
Abstract
Background
Immunoassays for urinary albumin are often subject to the problem of antigen excess (the ‘hook’ effect) at high albumin concentrations. We developed an automated protocol to identify such samples based on urinary albumin to creatinine ratio (uACR) and urinary total protein (uTP) results.
Methods
An automated flagging system was designed and written into the laboratory computer system to alert technical staff to samples potentially affected by the ‘hook effect’. This flag was activated when there was a combination of an uTP of ≥2400 mg/L and an uACR of <30 mg/mmol.
Results
The potential rate of false-negative uACR results was approximately 0.17% in samples from primary care and diabetic clinic sources.
Conclusions
Samples with falsely low uACR results were identified, allowing the vast majority of results to be authorized without intervention. The protocol prevented the reporting of false-negative uACR results which might impact on the management of patients.
Introduction
Urine albumin to creatinine ratio (uACR) is a commonly requested test for the early detection of proteinuria, and therefore chronic kidney disease (CKD). uACR has been recommended as a screening tool for CKD in a number of recent guidelines (NICE, 1 KDOQI 2 ) due to its greater sensitivity for detecting renal protein loss and its technical performance at lower levels of proteinuria.
It is commonly recognized that when measuring albumin in urine with immunoturbidimetric methods, samples with very high concentrations of albumin can be subject to the ‘hook effect’ or antigen excess, resulting in false-negative results. 3 To detect antigen excess, some manufacturers have developed automated techniques. 4 For example, Cobas® reagents for the Roche MODULAR P Analyzer (Roche Diagnostics Ltd, West Sussex, UK) use an additional reagent step where human albumin is added following the initial turbidity measurement. A failure to identify a linear increase in turbidity indicates antigen excess. 4 An alternative approach that avoids the effect of antigen excess is an immunoturbidimetric inhibition technique, which was developed on the Dade aca® IV analyser (Dade International, Wilmington, DE, USA). This technique has the advantage of not requiring extra steps in analysis. 5 In our laboratory, the Olympus AU2700 analyser system (Beckman Coulter [UK] Ltd, High Wycombe, UK) is used for the analysis of urine albumin; an inherent checking system for antigen excess is not available. The aim of this work was to establish a process which would automatically identify uACR samples affected by antigen excess.
Method and results
A simple automated flagging system was designed and written into the laboratory computer systems (Olympus Data Wizard, Beckman Coulter [UK] Ltd and Clinisys WinPath, Guildford, UK) to alert technical staff to urine albumin samples potentially affected by antigen excess. The flag system was activated when urinary total protein (uTP) ≥ 2400 mg/L and uACR < 30 mg/mmol. On being alerted, staff performed a manual dilution of the sample, repeated the albumin analysis and reported the calculated value. The uTP limit of ≥2400 mg/L was chosen as a flag limit as 2400 mg/L is the limit of the Olympus urine albumin assay following automatic on-board dilution. An uTP result at this concentration assumes an urine albumin concentration of <2400 mg/L, which should have been accurately measured by the urine albumin assay. An uACR limit of <30 mg/mmol was chosen as an uACR of ≥30 mg/mmol in non-diabetic patients has been defined as clinical proteinuria. 1 An uTP of ≥2400 mg/L with an uACR of <30 mg/mmol should only occur if the urine albumin assay has been subject to antigen excess or if the patient is losing large amounts of protein other than albumin.
Predicted laboratory impact
In an one-year period (1 September 2009–31 August 2010), approximately 65,000 uACR measurements were made in our laboratory. Each of these requests had uTP as well as albumin analysed, but only 688 of these requests had initially had an urine protein to creatinine ratio (uPCR) requested alongside the uACR; these were mainly from nephrologists. Of the 688 samples in which both uACR and uPCR results were readily available from the laboratory computer system, only one sample would have been identified by the flagging system (Figure 1). By extension, this indicated that approximately 100 samples per year were likely to be flagged; this would have a minimal impact on the laboratory work load. Further, as the majority of the samples in this data-set were from nephrologists, and therefore more likely to be from patients with heavy proteinuria, this could be an overestimate.
