
Abstract
Background
Spurious hyperkalaemia is a well-recognized problem when reporting potassium results in samples originating from Primary Care. This is particularly relevant in laboratories serving large geographical areas where sample transport can cause significant delays in sample centrifugation. We have carried out a retrospective audit comparing serum potassium results on samples centrifuged at the general practice (GP) with those centrifuged on arrival at the clinical laboratory.
Methods
Potassium results were reviewed on serum samples received from 87 GPs in the Grampian region between August 2010 and March 2011. Potassium results were compared between samples centrifuged at the practice versus those centrifuged on arrival at the clinical laboratory.
Results
In the period between November 2010 and February 2011, median monthly serum potassium results were significantly different between samples centrifuged at practices and those centrifuged on arrival at the laboratory. Median potassium concentrations were 10.2% higher in January 2011 (4.8 mmol/L; interquartile range [IQR]: 4.5–5.1) compared with August 2010 (4.3 mmol/L; IQR: 4.0–4.6). A similar trend in monthly median potassium concentrations was not evident in samples centrifuged at source over the same period.
Conclusions
The introduction of centrifuges into all GPs across NHS Grampian has significantly reduced the effect of seasonal variation in serum potassium results. There has also been a concurrent reduction in the number of cases of spurious hyperkalaemia. This exercise has significantly improved the overall quality of potassium results reported to Primary Care.
Introduction
Spurious hyperkalaemia is experienced daily in many laboratories. It occurs when elevated serum potassium concentrations are not explained by the clinical picture and normalize with repeat analysis on a fresh sample without the requirement for clinical intervention. Hyperkalaemia is a cause of cardiac arrest and arrhythmias, highlighting a requirement for production of valid results to prevent life-threatening clinical action or inaction. Therefore, true and spurious results need to be identified in a timely manner.
In the Primary Care setting, spurious hyperkalaemia can lead to avoidable emergency referrals to acute medical assessment units and unnecessary distress to patients. This can be a particular problem outside routine laboratory hours when full clinical details may not be available. 1 The main causes of spurious hyperkalaemia are well documented and include thrombocytosis, ‘leaky cell syndrome’ and preanalytical variables (haemolysis, temperature and delays in separation). 2 The latter is a considerable issue with samples sent from Primary Care.
The Clinical and Laboratory Standards Institute recommends that serum samples are centrifuged within two hours of venepuncture to ensure the integrity of most analytes. This guidance is supported by several studies showing that potassium is affected by temperature 3–7 and delays in separation of serum from cells. 4,8–10
NHS Grampian covers an area of approximately 8700 km2 and serves a population of 525,000. The timely transport of samples to the laboratory is a challenge. The 87 general practices (GPs) that use the laboratory service based at Aberdeen Royal Infirmary (ARI) are situated up to 60 miles away and generally samples are only collected once daily. Therefore, spurious hyperkalaemia is a frequent occurrence. One effective strategy to prevent spurious hyperkalaemia is to ensure the collection of blood samples for biochemistry analysis into gel separator tubes followed by timely centrifugation at the requesting GP practice site. 10 In 2010, the Biochemistry Department at ARI actively engaged with Primary Care users promoting the benefits of on-site centrifugation as a quality improvement initiative that would benefit GPs, the laboratory and ultimately the patient.
Methods
All serum potassium requests received from Primary Care between August 2010 and March 2011 were reviewed. Those blood samples were collected into BD Vacutainer® SST™ II Advance gel tubes (Becton Dickinson, Franklin Lakes, NJ, USA). Samples were divided into two groups: those that had been centrifuged at source (n = 109,177) and those that had not been centrifuged prior to arrival at the laboratory and were >4 h old (n = 51,935). A four-hour cut-off was used as a pragmatic approach that GP surgeries would find acceptable and workable. The manufacturer's guidelines state that serum samples collected into serum separating tubes are stable for 24 h at room temperature and seven days at 2–8°C. The data were not normally distributed. Monthly median serum potassium concentrations in each group were compared by Kruskal–Wallis test and Mann–Whitney U test. Over the duration of the audit there was a dramatic increase in the number of samples being centrifuged at source, rising from 20% to 95%.
Results
In samples centrifuged on arrival at the clinical laboratory over the eight months from August 2010 to March 2011, monthly transport times were constant over the eight-month period (interquartile range [IQR]: 8 h 50 min to 10 h 15 min). This compared with samples centrifuged at the GP, where the median transport time was 10 h 16 min (IQR: 9 h 58 min to 12 h 55 min).
Samples centrifuged on arrival at the clinical laboratory exhibited a maximum of 10.2% increase in median serum potassium concentrations (P < 0.0001; n = 51,935), between August 2010 (4.3 mmol/L; IQR: 4.0–4.6) and January 2011 (4.8 mmol/L; IQR: 4.5–5.1). This variation in potassium was observed in the context of a concurrent decrease (−11°C) in ambient temperature in the Grampian region over the same time period (Figure 1). According to the method of Fraser and Harris, 11 the reference change value at 95% probability is 10% at serum potassium concentration 5 mmol/L. Consequently, the 10.2% increase in potassium observed would be deemed clinically significant.
