinine metabolism as previously postulated, since the rises in serum creatinine concentration were reflected by rises in cystatin C, an independent marker of renal function.
Introduction
Fibrates are a group of lipid-regulating drugs that are derived from fibric acid. They act mainly by lowering serum triglyceride concentration and can also increase concentrations of serum HDL cholesterol, which may reduce cardiovascular risk.
Fibrate-induced elevation in serum creatinine concentration is well-recognized, but its mechanism is not clearly understood. A study by Hottelart et al. 1 suggested that this reversible creatininaemia results from an increased endogenous production of creatinine as opposed to a decline in renal function. In the present study, we have tested this hypothesis by monitoring renal function, as measured by serum creatinine and cystatin C, in a group of hyperlipidaemic subjects undergoing therapy with fenofibrate. Cystatin C, an endogenous marker of glomerular filtration rate (GFR), is considered close to ‘ideal’, since unlike creatinine, it is not secreted by renal tubules and is unaffected by race or diet. 2
Methods
Patient group
Twelve hyperlipidaemic patients (10 men, 2 women), median age 43.5 y (range 33–70), were recruited into this study, four of whom had diabetes mellitus. Blood samples were collected before (baseline) and three months after commencing fenofibrate therapy (267 mg daily).
Analytical methods
All assays were performed using a Siemens ADVIA 1800 system. Creatinine was measured by an enzymatic method (ECreat_2®); fasting lipids, total cholesterol, HDL-cholesterol, triglycerides and creatine kinase (CK) were determined using routine assays; and cystatin C was measured using a latex-enhanced immunoturbidimetric method (Siemens Healthcare Diagnostics Ltd, Frimley, UK). Samples for cystatin C and creatinine were run in the same analytical batch. Preliminary assay validation using aliquots of pooled serum demonstrated that samples were stable for at least 12 months when stored at −20°C. The maximum storage period for any of the patient samples was eight months.
Statistical analysis
Statistical analysis was performed using SPSS® software version 19 (IBM Corporation, Armonk, NY, USA). Differences in serum creatinine and cystatin C concentrations before and after three months of fenofibrate treatment were analysed using the Wilcoxon signed-rank test, since these data showed a non-normal distribution. Changes in fasting lipid concentrations were normally distributed and were analysed using Student's paired t- test. A P value <0.05 was considered significant.
Results
Fasting serum triglyceride and total cholesterol concentrations fell following fenofibrate treatment. The mean triglyceride concentration decreased by 38.8%, from 2.99 mmol/L at baseline to 1.87 mmol/L (P < 0.05). The mean total serum cholesterol concentration fell by 22.2%, from 6.02 mmol/L to 4.70 mmol/L (P < 0.001). The mean HDL-cholesterol concentration did not change significantly, with concentrations of 1.18 mmol/L at baseline and 1.24 mmol/L after fibrate therapy (P = 0.648).
The median estimated glomerular filtration rate (eGFR) at baseline was 81 mL/min/1.73 m2 (range 52–122 mL/min/1.73 m2) using the abbreviated Modification of Diet in Renal Disease equation. In all patients, there was an increase in either creatinine or cystatin C. The median creatinine at baseline was 87 μmol/L (interquartile range 71–108 μmol/L) and increased to 89 μmol/L (interquartile range 84–117 μmol/L) after three months of fenofibrate therapy (P < 0.005).
Before commencement of fenofibrate treatment, the median cystatin C concentration was 0.79 mg/L (interquartile range 0.72–0.92 mg/L). This increased to 0.89 mg/L (interquartile range 0.82–1.02 mg/L) after three months of therapy (P < 0.01) (Figure 1).
