
Abstract
Cocaine is a drug notorious for its ability to adversely affect almost any organ in the body and cause a plethora of biochemical abnormalities secondary to its severe vasoconstrictive properties. These abnormalities are not exclusively seen in habitual users or cases of overdose, and may sometimes cause confusion as to the underlying pathology. We describe a case of a young female who presented to the Accident and Emergency department in the early hours of the morning complaining of muscle weakness following the inhalation of a small quantity of an ‘unknown substance’ the previous night. Investigations showed life-threatening hyperkalaemia with a potassium of 9.0 mmol/L, evidence of rhabdomyolysis, acute renal as well as liver failure, disseminated intravascular coagulopathy and a raised troponin of 7000 ng/L, which later peaked to 15,600 ng/L. Four days later, she became hypoxic as a result of adult respiratory distress syndrome with grossly abnormal chest X-ray appearances. Following intensive therapy, she made a dramatic recovery and was discharged from hospital 20 days from presentation. This case highlights the importance of biochemical profiling in patients presenting with possible drug use, even in the absence of significant symptoms.
Introduction
Cocaine overdose can manifest not only with pronounced central nervous system effects, but also has recognized cardiotoxic, and to a lesser extent hepatotoxic, effects as well as producing rhabdomyolysis which may culminate in acute renal failure. 1–3 These systemic effects are predominantly the result of the severe vasoconstrictive properties of this drug. 4 We describe here the case of a young female who appears to have been exposed to cocaine for the first time and presented with severe life-threatening hyperkalaemia following rhabdomyolysis and acute renal failure, as well as ischaemic hepatitis, lung complications and significantly raised troponin I.
Case report
A young female presented to the Accident and Emergency (A&E) department, previously well and on no regular medications. She had been socializing the previous night and was introduced to an ‘unknown substance’ in the form of a white powder which she claimed to have inhaled in a small quantity. She presented complaining of weakness and pain in her quadriceps muscles. There was no history of vomiting or diarrhoea nor headache or photophobia. There was also no history or clinical evidence of physical trauma and the patient denied being on any medications or having any previous medical history. At the time of presentation, she had a Glasgow Coma Scale 15/15, chest was clear to auscultation, heart sounds were normal and abdomen was soft with no organomegaly.
Urine by dipstick tested strongly positive for blood and protein. Blood gases showed a metabolic acidosis with pH 7.22, lactate 6 mmol/L and a raised anion gap of 18.7 mmol/L. Analysis of venous blood at presentation showed a profound life-threatening hyperkalaemia, potassium being 9 mmol/L, as well as a very high phosphate of 4.33 mmol/L with a subsequently low albumin-adjusted calcium concentration. The biochemical profile of this patient on admission is indicated in Table 1. Significantly raised serum creatine kinase of over 8000 IU/L and high urea and creatinine suggested acute renal failure secondary to rhabdomyolysis. Total protein and albumin levels were normal; however, transaminases surged to almost 100 times the upper reference limit, with an acutely raised ferritin of 27,004 μg/L, consistent with acute hepatic necrosis. Her international normalized ratio (INR) was initially 1.85 and peaked to 3.0 within a few hours (Figure 1). Alkaline phosphatase and gamma glutamyl transferase concentrations were both within the reference range. Hepatitis viral serology was negative. Her platelets dipped to a low of 71 × 109/L on day two. Salicylate and paracetamol were not detected in the serum. A urinary drug screen was negative for opiates, amphetamines benzodiazepine and barbiturates, but positive for cocaine. Her measured osmolality was 292 mmol/kg (similar to her calculated osmolality); hence, there was no significant osmolar gap to suggest the presence of any ethanol or toxic alcohols in her blood. Her troponin I concentration was 7000 ng/L on day 1 and peaked to 15,600 ng/L on day 2. An electrocardiogram initially showed changes compatible with hyperkalaemia, in the form of tented T waves and subsequently T-wave inversion, which later resolved. An echocardiogram showed evidence of normal left ventricular size with normal wall thickness, moderate systolic function but which was described as somewhat stiff. An abdominal ultrasound the day after her admission to hospital showed ascites and bilateral pleural effusion.
