
Abstract
Background
Timely detection of acute kidney injury (AKI) in hospital patients has been hampered by the multiple definitions of AKI and difficulties applying their criteria. A laboratory delta check may provide an effective means of detecting patients developing AKI. This study compared three of the proposed AKI definitions and a delta check to detect AKI using serum creatinine results of hospital inpatients.
Methods
Serum creatinine results for 2822 inpatients were gathered retrospectively from the clinical biochemistry database. All serum creatinine results within 30 d of admission were included for each patient and assessed for AKI according to four criteria: Risk, Injury, Failure (RIFLE), Acute Kidney Injury Network (AKIN), Waikar & Bonventre or a delta check (increase of >26 μmol/L between two successive values).
Results
A total of 149 (11.3%) patients were defined as having AKI by at least one of the four criteria. Different populations of patients were identified by each criterion. The number of patients identified and the incidence of AKI were as follows: RIFLE 94 (7.1%), AKIN 125 (9.5%), Waikar & Bonventre 100 (7.6%) and delta check 146 (11.1%). The delta check detected 132 (98%) of all 135 cases detected by the other three criteria. A further 14 patients were detected solely by the delta check.
Conclusions
The different definitions proposed for AKI detect different populations of patients. A laboratory delta check detected 98% of all the patients identified by AKIN, RIFLE and Waikar & Bonventre combined and could therefore provide a practical way of detecting AKI patients.
Introduction
Acute kidney injury (AKI) is associated with significant morbidity and mortality. The National Confidential Enquiry into Patient Outcome and Death (NCEPOD) Adding Insult to Injury report on AKI found that there was an unacceptable delay in recognizing AKI in 43% of patients who developed the condition postadmission. 1 This clearly illustrates the need to improve the detection of AKI in hospitalized patients.
Outlines the definitions for AKI in accordance with RIFLE, AKIN and Waikar & Bonventre, respectively
AKI, acute kidney injury; sCr, serum creatinine
A delta check is an automated alert system employed by laboratories to detect potentially erroneous results. This system compares each new result with the previous result for the same patient and flags when the difference between the two exceeds specified limits. Although it was originally designed to detect laboratory errors such as mislabelled samples, 6 a delta check also has clinical utility when used to detect clinically significant changes in patient results.
The purpose of this study was to compare three of the proposed definitions of AKI (RIFLE, 3 AKIN 4 and Waikar & Bonventre 7 ) by applying their criteria to hospital patient creatinine results. In addition, the performance of a delta check to identify these AKI patients was assessed.
Methods
The laboratory clinical biochemistry database was interrogated to gather retrospectively all serum creatinine results for adult (≥18 y) inpatients admitted to Leeds General Infirmary (880 inpatient beds) during the calendar month of October 2008. Only inpatients were included and the data did not include patients admitted to renal wards (renal wards are located on a sister hospital site). Serum creatinine was measured using the O'Leary modified Jaffe method (Audit Diagnostics, Carrigtwohill, Ireland) on the Siemens Advia 2400 (Siemens Healthcare, Surrey, UK) with typical inter-assay coefficient of variation of 3.3% at 64 μmol/L and 2.1% at 520 μmol/L creatinine. All serum creatinine results for these patients reported within 30 d following the day of admission were collected. The data were analysed using the RIFLE, AKIN and Waikar & Bonventre criteria (Table 1). The baseline creatinine was defined as the lowest creatinine within seven days (RIFLE) or 48 h (AKIN) of an increase in creatinine (i.e. a rolling baseline creatinine). In addition, the data were analysed using a delta check criterion defined as an increase of >26 μmol/L (in accordance with AKIN criteria 4 ) between two successive serum creatinine results over a period of 30 d. For the purposes of this study, a patient was defined as having AKI if they met the criterion of any of the three definitions in Table 1 or if they triggered a delta check alert. Data were analysed using Microsoft Excel software 2002.
Results
A total of 8373 patients were admitted to Leeds General Infirmary during October 2008 and following exclusions, 5565 adult inpatients were identified for analysis (Figure 1). Of these 5565 patients, 2822 (51%) had serum creatinine measured, accounting for a total of 10,019 creatinine results. These 2822 patients consisted of 1401 men and 1421 women and had a median age of 61 years (range 18–98 y).