Box plots showing the effect of fenofibrate on (a) creatinine (P < 0.005) and (b) cystatin C (P < 0.01) demonstrated by the Wilcoxon signed-rank test. Boxes show medians and interquartile ranges with the lowest and highest values obtained are shown above and below each box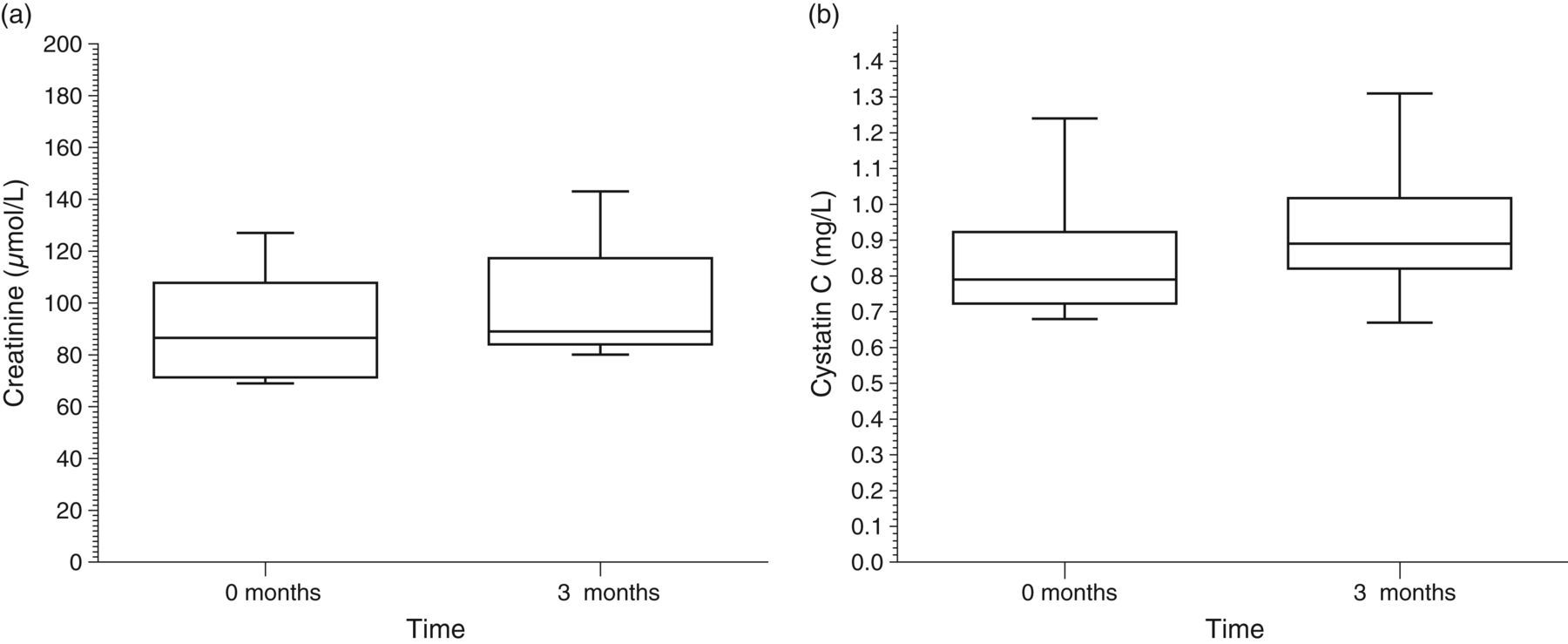
In 10 patients (83.3%), increases in median concentrations of both analytes were observed, namely, 15.1% (range 5.5–23.2%) for creatinine and 9.9% (range 1.1–26.1%) for cystatin C. In only two subjects was a decrease in one or other parameter observed. In one subject, a 9.5% decrease in cystatin C was accompanied by a 20.2% increase in creatinine, and in the other, a fall in creatinine of 4.4% was accompanied by an increase in cystatin C of 13.3%. There was no correlation between changes in CK activity and markers of renal function, and CK activity remained within the reference interval for all patients.
Discussion
The mechanism by which fenofibrate increases serum creatinine has been addressed in previous studies, but no firm conclusion has been reached. 3–6 One view is that fibrates increase the metabolic production of creatinine. 1 Another suggests that fibrates impair renal function by altering renal blood flow via a peroxisome proliferator-activated receptor-α-mediated decrease in renal synthesis of vasodilatory prostaglandins. 3 A third, proposes that the concentration of serum creatinine increases in response to fibrate-induced myopathy. 1 However, none of the subjects in the present study complained of muscle aches, or demonstrated an increase in CK above the reference interval, and there was no correlation between changes in CK and changes in either cystatin C or eGFR.
In the present study, the observed increases in creatinine and cystatin C during fenofibrate therapy were clinically modest. For example, in only 22% of patients with baseline serum creatinine concentrations within the reference interval did the creatinine rise above the upper reference limit (URL). Similarly, for cystatin C, only 27% of patients had post-therapy values above the URL.
The changes in these parameters in the study group were statistically significant (P < 0.005 and P < 0.01 for creatinine and cystatin C, respectively). In a similar investigation by Ansquer et al., 4 the increases in creatinine and cystatin C results mirrored those observed in the present study. However, these authors observed no change in inulin clearance in the subjects studied, after fenofibrate therapy. This was possibly because a lower dose of fenofibrate (160 mg/d) was administered over a shorter period (six weeks). Ansquer et al. 4 postulated that the reasons inulin clearance did not alter in their study were due to the small sample size and relatively short duration of their study.
In conclusion, the increases in serum creatinine observed in the subjects in the present study were reflected by the changes in cystatin C, a second, independent marker of renal function. These results suggest that the decrease in eGFR, as calculated from serum creatinine concentration, reflects a genuine effect on kidney function, rather than a change in creatinine metabolism as has been previously proposed. 1 Our data are in accord with previously published findings 3–5 and with a substudy of the Fenofibrate Intervention and Event Lowering in Diabetes (FIELD) trial. 6 In view of this, we recommend that renal function should be closely monitored in all patients undergoing lipid-lowering therapy with fibrates.
DECLARATIONS