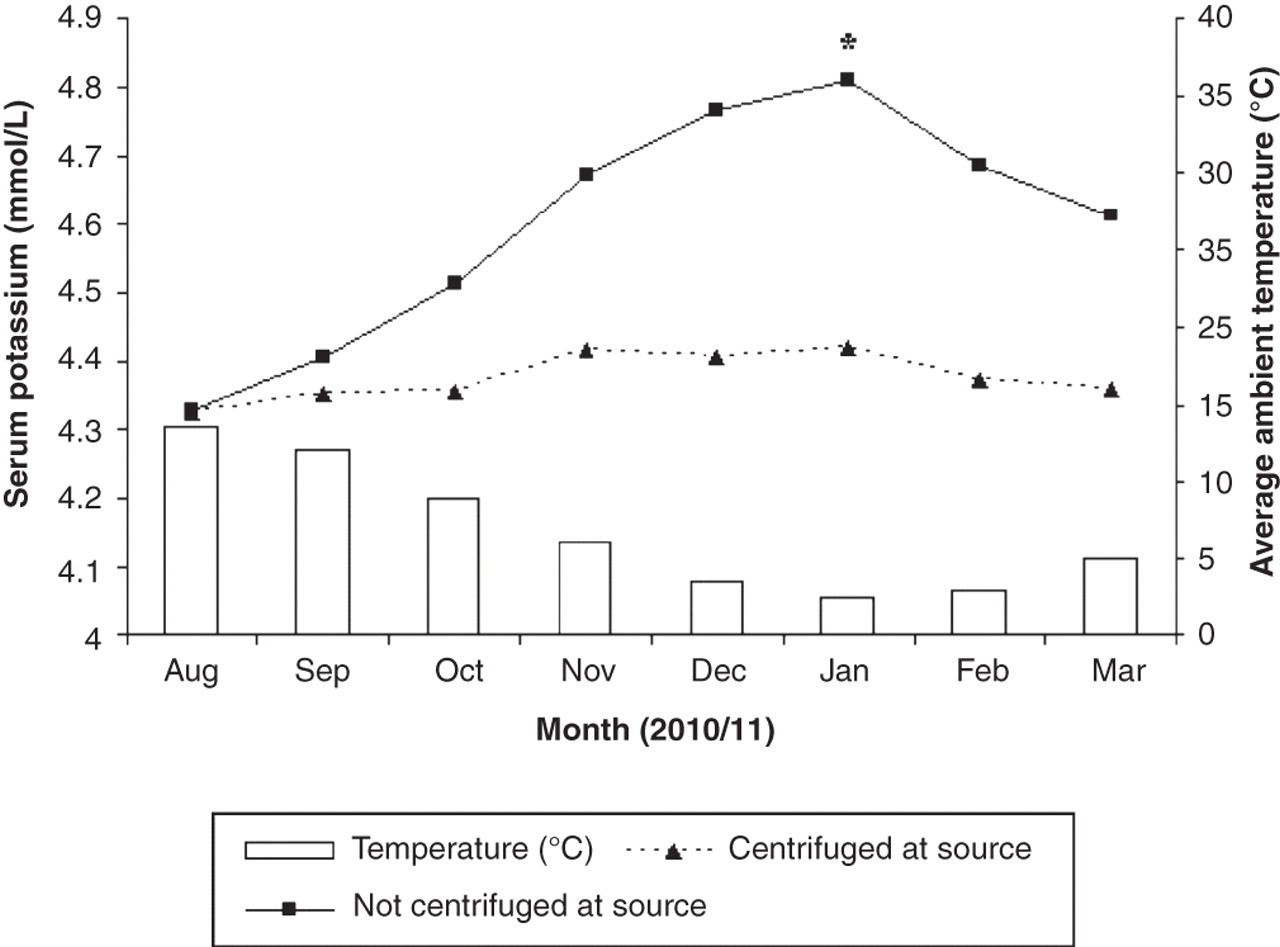
Comparison of monthly median potassium concentrations between samples centrifuged at source and those not centrifuged at source. Monthly median serum potassium concentrations in samples centrifuged at their source in Primary Care (n = 109,177) are compared with the equivalent data from samples centrifuged on arrival at the clinical laboratory (n = 51,935). The corresponding monthly average temperatures (°C) in the Grampian region for 2010/2011 are also displayed.
