
Abstract
Background
Preventing laboratory errors promotes patient safety and reduces the cost of unnecessary processing.
The aim of this study was to test the effectiveness of two short-term interventions at reducing errors in the preanalytical stage of laboratory testing.
Methods
Error data were reviewed from inpatient wards at Bradford Royal Infirmary (BRI), Leeds General Infirmary (LGI) and St James’ University Hospital (SJUH) for 22 weeks. Two separate interventions lasted for two weeks. The outcome measures were inadequate tube and form labelling, incorrect tube selection and insufficient sample volume. Posters targeting these errors were created and displayed on inpatient wards in SJUH (
Results
There was no change in error rate or type at the intervention site(s) compared with the control(s). There were 7058 reported errors across three sites, of which 6623 were errors targeted by the interventions. The overall error rate remained stable on all three sites (analysis of variance,
Conclusions
Despite enthusiasm on the part of the ward-based staff, both short-term interventions had no significant impact on preanalytical error rates. Most errors are due to human factors. These may be reduced with the introduction of an electronic ordering system.
Introduction
The total testing process can be divided into three main stages describing sample processing before, during and after laboratory analysis. Up to 87% of all errors occur in the preanalytical stage, before the sample reaches the laboratory. 1–4 Apart from incorrect test selection, these include incorrect tube selection, incorrect labelling and insufficient sample volume. 5 While not all errors lead to negative outcomes, Plebani and Carraro 1 found that 26% have a negative impact on patient care. Working to reduce the occurrence of such preventable errors is a high priority.
Three approaches to reducing preanalytical errors include improving training and education for operators; identifying weaknesses and system redesign; and increasing automation to reduce human input.
Long-term continuous education via gentle reminders has shown to reduce errors with wristband identification, in a study using the Q-Tracks programme. 6 However, there is little evidence showing whether short-term interventions have any impact. Quality management techniques such as the hazard analysis and critical control points 7,8 and failure mode and effect analysis 9 are useful only if results are acted upon to create more defences against errors. Ultimately, increased automation will reduce the role of people and therefore prevent opportunity for human error to occur. This has been shown to be successful, 10 but is expensive to implement and maintain.
We have explored the effects of two ward-based interventions to determine what effect they might have on preanalytical errors on inpatients. The first was a short-term poster with ward educational visits and the second a computer screen-saver.
Methods
The Leeds Bradford Pathology Partnership provides services to three teaching hospitals and primary care for a population of approximately 1.2 million. The laboratory protocols and venepuncture equipment are similar for all sites, with routine samples collected by phlebotomists and non-routine by doctors or nurses. Tests are requested via a paper-based ordering system and reports are returned through an electronic results server. There is a regular audit of errors in sample quality and identification, which shows that there are approximately 16,700 errors annually on inpatient samples.
Intervention 1
Posters were designed with blood-tube caricatures and limericks to raise awareness of the three main error types (insufficient sample volume, inappropriate tube selection and labelling or request form error) and the potential cost of such errors to the Trust. The aim of the posters was to be distinctive in a ward environment and to remind staff of the reasons for following phlebotomy protocol. Posters were displayed for two weeks in phlebotomy equipment storerooms and, where available, in the nurses’ and doctors’ rooms. St James’ University Hospital (SJUH) was selected as the intervention hospital while Bradford Royal Infirmary (BRI) and Leeds General Infirmary (LGI) were control hospitals. Each ward (
Intervention 2
Ten weeks after the interventions above, a screensaver reminding staff to correctly follow protocol in test requesting was displayed for 10 d on all computers in LGI and SJUH. The BRI was a control hospital.
