
Abstract
Background
We previously reported that the indicator of glycaemic control, glycated albumin (GA) levels, are low in relation to glycaemia in patients with high alanine aminotransferase (ALT) levels in non-alcoholic fatty liver disease because of chronic inflammation, and that the GA/glycated haemoglobin ratio (G/H ratio) is inversely correlated with hepatic function in patients with chronic liver disease. The severity of liver fibrosis is known to be a good indicator for surveillance, and for determining the prognosis and optimal treatment of non-alcoholic steatohepatitis (NASH). In this study, we aimed to investigate the clinical usefulness of measuring the G/H ratio for predicting the severity of liver fibrosis in patients with NASH.
Methods
The study subjects were 36 patients with histologically diagnosed NASH (19 men, 17 women; mean age54.8 ± 12.2 years, body mass index 28.3 ± 5.0 kg/m2). The relationships of the G/H ratio to hepatic function tests and fibrosis stage in the liver were investigated.
Results
The G/H ratio in patients with NASH was inversely correlated with ALT (P < 0.001) and platelet count (P < 0.0001). Furthermore, the G/H ratio was positively correlated with the fibrosis stage in liver (P = 0.003).
Conclusions
These results suggest that the G/H ratio increases along with the fibrosis stage in patients with NASH.
Introduction
Non-alcoholic fatty liver disease (NAFLD) is the most common cause of chronic liver disease, affecting up to 20% of the population in Western countries, and 70–80% of obese individuals. 1,2 The incidence of NAFLD is increasing due to the ongoing epidemic of its two major risk factors, obesity and type 2 diabetes mellitus, related to a sedentary lifestyle and inadequate dietary choices. It encompasses a spectrum of distinct histological entities with different natural histories and outcomes, ranging from simple fat accumulation in hepatocytes to liver steatosis accompanied by a microinflammatory component that may have associated fibrosis. In contrast to simple steatosis, which is defined as a benign form of NAFLD with minimal risk of progression, non-alcoholic steatohepatitis (NASH) can progress to liver cirrhosis in up to 20% of patients and subsequently lead to hepatic failure or hepatocellular carcinoma. 3,4
Diabetic patients are known to show greater glycation of various proteins than non-diabetic subjects and it has been suggested that some of these glycated proteins are involved in the onset and development of the chronic complications of diabetes. 5 One of these glycated proteins, glycated haemoglobin (HbA1c), is often used in clinical settings as an indicator of glycaemic control. 6,7 Since the lifespan of erythrocytes is approximately 120 days, HbA1c reflects the glycaemic control status of the previous 2–3 months. However, measurement of HbA1c is affected in diseases in which the erythrocyte lifespan is shortened, such as haemolytic anaemia and renal anaemia, and with variant haemoglobins, and thus HbA1c does not accurately reflect the glycaemic control status in such cases. 8,9
Glycated albumin (GA) is used as another glycaemic control indicator. 6 Since the half-life of serum albumin is shorter than that of erythrocytes, at 14 days, GA reflects plasma glucose concentrations over a shorter period (approximately two weeks). Moreover, GA has a benefit in that its measurements are not affected by haemoglobin disorders. 10 However, measurements of GA are affected in patients with disorders of albumin metabolism, such as in nephrotic syndrome or thyroid dysfunction, and do not correctly reflect the glycaemic control status in such cases. 11
It has been recently demonstrated that GA is low relative to plasma glucose concentrations in obese patients with diabetes. 12 We observed a significant negative correlation between body mass index and GA even in non-diabetic subjects. 13 We also demonstrated a significant negative correlation between highly sensitive C-reactive protein (hs-CRP) and GA, and that hs-CRP was a significant negative explanatory variable for GA in a multivariate analysis. 13 From the finding that hs-CRP is elevated as a result of accelerated release of various cytokines in obesity, we hypothesized that the negative regulatory mechanism of GA resulting from obesity is based on accelerated albumin catabolism accompanied by chronic microinflammation. 13 We have also reported low levels of GA by similar mechanisms in smoking, 14 hyperuricaemia 15 and hypertriglyceridaemia, 16 which are representative conditions causing elevated hs-CRP. High levels of hs-CRP have also been reported in NAFLD patients with high alanine aminotransferase (ALT). 17,18 We reported GA concentrations to be low in relation to glycaemia in patients with high ALT without a drinking habit. 19
It has been demonstrated that patients with chronic liver disease (CLD) have apparently low HbA1c 20,21 due to a shortened lifespan of erythrocytes that is caused by hypersplenism. Furthermore, since the ability of albumin synthesis is impaired and the half-life of serum albumin is prolonged in patients with CLD, 22 their GA concentrations appear to be high relative to glycaemia. 23 Therefore, the GA/HbA1c ratio (G/H ratio) in patients with CLD was shown to be correlated with hepatic function irrespective to glycaemia. 24
The severity of liver fibrosis is known to be a good indicator for surveillance, and for determining the prognosis and optimal treatment of NASH. In this study, we aimed to investigate the clinical usefulness of measuring the G/H ratio for predicting the severity of liver fibrosis in patients with NASH.
