
Abstract
Background
Falsely decreased serum alphafetoprotein (AFP) concentrations are reported in the autoDELFIA® hAFP immunoassay due to interference by complement. AFP is measured, using this assay, as part of second-trimester and integrated Down's syndrome screening tests. Decreased AFP concentrations increase the calculated risk of Down's syndrome; therefore falsely low AFP, due to assay interference, may artificially increase a patient's risk, and have the potential to cause false screen positive results. It was our aim to assess whether negative interference in the autoDELFIA® hAFP assay was a cause of very low AFP concentrations, and to examine the effect of falsely decreased concentrations on the calculated risk of Down's syndrome.
Methods
Three hundred and twenty-three sequential Down's screening serum samples with very low serum AFP concentration (<15 KU/L) using the autoDELFIA® hAFP immunoassay were selected and AFP re-measured using the E170 AFP immunoassay.
Results
Interference was detected in nine samples (from eight patients) on the basis of discordant AFP concentrations. The interference decreased following storage of samples at 4°C to deplete complement. Use of the falsely low AFP concentrations to calculate risk of Down's syndrome resulted in significantly increased calculated risk compared with complement depleted results.
Conclusions
Laboratories should be aware that falsely low AFP concentrations due to complement interference may be obtained using the autoDELFIA® hAFP immunoassay. We have shown that falsely low AFP concentrations increase the calculated risk of Down's syndrome. This is a potential cause of false Down's syndrome screen positive results.
Introduction
Interference in immunoassays due to endogenous proteins is well described 1,2 and can lead to unnecessary medical intervention when unrecognized. 2 Identification of spurious immunoassay results due to interference generally requires good liaison between clinicians and laboratories so that when immunoassay results do not agree with clinical findings, appropriate laboratory investigations can be undertaken to identify the cause. 3 Interference in immunoassays can be more difficult to identify in the setting of screening programmes, 4–10 where laboratory testing is applied to identify those at risk of a disorder, in a population who have not sought medical attention on account of symptoms of that disorder. 11
Immunoassay interference due to complement is reported, in rare cases, in the autoDELFIA® serum alphafetoprotein (AFP) assay and may cause falsely decreased concentrations. 12 AFP is measured as part of second-trimester and integrated Down's screening tests, which calculate the chance of a Down's syndrome-affected pregnancy using a combination of maternal age and weight, gestation of the fetus and a blood test for biochemical markers. 13 Serum AFP, human chorionic gonadotrophin (HCG) (or freeβ HCG) and unconjugated oestriol (uE3) are the markers used for the triple test, with the addition of inhibin for the quadruple test. Integrated serum testing combines measurement of pregnancy-associated polypeptide A in the first trimester with the quadruple test in the second trimester. In cases of Down's syndrome, the AFP concentration is decreased by around one quarter compared with concentrations found in an unaffected singleton pregnancy. 14 Decreased AFP concentrations increase the calculated risk of a Down's syndrome pregnancy. Therefore, a falsely low AFP, due to assay interference, will lead to an artificially increased calculated Down's syndrome risk, which may result in a false screen positive result.
It was our aim to assess whether negative interference in the autoDELFIA® hAFP assay caused very low AFP concentrations, and to examine the effect of falsely decreased AFP concentrations on the calculated risk of Down's syndrome.
Method
The Department of Medical Biochemistry, University Hospital of Wales provides second-trimester Down's syndrome screening for the whole of Wales, and screens approximately 19,000 women/year. Between 18 January 2010 and 28 October 2010, AFP was measured in 15,729 samples using the autoDELFIA® hAFP assay (Perkin Elmer Life and Analytical Sciences, Turku, Finland). The autoDELFIA® hAFP assay is a two-site immunometric assay which uses mouse monoclonal antibodies directed against two separate antigenic determinants on the AFP molecule. Between-assay precision was 3.0% at 10.1, 2.7% at 29.8 and 2.3% at 69.5 KU/L.
Samples having an AFP concentration of less than 15 KU/L were identified and to screen for interference, AFP was re-measured using the Modular Analytics E170 (Roche GmbH, Mannheim, Germany). Between-assay precision was 4.2% at 9.4 and 2.9% at 100.9 KU/L.
