
Abstract
Background
The clinical performance of the Roche cobas e411 automated assay for the measurement of thyrotropin (TSH)-receptor antibodies (TRAbs) for the diagnosis of Graves' disease was evaluated in the setting of new referrals to a specialized thyroid clinic.
Methods
The final diagnosis of 102 new patients attending their first outpatient appointment at a thyroid clinic was correlated with the TRAbs result. In all cases, the diagnosis was made independently of the TRAbs result by the same consultant (ADT) based on clinical examination, thyroid function tests (TSH, free thyroxine, total triiodothyronine measured on Architect; Abbot Diagnostics), and a technetium-99m uptake and scan. TRAbs were measured using the cobas e411 (Roche Diagnostics). The clinical sensitivity and specificity of the assay were determined and compared with other published performance characteristics of the assay.
Results
Optimal sensitivity (95%) and specificity (98%) were obtained using a cut-off of 1.6 IU/L. The positive and negative predictive values at this cut-off were calculated as 98% and 94%, respectively.
Conclusions
Using a cut-off of 1.6 IU/L, considered independently of thyroid function tests, the Roche cobas e411 automated immunoassay for TRAbs is a convenient, sensitive and specific tool for the differential diagnosis of hyperthyroidism.
Introduction
Graves' disease is an autoimmune condition causing hyperthyroidism through auto-antibody stimulation of the thyrotropin (TSH) receptor. Measurement of TSH-receptor antibodies (TRAbs) is therefore useful in the differential diagnosis of hyperthyroidism. Recently, an automated, third-generation TRAbs assay has become available, which comprises a human, ruthenium-labelled monoclonal TRAb that competes with endogenous TRAbs in patient serum samples for binding to porcine TSH-receptors.
Several published studies have assessed this assay and recommended different cut-offs for use in the diagnosis of Graves' disease (1.75 and 1.86 IU/L). 1–4 In this paper, we report our experience of the clinical utility of the assay performed using the Roche cobas e411 on new patients presenting to a specialized thyroid clinic.
Methods
Patients
The final diagnosis of 102 consecutive patients attending their first appointment at a thyroid clinic (Royal Infirmary of Edinburgh) between June 2008 and August 2009 was obtained. In each case the diagnosis was made by the same consultant (ADT), independently of the TRAbs result, based on clinical examination with TSH, free thyroxine (FT4) and total triiodothyronine concentrations measured on the Architect analyser (Abbott Diagnostics, Berkshire, UK). Seventy patients received a technetium-99 uptake scan to aid diagnosis.
Based on initial thyroid function test results, 58 of the 102 patients included in the study had overt hyperthyroidism, seven patients had subclinical hyperthyroidism, one patient had hypothyroidism, five patients had subclinical hypothyroidism and 31 patients were euthyroid. Fifty-three of the patients with overt hyperthyroidism were diagnosed with Graves' disease. The remaining five overtly hyperthyroid patients had diagnoses of autonomous nodule, postpartum thyroiditis, silent thyroiditis, type 2 amiodarone-induced thyroiditis or viral thyroiditis. Three of the patients with subclinical hyperthyroidism were diagnosed with Graves' disease; two of these received an isotope uptake scan and all three had TRAbs detected in their serum samples. The remaining four patients with subclinical hyperthyroidism all received isotope uptake scans; three were diagnosed with multinodular goitre and one with a toxic nodule.
TRAbs analysis
TRAbs were measured using the cobas e411 analyser (Roche Diagnostics, Sussex, UK). The sensitivity, specificity and positive and negative predictive values for the TRAbs assay in the diagnosis of Graves' disease were compared with published performance characteristics at cut-offs of 1.6, 1.75 and 1.86 IU/L, and also the manufacturer's stated functional sensitivity (0.9 IU/L). It was noted that false-positive results were obtained on samples collected in lithium-heparin tubes (unpublished data).