Methods
Study patients
GA and HbA1c were simultaneously measured in 36 patients with NASH (Table 1) undergoing treatment at Fukui-ken Saiseikai Hospital or Hyogo College of Medicine. Among the 36 patients, 26 patients (72%) displayed complications of type 2 diabetes mellitus. Patients with unstable glycaemic control were excluded. The diagnosis of NASH was made histologically, and the fibrosis stage was classified as S1–S4 according to the method of Brunt et al. 25 This study was approved by the ethics committee at Fukui-ken Saiseikai Hospital and Hyogo College of Medicine. The purpose of the study was explained to all patients, and all patients provided their written informed consent.
Clinical characteristics of the study patients classified by the stage of fibrosis*
BMI, body mass index; DM, diabetes mellitus; ALT, alanine aminotransferase; Hb, haemoglobin; HbA1c, glycated haemoglobin; GA, glycated albumin; G/H, GA/HbA1c
*The fibrosis stage was classified as S1–S4 according to the method of Brunt et al. 25
Laboratory measurements
HbA1c was measured by high-performance liquid chromatography, with calibration using Japan Diabetes Society (JDS) Lot 2. 26 The value for HbA1c (%) was estimated as a National Glycohemoglobin Standardization Program (NGSP) equivalent value (%) calculated using the formula HbA1c (%) = HbA1c (Japan Diabetes Society: JDS) (%) + 0.4%, considering the relational expression of HbA1c (JDS) (%) measured using previous Japanese standard substances and measurement methods and HbA1c (NGSP). 27 Serum GA was determined by enzymatic methods using albumin-specific protease, ketoamine oxidase and albumin assay reagent (Lucica GA-L; Asahi Kasei Pharma, Tokyo, Japan). 28 GA was hydrolysed to amino acids by an albumin-specific proteinase and then oxidized by ketoamine oxidase to produce hydrogen peroxide, which was measured quantitatively.
Statistical analysis
All data are shown as mean ± SD. The significance of the differences between the two groups was calculated using Student's t-test. To evaluate the relationship between the G/H ratio and other variables, Spearman's correlation coefficient was performed. The relationship between the stages of fibrosis on histology and the G/H ratio was tested by analysis of variance with StatView (Version 5.0 for Windows; Abacus Concepts, Berkeley, CA, USA) software. A P value <0.05 was considered significant.
Results
The clinical characteristics of the study patients classified by the stage of fibrosis are shown in Table 1. Serum ALT, platelet count and haemoglobin decreased with the progression of fibrosis. On the other hand, higher GA, but not HbA1c, was seen with the progression of fibrosis. Higher G/H ratios were also seen with the progression of fibrosis (Table 1). A significant inverse correlation was seen between the G/H ratio and serum ALT in patients with NASH (R = −0.572, P < 0.001) (Figure 1a). The G/H ratio was also inversely correlated with platelet count (R = −0.663, P < 0.0001) (Figure 1b).