Trends of international normalized ratio (INR), aspartate aminotransferase activity and phosphate and potassium concentrations (from above downwards) from the time of admission to the emergency department Biochemical investigations at the time of admission to hospital eGFR, estimated glomerular filtration rate; AST, aspartate aminotransferase; ALT, alanine aminotransferase; CK, creatine kinase; LDH, lactate dehydrogenase; INR, international normalized ratio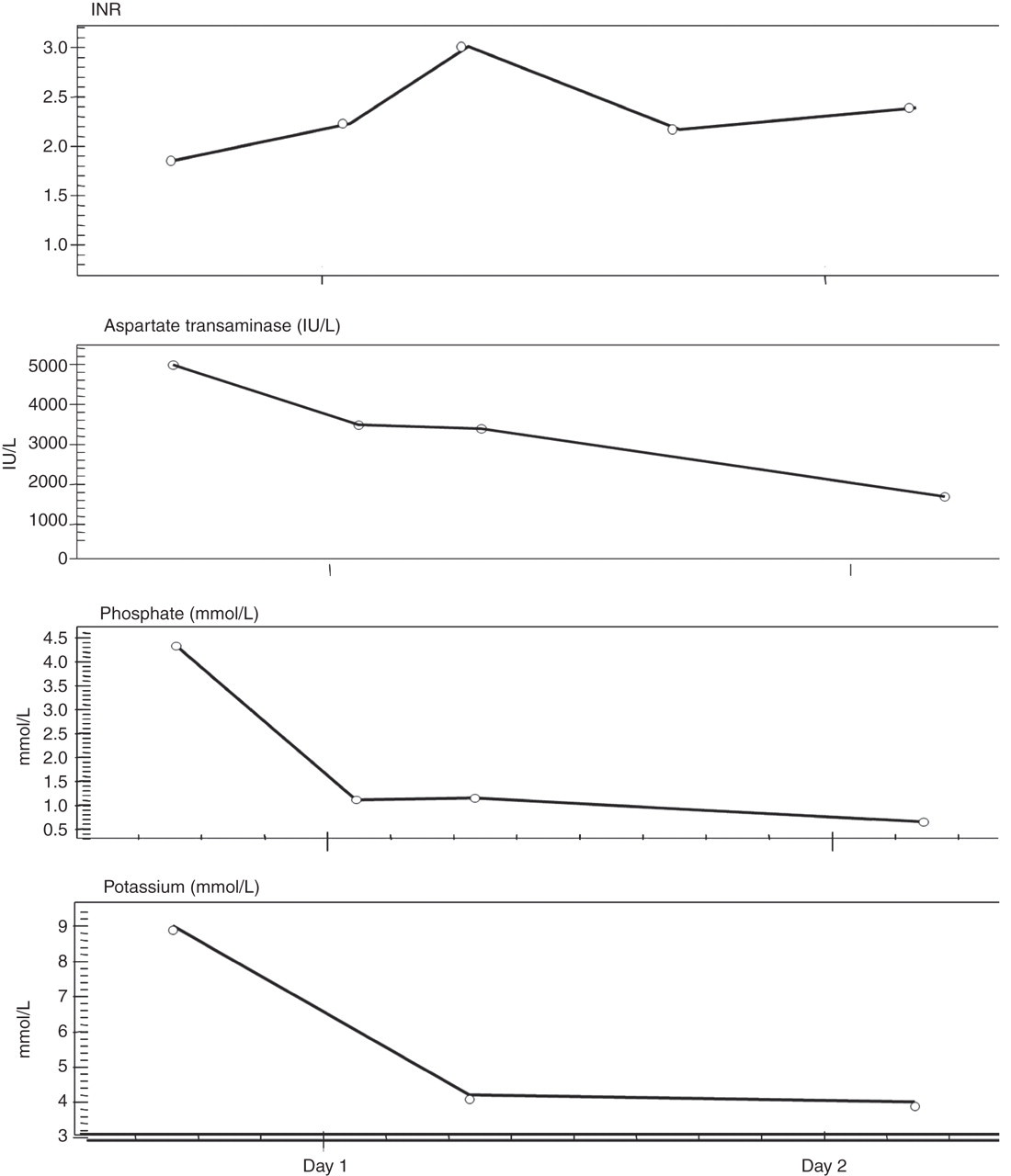
Emergency management of her hyperkalaemia consisted of an infusion of calcium, insulin and glucose and aggressive fluid resuscitation resulting in resolution of her initial hypotension at presentation. She was admitted to the intensive care unit (ITU) for further management of her biochemical and metabolic abnormalities. In view of her acute liver failure, she was treated with N-acetlycysteine and required renal replacement therapy in the form of continuous veno-venous haemofiltration for a period of 48 h. At no time did she become significantly encephalopathic and arterial ammonia remained normal. Within a few days there was evidence of significant improvement in her condition and she was subsequently transferred to a non-acute ward.