To confirm that the interference in the autoDELFIA® hAFP assay was due to complement, samples in which discordant AFP results were recorded were stored at 4°C for one week before re-assay. 1
Serum AFP concentrations obtained using the autoDELFIA® hAFP assay, either fresh or after storage at 4°C for a week, were converted into weight-corrected multiples of the median (MoM). AFP MoMs were truncated below 0.4 MoM and used in the triple test Down's calculation (LifeCycle 3.1; Perkin Elmer Life and Analytical Sciences). A risk of Down's syndrome greater than 1 in 150 was considered screen positive. 15 For samples in which interference in the AFP assay was suspected, screen negative results were reported, but the actual risk was suppressed, with a comment that it was not possible to report an accurate risk due to interference in the AFP assay. Since a falsely decreased AFP result may cause a false-positive Down's risk, all screen positive results were suppressed in those samples with suspected interference and patients were offered the opportunity of a repeat test.
Results
Three hundred and twenty-three samples with AFP concentration <15 KU/L using the autoDELFIA® hAFP assay were identified. All samples were screened for interference by repeat analysis using the E170 AFP assay (Figure 1). Nine samples (from eight patients) were considered to exhibit interference in the autoDELFIA® hAFP assay on the basis of discordant AFP concentrations between the two methods (Table 1, Figure 1). The relationship between the two methods for the remaining 313 samples was given by y = 1.0199x − 0.5724 (R 2 = 0.7315) (Figure 1). Of the nine samples in which interference in the autoDELFIA® hAFP assay was identified, two were associated with a positive Down's syndrome screen (Table 1).
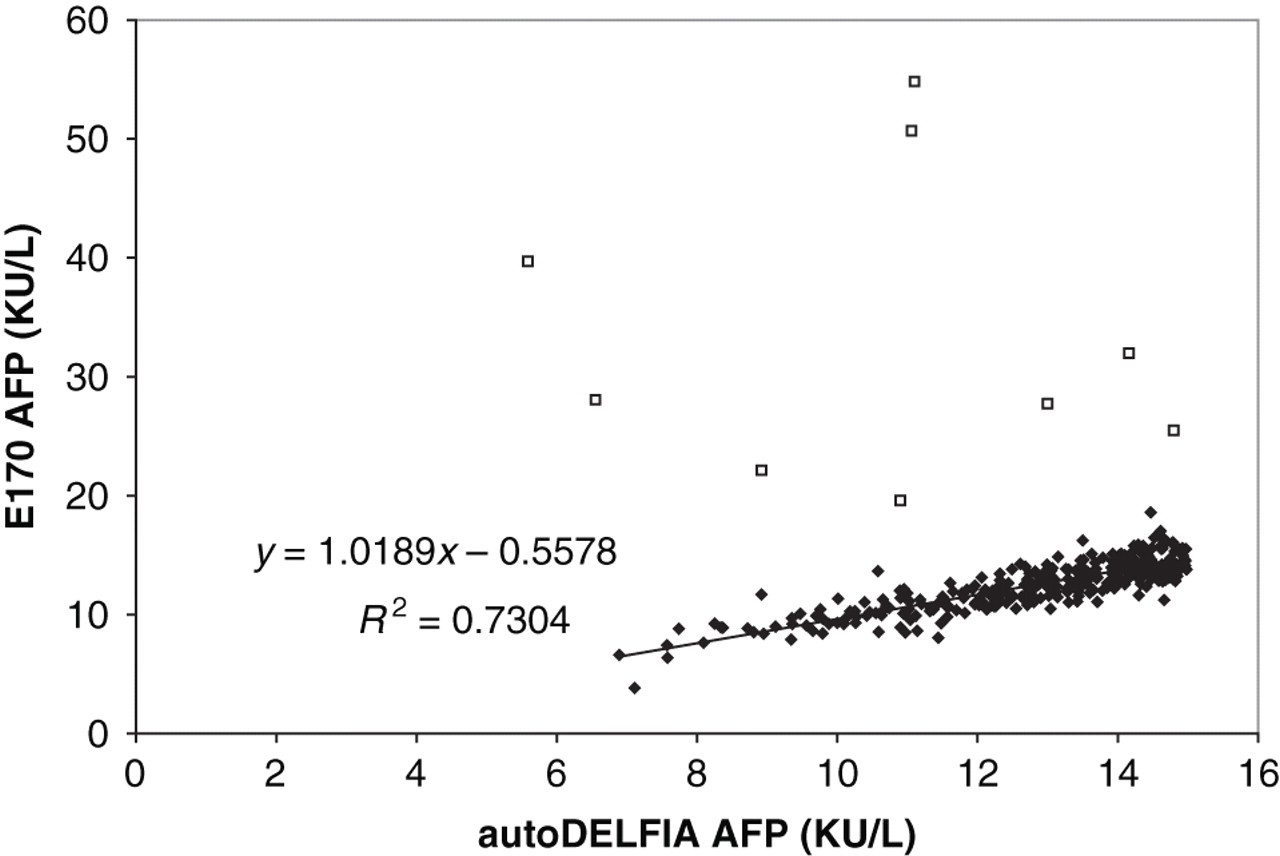
Scatter plot of autoDELFIA® and E170 AFP assays. Open boxes show samples considered discordant and therefore affected by immunoassay interference. Closed diamonds show correlation of remaining samples and the regression equation for these samples is also shown AFP, alphafetoprotein
Details of samples with falsely decreased AFP concentrations due to interference in autoDELFIA® hAFP assay
Weight-corrected AFP, uE3 and HCG MoM and maternal age at term are given. Down's risk calculated by triple test, risk > 1 in 150 is considered positive. Repeat autoDELFIA® hAFP concentrations following one week at 4°C are shown to demonstrate the effect of complement depletion
AFP, alphafetoprotein; MoM, multiples of the median; HCG, human chorionic gonadotrophin; uE3, unconjugated oestriol
Four of the nine samples with suspected interference were available for further investigation. Following storage for one week at 4°C to deplete complement, 1 these samples were re-analysed using the autoDELFIA® hAFP assay (Table 1). AFP was significantly higher in all samples following storage, consistent with complement interference in the assay. Down's risks re-calculated using the AFP measurements undertaken following complement depletion were significantly decreased compared with that calculated using the fresh samples (Table 1).