Flow diagram to illustrate number of patients included in the study and their respective serum creatinine results. AKI patients defined as those that met any of the four criteria outlined in the Methods section. AKI, acute kidney injury; sCr, serum creatinine, RI, reference interval, URL, upper reference limit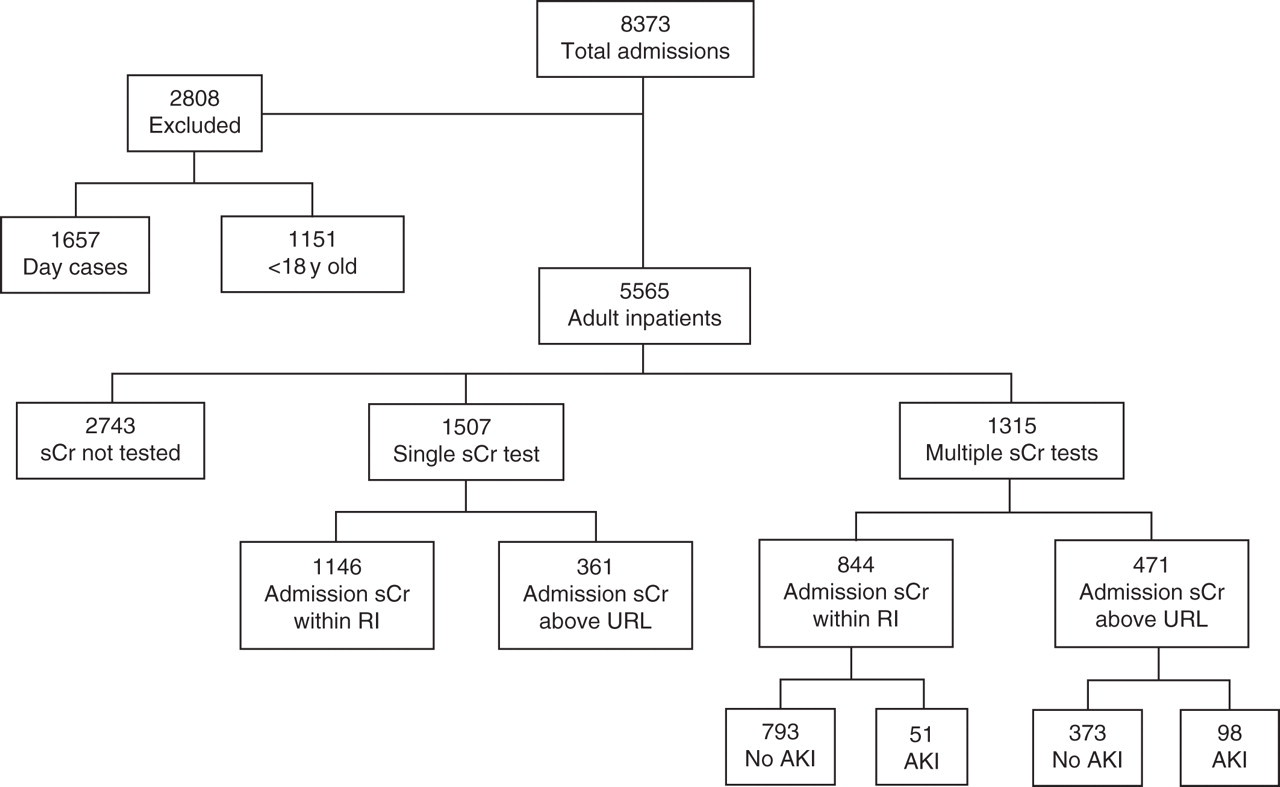
The admission creatinine results of the 2822 patients ranged from 47–1063 μmol/L, with 832 patients (29%) having serum creatinine concentrations above the upper reference limit on admission (>110 μmol/L for men, >100 μmol/L for women). However, 1507 of the 2822 patients had only a single creatinine result and therefore could not be assessed for AKI using the proposed criteria, which require at least two serum creatinine results.