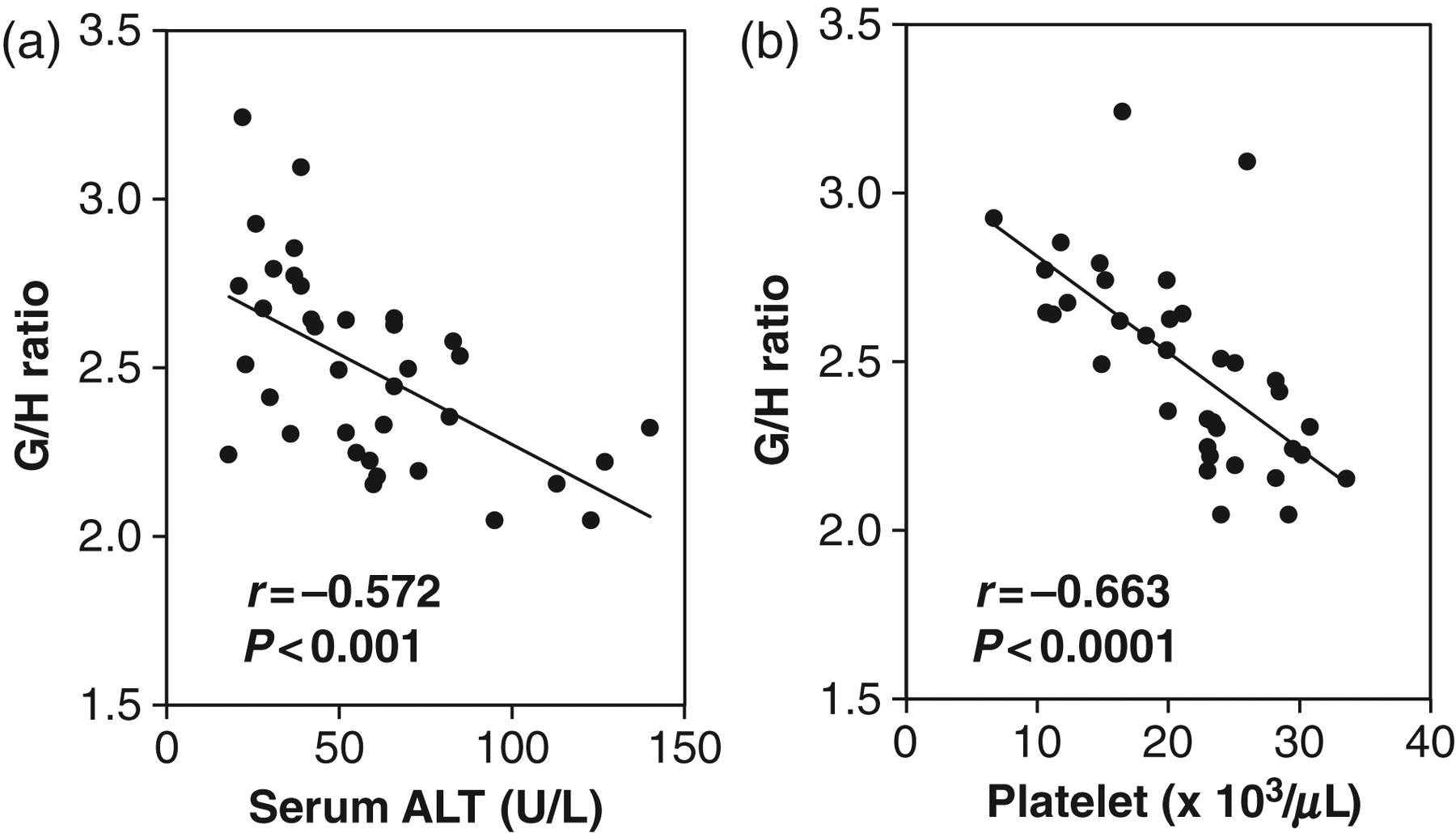
Correlation between the GA/HbA1c (G/H) ratio and serum ALT (a) and platelet count (b) in patients with NASH. HbA1c, glycated haemoglobin; GA, glycated albumin; NASH, non-alcoholic steatohepatitis; ALT, alanine aminotransferase
Discussion
A significant inverse correlation was seen between the G/H ratio and serum ALT in patients with NASH. We previously reported that serum ALT showed significant inverse correlations with both GA and the G/H ratio in patients with NAFLD. 19 In those patients, hs-CRP had a significant positive correlation with serum ALT and a significant inverse correlation with GA, 19 indicating the possibility that GA values declined as a result of accelerated albumin metabolism due to chronic inflammation 29 in patients with NAFLD with high serum ALT. This suggests that GA concentrations are set lower relative to plasma glucose concentrations because of hepatic inflammation in the early stages of NASH, resulting in lower G/H ratios.
The G/H ratio in patients with NASH showed a significant inverse correlation with platelet count, which reflects hepatic function. A significant increase in the G/H ratio was also seen with progressing fibrosis stage histologically. While there was an apparent decrease in HbA1c and an apparent increase in GA in patients with CLD, we previously showed that these indicators diverged markedly with the state of glycaemic control as hepatic function decreased. 23 We also showed that the G/H ratio was related to hepatic function irrespective to glycaemia in patients with CLD. 24 Therefore, it is thought that in patients with NASH, hepatic function declines with the progression of histological findings including fibrosis, finally reaching a state of cirrhosis, while the G/H ratio becomes higher.
The above results are thought to indicate that the G/H ratio in patients with NASH declines in the early stage of the disease, but increases with the progression of the disease, and becomes high in the final stage. These results suggest that the G/H ratio is associated with the progression of fibrosis in patients with NASH. Since other fibrosis markers (hyaluronic acid and type IV collagen) were measured only in a small number of the patients in this study, statistical analysis was difficult to compare the G/H ratio with these markers. The relation between the G/H ratio and such fibrosis markers will need to be studied in future.
DECLARATIONS