Discussion
We have established that falsely low AFP concentrations due to immunoassay interference in the autoDELFIA® hAFP assay occurs in 2.8% of samples with reported AFP concentrations <15 kU/L. AFP concentrations increased following storage of samples at 4°C, consistent with complement interference, which can affect immunoassays by blocking antibody binding to antigens through binding to the Fc region of the antibodies used in the assay. 1
Perkin Elmer suggests that interference in the autoDELFIA® hAFP immunoassay is rare, but its use in a national screening programme makes it inevitable that such cases will arise. Second-trimester and integrated screening tests, which require AFP measurement, currently account for 44.5% of Down's screening tests in the UK. 16 Twenty-three UK laboratories measure AFP for Down's screening, 16 of which use the autoDELFIA® hAFP assay (personal communication, Mr Andy Ellis, UK NEQAS). Although in England there is a move to first-trimester Down's screening, 17,18 second-trimester screening will continue to be required for those women who attend later in the pregnancy (around 15% of the pregnant population). 17 Quad testing is the recommended second-trimester test. 17 We have calculated Down's syndrome risk using the triple test in this manuscript and have demonstrated that falsely decreased AFP concentrations significantly increase the calculated risk of Down's syndrome. False AFP results are likely to have less of an effect when Quad or integrated screening tests are used, because more markers are used in the calculation. The truncation of AFP MoMs at 0.4 also limits the impact of a falsely low AFP on the Down's syndrome risk.
When a Down's syndrome screen positive result is returned, the woman will usually be offered an invasive diagnostic test comprising amniocentesis and karyotyping of fetal cells. Amniocentesis is associated with an approximate risk of fetal loss of 1% compared with women with no invasive testing, 17 and hence it is vital that laboratories are aware of the potential for immunoassay interference to cause false Down's screen positive results and where possible take steps to mitigate this occurrence. We suggest that Down's screen positive reports where AFP is <15 KU/L are investigated for interference. Interference is also likely to be found in samples with AFP concentrations >15 KU/L, and therefore we also recommend that screen positive results are scrutinized so that results where the AFP MoM is atypically low, are also screened for assay interference by measuring AFP by an alternative method. Finally, although laboratories may take steps to identify false screen positive results, elimination of assay interference should be a priority of assay manufacturers. 2 Use of Fab antibody fragments (derived from papain digest if immunoglobulins) or inclusion of chicken IgG or EDTA into the assay reagent have been used to reduce complement binding and are approaches that may reduce this problem. 1
Footnotes
DECLARATIONS