Of the 1315 patients who had multiple creatinine results, 149 (11.3%) were identified as potentially suffering from AKI in accordance to either the RIFLE, AKIN, Waikar & Bonventre or delta check criteria. These 149 patients consisted of 73 men and 76 women and had a median age of 75 years (range 22–95 y). Admission serum creatinine for these patients ranged from 47 μmol/L to 1063 μmol/L, with 98 patients (65.8%) being above the upper reference limit. Using all four criteria, AKI was detected within 48 h of admission in 36 patients (24%) but the median was six days (range 1–30 d).
The number of patients identified by each of the four criteria are shown in Figure 2. When the RIFLE, AKIN and Waikar & Bonventre criteria were combined, they identified 135 patients and the laboratory delta check identified 132 (98%) of all these cases. In addition, the delta check identified a further 14 patients not detected by the other three criteria. The incidence of AKI among the 1315 patients with multiple serum creatinine results was 7.1% using RIFLE, 7.6% using Waikar & Bonventre, 9.5% using AKIN and 11.1% using the delta check criterion.
A Venn diagram to show the distribution of AKI patients detected by RIFLE, AKIN, Waikar & Bonventre and delta check criteria. AKI, acute kidney injury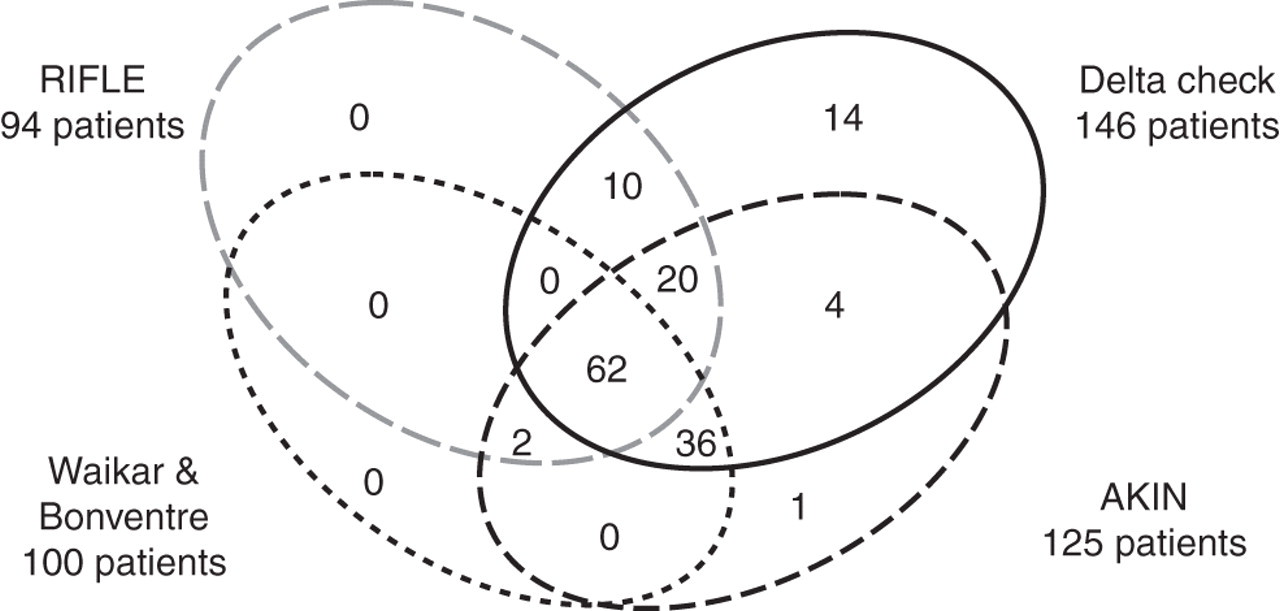
Number of patients at each stage of AKI according to RIFLE, AKIN and Waikar & Bonventre criteria are shown
AKI, acute kidney injury
Discussion
AKI is now recognized as a spectrum of injury and can be difficult to identify clinically in its early stages in hospitalized patients as the clinical features may not be recognized beyond those of the admission illness. The aspiration is that the introduction of new definitions based on relatively small but significant rises in serum creatinine will help in the identification of AKI at an earlier stage. However, recognition of patients developing AKI can be further hampered by the multiple definitions of AKI and difficulties in applying their criteria to current biochemistry automated systems. This study compared three of the proposed AKI definitions and a delta check to detect AKI using serum creatinine results of hospital inpatients. The results suggest that different populations of AKI patients are detected by each definition and that a delta check could provide an effective way of detecting all these patients.