Error recording
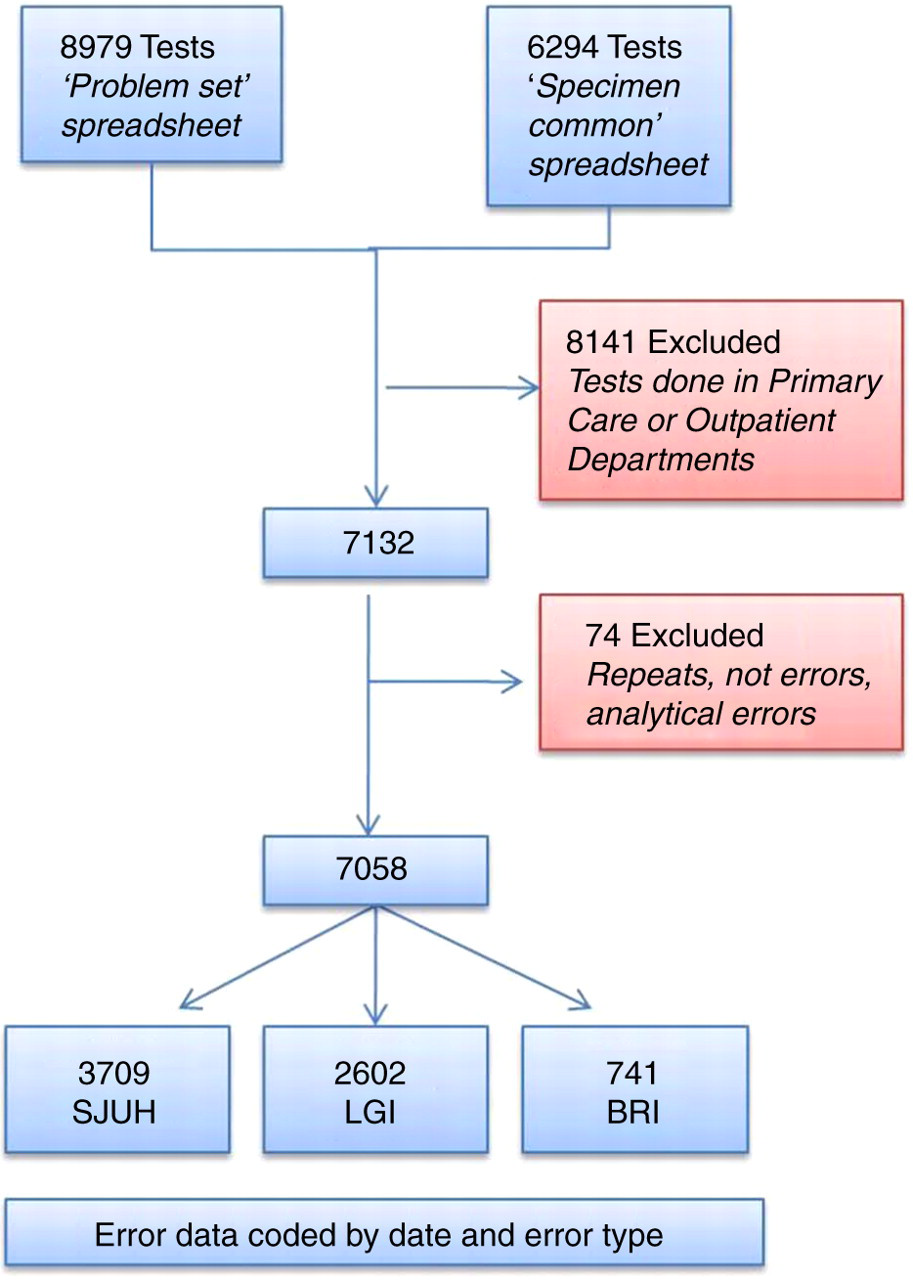
All test requests that cannot be processed are recorded in a laboratory database. Error data for SJUH, LGI and BRI were collated in two-week periods (A–K) from 13 September 2010 to 13 February 2011. The first intervention took place during period D and the second intervention took place during period J (Figure 1). A search of the laboratory computer was used to identify all samples with a specific problem. The data were sorted to remove errors from outpatient or primary care samples. The comments were reviewed and each entry was assigned a category. The categories included: no error, tube selection error, insufficient sample volume, labelling or request form error, no sample provided or miscellaneous error (Figure 2). All data were entered into a spreadsheet and statistical analysis was performed using the Analyse-it® add-in package (Version 2.10) for Microsoft Excel ( Error rate for the three hospitals. Inpatient error rate per request in two-week blocks for the three hospital sites. Period D was the poster and ward education intervention and period J was the computer screen saver. No significant change occurred in any time block. SJUH, St James' University Hospital; LGI, Leeds General Infirmary, BRI, Bradford Royal Infirmary Flow chart to show extraction of relevant data from laboratory computer records. SJUH, St James' University Hospital; LGI, Leeds General Infirmary, BRI, Bradford Royal Infirmary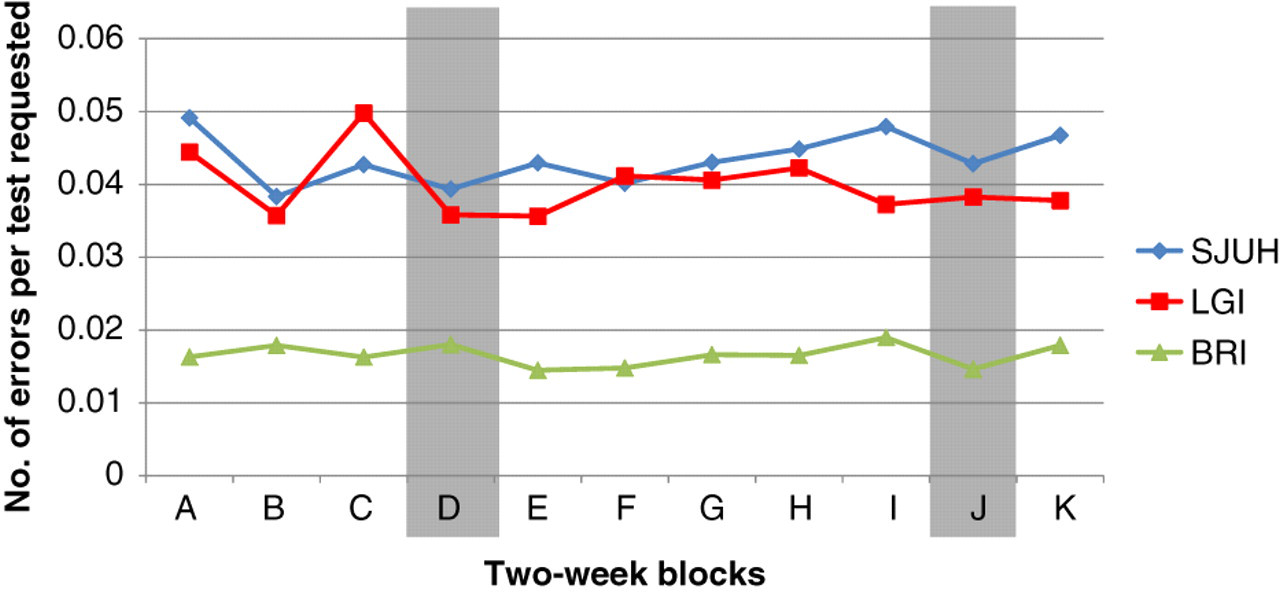
Results
There were 195,695 tests requested on inpatients at the three sites during the 22-week period. There were 7058 errors in the 22-week period (3709 from SJUH, 2602 from LGI and 747 from BRI). The overall error rates at SJUH, LGI and BRI were 4.4, 4.0 and 1.7%, respectively.