The relationship between urinary total protein (uTP) and urinary albumin to creatinine ratio (uACR) in samples requesting both uACR and urine protein to creatinine ratio (uPCR) from nephrology sources during an one-year period. Samples below the horizontal dashed line are those with an uACR of <30 mg/mmol and samples to the right of the vertical dashed line have an uTP concentration of >2400 mg/L. Only samples in the bottom right quadrant of this figure would have been identified by the flagging system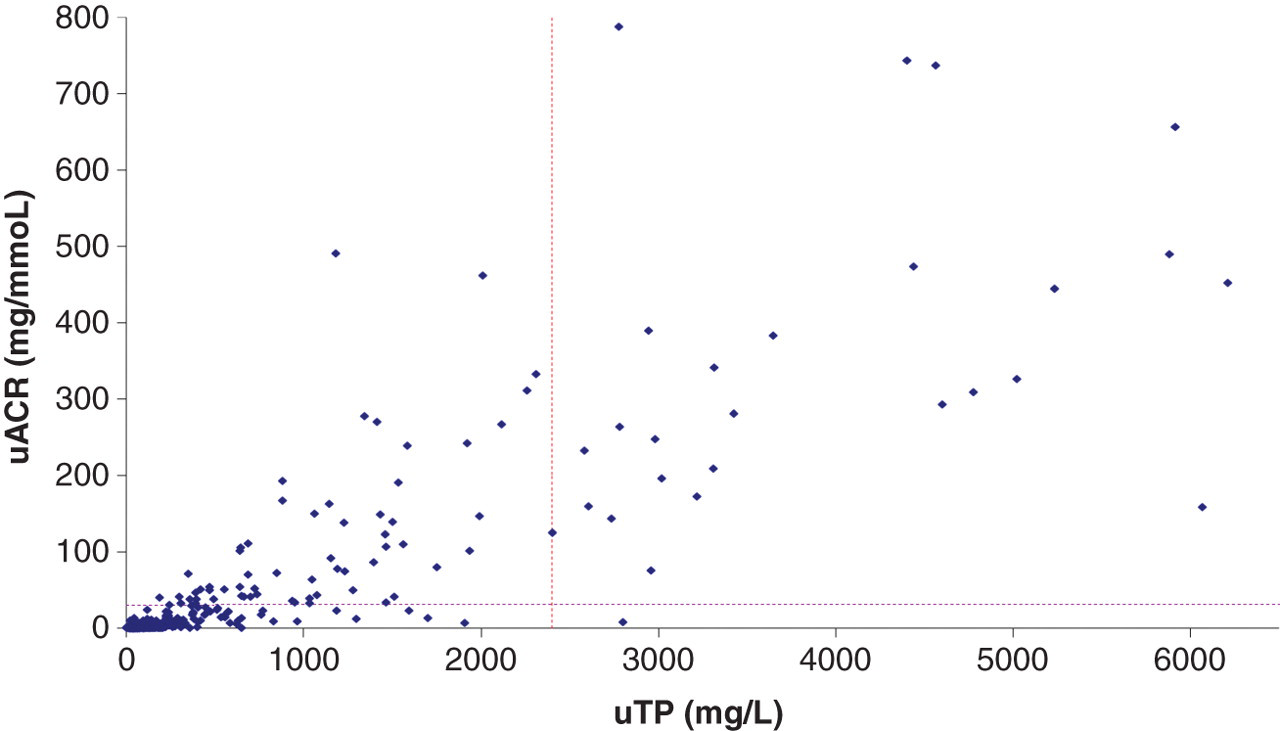
Laboratory data from the seven months following the introduction of the system (1 December 2010–30 June 2011) showed that 64 out of 36,603 primary care or diabetic clinic requested uACRs were flagged (approximately 0.17%), indicating that our predictions regarding the number of samples likely to be identified were reasonably accurate.
Predicted economic impact
The economic impact of introducing this testing strategy was considered negligible as both urine albumin and protein were already being measured by the laboratory on receiving a request for uACR. Including uTP with all requests for uACR costs the laboratory approximately £0.40 extra per sample (£26,000/y). From our total workload and assuming a rate of 0.17% for samples affected by antigen excess, this equates to approximately 110 patients per year who could have a diagnosis of CKD missed on the basis of a false-negative uACR result. Patients identified as having proteinuria are able to benefit from measures aimed at slowing the progression of CKD to established renal failure (ERF). The cost for the treatment of ERF has been calculated to be almost £34,000 per patient per year on haemodialysis (76% of patients with ERF) and around £20,000 per patient per year for those on peritoneal dialysis (21% of patients with ERF). 1 A strategy that prevents false-negative uACR results from being reported, potentially delaying diagnosis of CKD and the start of treatment, is likely to be of benefit to the overall health economy.
Conclusion
This method of identifying the 0.17% urine samples affected by the ‘hook effect’ by measurement of both the uTP and uACR was successfully implemented in December 2010. Samples are clearly identified, allowing the majority of results to be authorized without intervention. uPCR is reported when uACR is increased to assist patient management.
DECLARATIONS