Results
Assay precision
The functional sensitivity of the TRAbs assay was determined to be 0.8 IU/L (CV 20%). We applied the manufacturer's stated functional sensitivity (0.9 IU/L) throughout this study. The between-assay precision was as follows: in-house pool mean 2.7 IU/L, CV 6.5% (17 runs); Precicontrol-1 mean 4.5 IU/L, CV 4.0% (11 runs); and Precicontrol-2 mean 16. 9 IU/L, CV 6.0% (11 runs).
Clinical utility
Figure 1 displays the TRAbs results by diagnoses. All 56 patients with Graves' disease had a serum TRAbs concentration ≥1.5 IU/L. TRAbs were also detectable in five patients without Graves' disease, viz: autoimmune subclinical hypothyroidism (TRAbs 1.7 IU/L, TSH 4.6 mU/L and FT4 14 pmol/L), Hashimoto's thyroiditis (TRAbs 1.5 IU/L, TSH 0.27 mU/L and FT4 15 pmol/L), postpartum thyroiditis (TRAbs 0.9 IU/L, TSH 69.5 mU/L and FT4 6 pmol/L), solitary toxic nodule (TRAbs 0.9 IU/L, TSH <0.01 mU/L and FT4 17 pmol/L) and postpartum thyroiditis (TRAbs 1.2 IU/L, TSH 4.7 mU/L and FT4 10 pmol/L). TRAbs were undetectable in the remaining 41 patients. Only one of the five patients with non-Graves' hyperthyroidism had detectable TRAbs (solitary toxic nodule, TRAbs 0.9 IU/L).
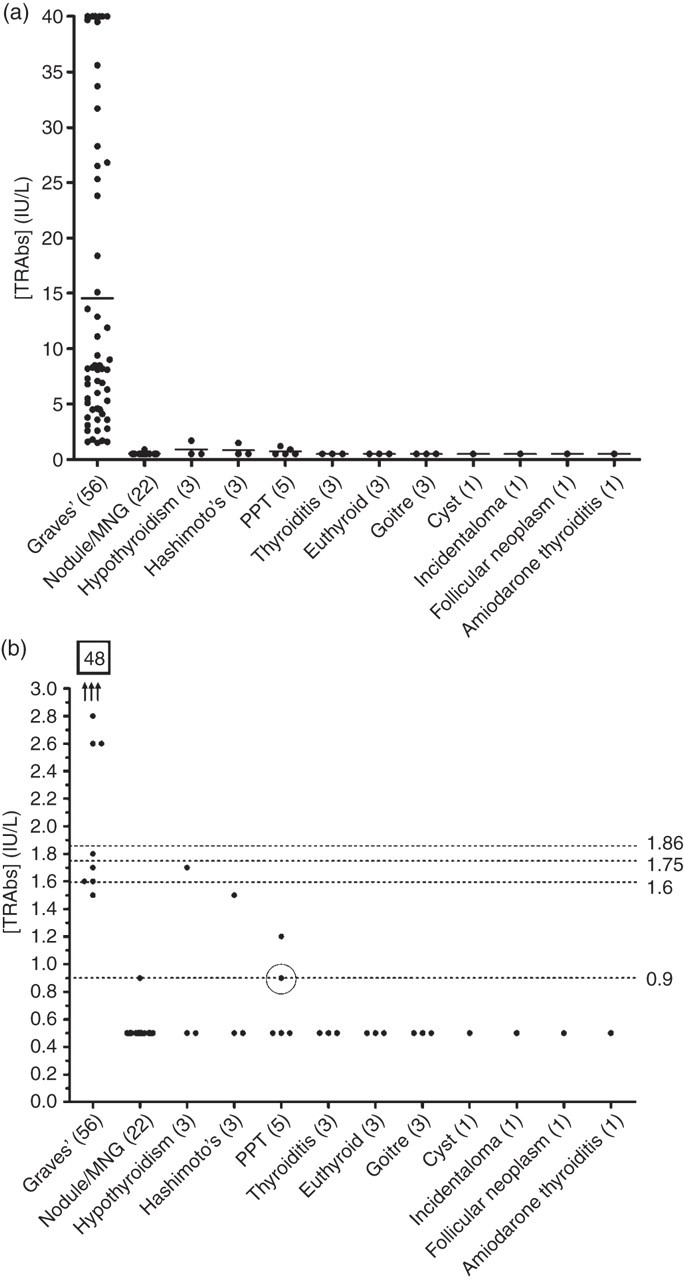
(a) TRAbs concentration plotted against diagnosis for patients attending their first appointment at a thyroid clinic, Royal Infirmary of Edinburgh between June 2008 and August 2009. Bars represent mean values. (b) Data as in (a), focusing on the range 0.0–3.0 IU/L. Dashed lines represent the functional sensitivity of the assay (0.9 IU/L) and the in-house (1.6 IU/L) and published (1.75 and 1.86 IU/L) recommended cut-offs. The circled point represents a case where the final diagnosis was unclear (PPT/Hashimoto's thyroiditis) and the patient was lost to follow-up. Numbers in brackets represent the number of patients with each diagnosis. MNG, multinodular goitre; PPT, postpartum thyroiditis. Sensitivities of 100%, 95%, 93% and 91%, and specificities of 89%, 98%, 100% and 100% were determined for the cut-offs 0.9, 1.6, 1.75 and 1.86 IU/L, respectively
Clinical utility with a cut-off of 0.9 IU/L
Using the functional sensitivity (≥0.9 IU/L), the following performance characteristics were found: sensitivity 100%, specificity 89%, and positive and negative predictive values of 92% and 100%, respectively.
Clinical utility with a cut-off of 1.6 IU/L