The majority of errors fell into one of the three groups targeted by the intervention: insufficient volume (5%), incorrect tube selection (or no sample received) (78%) and error on labelling or request form (11%). However, in Bradford, there was a notably lower error rate and very few volume errors. The mean error rate (% [SD]) per two-week block at SJUH was 4.35 (0.35), at LGI was 3.99 (0.44) and at BRI was 1.66 (0.15) (Figure 1). There was no statistically significant change in the frequency of errors over time (analysis of variance,
The qualitative discussions at SJUH yielded a good response (
Discussion
The findings of this report strongly suggest that intensive, short-term poster and screensaver interventions do not reduce errors in the preanalytical phase of laboratory testing. BRI and LGI were controls to ensure that variations in error rate were not due to seasonal changes. Staff at the BRI, LGI and SJUH are similarly trained and the hospitals have a similar range of wards and activities. However, there was little variation in error rates between intervention and control sites over the 22-week period and the expected reductions after interventions were not observed.
The posters targeted 94% of the errors which occurred during the study period. Posters were placed in clear view of staff, and the caricatures and limericks were recognized on subsequent visits; therefore, it can be assumed that a large proportion of phlebotomy staff were aware of the project. Despite focusing on appropriate themes and maintaining staff awareness, the intervention had no significant effect. The passively displayed screensaver intervention also made no significant difference to error rates in either hospital. While some studies have shown that long-term interventions can reduce error rates, 6,12 the time and intensity of intervention required (such as a year of continuous monitoring and education) is neither efficient nor feasible for large hospitals to implement. In addition, there is a significant chance that error rates would return to original levels after the intervention. Where errors are ‘simple human error’ and not a lack of education, an intervention is only effective when it interrupts the subconscious process to cause a staff member to consciously think about the details they are writing on the request card.
During discussions with clinical staff, many were unsure why tests were rejected and welcomed suggestions to improve practice. The two main themes were equipment problems and identifying the appropriate tubes for requested tests. Considering the predominance of tube errors (78%), phlebotomy training must cover tube selection, and promote online resources for information regarding rarer tests. Computerized order entry systems, used in some hospitals, have been shown to improve clinical efficiency and reduce preanalytical errors. 13–15 These systems could specify the tubes required and alert the laboratory when a rare test is requested, thus reducing the opportunity for incorrect tube selection. To avoid errors in phlebotomy technique, training must be specific to the equipment on the ward.
Mislabelled blood tubes or request forms were also a significant problem, contributing to 11% of the total errors recorded. This is a simple part of the process, yet a consistent problem and can have devastating results, particularly in transfusion. Introducing protocols to monitor ward staff when labelling specimens might be counterproductive: a recent study has shown that reducing the paperwork required for a transfusion match but ensuring the patient's ID is checked at the bedside, decreases the number of related errors. 16
Limitations
The interventions were carried out over short periods of time, during which it was impossible for two medical students to have a meaningful conversation with all staff involved in phlebotomy. This meant that awareness of the campaign was dependent on poster visibility and word of mouth. Poster placement varied due to the different ward layouts across SJUH, leading to variable penetrance of the intervention.
Another serious limitation was highlighted by the unexplained low error rate at BRI. Similar levels of staff training and comparable activity between wards suggest that this anomaly could be due to differences in error reporting or recording between Leeds and Bradford. In this case, there are implications for the validity of BRI as a control. However, the hospitals use the same error logging system, which has been in place for several years.
Conclusions
Despite enthusiasm on the part of the staff, both the poster and screensaver interventions had no significant impact on preanalytical error rates. The incorrect selection of blood tubes caused the majority of errors and must therefore be a focus for future improvements. Longer-term improvements to education may reduce error rates; however, time constraints and high workloads mean that human error will occur unless human input is eliminated by automation.
DECLARATIONS