Collectively, RIFLE, AKIN, Waikar & Bonventre and the delta check identified 149 AKI patients out of a population of 1315 patients (11.3%). In accordance with previous studies, 8,9 these patients were predominantly elderly and both men and women appeared to be affected equally. AKI can occur in patients of all specialties, 1,8,9 and this is reflected in the results of this study where the AKI patients were admitted to a total of 17 different specialties.
The delta check detected the highest number of patients (146) and these included all but three (2%) of the patients identified by the other criteria combined. These three patients were not detected by the delta check because they had frequent creatinine measurements within a short period of time so that each successive result showed an increase less than 26 μmol/L, even though the total increase was greater than this over 48 h.
A group of 14 patients were detected solely by the delta check. These patients had a period greater than 48 h between repeat serum creatinine measurements and therefore could not be detected by the AKIN or Waikar & Bonventre criteria despite a rise in creatinine >26 μmol/L. Further investigation is required to determine whether such patients are likely to be suffering from AKI.
An increase in creatinine of 26 μmol/L was used for the delta check criterion in this study because this is the increase used in both the AKIN and Waikar & Bonventre definitions of AKI. This relatively small increase in serum creatinine had previously been found to be associated with a 4.1 increased odds ratio of mortality in hospitalized patients. 10 However, when such a modest increase in creatinine is being used to define AKI, consideration needs to be given to factors that cause fluctuations in serum creatinine. One important factor is the consumption of a meat meal, which has been shown to increase serum creatinine by 20.5 μmol/L within 1–2 h. 11 Other factors include biological and analytical variation. Reference change values (RCV) can be used to determine whether changes in serum creatinine are statistically significant by accounting for biological and analytical variation. 12,13 In health, the biological variation of creatinine has been reported at 5.3% 14 and the analytical variation of the modern creatinine assay is approximately 5%. 15 Using these values to calculate the RCV for a unidirectional change (rise) in creatinine with 95% probability (Z score = 1.65) would give an RCV of 17%. Therefore, a rise of 26 μmol/L in serum creatinine would be considered significant as long as the patient's baseline creatinine was below 153 μmol/L. However, for a patient with a serum creatinine above 153 μmol/L, a rise of 26 μmol/L would be within 17% and therefore could be due to biological and analytical variation. Furthermore, for a patient with a baseline creatinine below 153 μmol/L, increases in creatinine that are less than 26 μmol/L would be significant and therefore could potentially be indicative of AKI. In addition, the fact that these criteria are being applied to acutely ill patients requires consideration. Although it has been reported that the biological variation of most analytes in stable chronic diseases does not significantly differ from that in health, 16 it is less clear as to whether this is true for acute illnesses. For example, one study found that the biological variation of serum creatinine increased to 13.4% in myocardial infarction patients, 17 giving an RCV of 33%. The adoption of a serum creatinine RCV could potentially provide a more efficient means of detecting AKI patients, but further research is required to determine whether this will identify the patients in whom outcomes can be improved.
The RIFLE, AKIN and Waikar & Bonventre definitions of AKI have been proposed as a means to classify AKI and determine the incidence of this condition. However, applying these definitions to detect patients developing AKI during hospital admission has practical limitations. 18 For example, RIFLE and AKIN both require the use of a baseline creatinine, but such information is not readily available for hospital doctors and difficulties in determining this value prevents their incorporation into automated systems. Furthermore, AKIN and Waikar & Bonventre criteria both require repeat serum creatinine results within 48 h and therefore cannot be applied to patients that have had a longer interval between repeat tests. In contrast, a delta check is simple to apply and it can be easily integrated into the laboratory computer system to provide an automated method to detect patients developing AKI during their hospital admission.
Conclusion
The different definitions proposed for AKI detect different populations of patients. A laboratory delta check detected 98% of all the patients identified by AKIN, RIFLE and Waikar & Bonventre combined and could therefore provide a practical way of detecting patients developing AKI.
DECLARATIONS