Three days later, she became febrile and developed dyspnoea and was diagnosed with hospital-acquired pneumonia and adult respiratory distress syndrome (ARDS). A chest X-ray showed dense bilateral air space opacification and she was transferred back to the ITU where she was treated with continuous positive airway pressure and antibiotics. She made a good recovery and was discharged back to the non-acute ward two weeks later. Her liver and kidney function tests, as well as her electrolytes, all returned to normal. Three days following this, she was discharged from hospital.
Discussion
Cocaine ingestion may be associated with a range of complications, encompassing cardiac, neurological, gastrointestinal, renal and psychiatric. 4 However, there exists a commonly held, but unsubstantiated, notion that cocaine-related complications and deaths are due to drug overdose. Its toxicity cannot be predicted from blood cocaine levels, and similarly death is not dose-related, with the exception of drug couriers (body packers) who have been massively exposed to the drug. 1
We have described here the case of a young female who appears to have been exposed to an unknown quantity of cocaine for the first time. Her biochemical abnormalities on presentation reflected a substantially life-threatening profile as well as evidence of multiorgan failure. The coexistence of severe hyperkalaemia with a significantly raised troponin was alarming, particularly with a background of renal and liver failure. The raised potassium in this patient was primarily the result of rhabdomyolysis and the subsequent acute renal failure, which is known to occur after cocaine use. 3 Troponin I has been reported to be falsely raised in about 17% of patients with rhabdomyolysis. 5 However, the specificity of cardiac troponin I was found to be unaffected by recent cocaine use in studies which examined patients presenting to A&E with chest pain, while that of myoglobin was reported to be significantly affected in the same cohort of patients. 6,7 Hence, myocardial ischaemia with subsequent microinfarcts cannot be excluded in our patient in light of the extreme vasoconstriction which culminated in the acute multiorgan failure. Cocaine binds to transporter proteins and blocks the reuptake of monamine neurotransmitters dopamine, norepinephrine and serotonin, resulting in the increase of their synaptic concentrations which produces the potent vasoconstrictor effect. 8 Cocaine also induces an increase in the principal determinants of myocardial oxygen demand: the heart rate, the systemic arterial pressure and left ventricular contractility. At the same time, the ingestion of even small amounts of the drug causes vasoconstriction of the coronary arteries. 9 The occurrence of cardiac complications after cocaine use has therefore been reported to be irrelevant to the amount ingested, the route of administration and the frequency of use. 10
Rhabdomyolysis was the main precipitant for the renal failure in this patient; yet the intense vasoconstriction that resulted in acute liver failure could have either triggered or exacerbated the renal failure. The rhabdomyolysis and acute renal failure produced the picture of severe hyperkalaemia and hyperphosphataemia seen in this patient. Approximately 24% of cocaine users have been reported to develop rhabdomyolysis. Many of these cases are not predictable from history or physical examination, making laboratory evaluation essential. 11
The patient was found to have pleural effusion on admission and she eventually developed hospital-acquired pneumonia and ARDS. Although habitual cocaine smoking can produce subtle long-term pulmonary consequences due to chronic alveolar epithelial and microvascular lung injury, single cocaine use (particularly crack cocaine) can lead to a variety of acute pulmonary complications, including an acute lung injury syndrome associated with a broad spectrum of histopathological changes. 12
The acute liver failure in this patient evidenced by significantly raised transaminases, lactate dehydrogenase, ferritin and INR, resolved completely within the first week of admission. Moreover, her renal function returned to normal within two weeks and she essentially made a complete and dramatic recovery following intensive treatment, with no evidenced of residual damage to any of her organs.
Despite the array of medical complications that arose in this patient following cocaine use, she was not only relatively asymptomatic, but also neurologically and mentally intact. There have been common reports of seizures and pathological behaviours, including psychosis among habitual cocaine users, as well as rare reports of excited delirium, which may be particularly associated with the occurrence of rhabdomyolysis. 13,14 The lack of such findings may support the patient's claim that she was a first-time user.
This case represents a rare and unexpected outcome of cocaine toxicity, given the grossly abnormal and life-threatening biochemical picture at presentation despite the lack of severity of her symptoms. The full recovery of this patient highlights the importance of early detection of the underlying biochemical derangements in suspected cocaine abuse and their subsequent management by intensive therapy.
DECLARATIONS