14
A similar trend in serum potassium concentrations was not observed in samples centrifuged at source, exhibiting a 2.3% increase in median serum potassium concentrations between August (4.3 mmol/L; IQR: 4.1–4.6) and December 2010 (4.4 mmol/L; IQR: 4.1–4.6). Although this change was statistically significant (P < 0.0001; n = 109,177), it corresponds to a 0.1 mmol/L increase in serum potassium concentration, and is therefore unlikely to be of clinical significance.
The largest discrepancy in sample potassium results between those samples centrifuged at source and centrifuged at the laboratory occurred in January 2011, where the average daily temperature was coldest (2.5°C). During this month, the median potassium concentration for samples centrifuged at the laboratory was significantly higher (4.8 mmol/L; IQR: 4.5–5.1) than that observed on equivalent samples centrifuged at source (4.4 mmol/L; IQR: 4.1–4.6; P < 0.0001). In August 2010, the average daily temperature for the region was 13.5°C. During this month, the difference was minimal (<0.01 mmol/L) between samples centrifuged at source and those centrifuged at the laboratory. Although this was a marginally statistically significant change (P = 0.041; n = 161,112), it is of minimal practical significance.
Discussion
These results clearly demonstrate the improvement in sample quality with respect to serum potassium concentrations when samples are centrifuged at source. In addition to the overall quality of results, the use of centrifuges in GPs has minimized the variation in potassium concentrations as the ambient temperature changes.
Spurious hyperkalaemia can cause major concern for GPs. Delays in sample separation is a well known cause for elevating serum potassium results. 2,3 The effect is exaggerated in winter months when ambient temperature falls, causing an elevation in serum potassium concentrations. 5–7,12 This can lead to difficulties in determining the difference between cases of hyperkalaemia requiring urgent attention and those that are artefactual.
Several options have been proposed to eliminate spurious hyperkalaemia with centrifugation of samples at point of collection being the most common. Stahl and Brandslund 13 showed that if samples were maintained at a temperature of 20–21°C, serum potassium concentrations remained stable for up to eight hours. They subsequently proposed that centrifugation of samples at source was no longer necessary. The obvious flaw in this approach is the difficulty in maintaining temperatures within this tight range. The challenges associated with transporting samples over large distances means that for a great number of laboratories throughout the UK, this is not a practical solution.
As well as an improvement in the quality of samples being received from GP practices, we have also had positive feedback from our users that the use of centrifuges has increased the flexibility of the phlebotomy service they offer. Users have greater flexibility in their sampling regimens throughout the day, making it easier for patients to arrange appointment times. Previously, samples could only be collected at rigid daily time points, severely limiting the phlebotomy service provided. The use of centrifuges in Primary Care has also served to expand the repertoire of tests available to GPs, including those requiring rapid centrifugation of the sample that were previously unsuitable (e.g. trace metals, parathyroid hormone). Adverse winter weather conditions in NHS Grampian have severely affected the transport of samples, often taking several days to reach the laboratory, rendering many unsuitable for analysis. The introduction of Primary Care centrifugation has largely eliminated this problem. In addition to advantages to Primary Care, the laboratory has also benefited from this initiative. We have been able to streamline processes in sample reception, resulting in more efficient sample workflow. Prior to the introduction of centrifugation at source, the vast majority of GP samples arriving at the laboratory in the evening were centrifuged offline, a time-consuming process. This meant that a significant proportion of samples was not analysed until the next day, delaying results and possible treatment of patients. As the majority of samples are now centrifuged prior to arrival, the handling time in reception is markedly reduced and enables more samples to be analysed and resulted the same day.
The undoubted benefits of introducing sample centrifugation in Primary Care are obvious. However, the process has not been without its problems. In 2008, centrifuges were purchased for the majority of practices by NHS Grampian, with a significant number of practices being omitted from the original procurement. Therefore, in 2010, agreement had to be sought from the three individual Community Health Partnerships (CHPs) to fund provision of centrifuges for the remaining practices. There was initial concern from the GP practices regarding several issues such as noise, training, health and safety. These were largely addressed by staff from the Department of Biochemistry, who offered training sessions to all users. Guidance documents were produced by the laboratory and the infection control and prevention team to cover general use and health and safety, respectively. An agreement was sought on how best to maintain and service the centrifuges and several options were suggested. Ultimately, the CHPs agreed to fund any necessary repair requirements. We are aware that the process will need continued monitoring and re-education of users as required, but the overall improvement in sample quality counteracts the staff time involved.
We have described the successful widespread introduction of centrifugation to Primary Care in the Grampian region. Pathology services are encouraged to reconfigure services in line with clinical need. Primary Care centrifugation has a stabilizing effect on samples, providing greater flexibility in transporting samples between sites, making the centralization of non-urgent ‘cold’ work a viable pathology model. The practical and clinical advantages with regard to the reporting of serum potassium results have benefited GPs, the laboratory and, most importantly, the patient. The success of this implementation has been reliant on good communication between the laboratories, GP and the CHPs.
DECLARATIONS