Serum TRAbs were >1.6 IU/L in 53 of the 56 patients with Graves' disease (sensitivity 95%). Five patients without Graves' disease had detectable TRAbs, which in one case was >1.6 IU/L (false-positive), giving a specificity for excluding Graves' disease of 98%. The positive and negative predictive values were 98% and 94%, respectively.
Clinical utility with a cut-off of 1.75 IU/L
TRAbs were >1.75 IU/L in 52 of the 56 patients diagnosed with Graves' disease, giving a sensitivity of 93%. No patient without Graves' disease had a TRAbs concentration above this cut-off, producing a specificity of 100%. For a cut-off of 1.75 IU/L, the positive and negative predictive values were 100% and 92%, respectively.
Clinical utility with cut-off of 1.86 IU/L
Fifty-one of 56 patients with Graves' disease had a TRAbs concentration >1.86 IU/L. No disease-negative patients had a TRAbs concentration above this cut-off. Performance characteristics using 1.86 IU/L as the cut-off were: sensitivity 91%, specificity 100%, positive predictive value 100% and negative predictive value 90%.
Discussion
TRAbs were detectable (>0.9 IU/L) in the serum samples of all 56 patients with Graves' disease, but also in five patients without the illness. This cut-off gave good sensitivity (100%), but poor specificity (89%) with positive and negative predictive values of 92% and 100%, respectively. When considering only patients with biochemical evidence of hyperthyroidism, the sensitivity, specificity and positive and negative predictive values were all 100%.
Previous studies have determined optimal cut-offs of 1.75 and 1.86 IU/L for this assay, with reported sensitivities and specificities of 97–100% and 99–100%, respectively. 1–4 Application of these cut-offs to our patient cohort produced poorer sensitivities than those reported in previous studies (sensitivities 91–93%). We found that optimal sensitivity (95%) and specificity (98%) for the diagnosis of Graves' disease was achieved using 1.6 IU/L when TRAbs results were considered independently of thyroid function test results.
Measurement of TRAbs is most useful in the differential diagnosis of hyperthyroidism. Since our study included few patients with non-Graves' hyperthyroidism, we may have over-estimated the specificity of the assay compared with a cohort including more of these patients. However, we conclude from the results that the Roche cobas e411 TRAbs assay is a convenient and useful tool for the differential diagnosis of hyperthyroidism.
DECLARATIONS