
Abstract
A 50-year-old man presented with a four-year history of unsteadiness, with recent falls and tingling in his fingers. Neurological examination found an ataxic gait, with a positive Romberg's sign. There was distal wasting and weakness in all four limbs and impaired co-ordination, with pseudoathetosis in the arms. Initial investigations showed a normochromic, normocytic anaemia, leucopenia, neutropenia and a low vitamin B12 (172 ng/L). Treatment with intramuscular cobalamin injections showed no clinical improvement. Further investigations showed an undetectable caeruloplasmin (<0.085 g/L), a very low serum copper (1.1 μmol/L) and a markedly raised serum zinc concentration (36.2 μmol/L). On detailed questioning it became apparent that he had ill-fitting dentures requiring excessive use of denture fixative with high zinc content. The patient was switched to a non-zinc containing denture fixative and commenced copper supplementation. Although within three months the bone marrow suppression had resolved, there was no clinical improvement in neurological presentation. Questioning a patient about their denture fixative usage and checking if zinc is an ingredient may be considered during an investigation for myelopolyneuropathy when vitamin B12 deficiency is not a cause.
Introduction
Copper deficiency is a rare cause of bone marrow suppression and neurological dysfunction. Zinc excess is known to cause copper deficiency by preventing the absorption of copper from the gut into the bloodstream. We describe a case of copper deficiency secondary to excessive use of a zinc-containing denture fixative, leading to myelopolyneuropathy and bone marrow suppression.
Case history
A 50-year-old man presented to the neurology clinic with a four-year history of unsteadiness with recent falls. He also described tingling in his fingers which was causing him to drop objects and a sensation of tightening in his legs. Previous medical history included mastoid surgery at 18 years old, leaving him with a hearing impairment. There was no family history of neuromuscular disease, he was not on any medication, did not drink and gave up a heavy smoking habit two years previously. Neurological examination demonstrated an ataxic gait with a positive Romberg's sign. There was wasting in the hands and the lower legs. Tone appeared normal. Power was decreased for the small muscles of both hands and for foot dorsiflexion and toe extension in both feet. Reflexes were normal with flexor plantar responses. Co-ordination was impaired for finger nose testing in both arms with pseudoathetosis present with eyes closed. Heal shin testing was impaired in both legs. Light touch, pinprick and temperature sensation were normal. Vibration was decreased at both ankles and proprioception was lost in the big toe bilaterally.
Initial investigations showed a normochromic, normocytic anaemia, leucopenia, neutropenia (Table 1) and a serum vitamin B12 concentration of 172 ng/L. Magnetic resonance imaging (MRI) scan of the brain was normal. Cerebral spinal fluid was negative for oligoclonal banding and a bone marrow aspirate was found to be hypocellular without signs of malignancy or significant myelodysplasic changes.
The biochemistry and haematology results on initial investigation (A); after three months of cobalamin injections (B); after three months of copper supplementation and cessation of zinc-containing Poligrip Ultra (C); two-month follow-up after stopping copper supplements (D)
In view of the low serum vitamin B12 concentration and large fibre neuropathy (including impaired vibration, proprioception and a positive Romberg's sign), the patient was treated with intramuscular cobalamin injections, which increased the serum vitamin B12 concentration to 683 ng/L after three months. Despite the cobalamin treatment there was no clinical improvement, with the patient presenting in the next clinic with further neurological deterioration, including difficulty in walking. In addition, he remained anaemic, neutropenic and leucopenic (Table 1). His cervical spine MRI showed no abnormality. Further questioning into family history gave no additional information. Although the patient had the signs of myelopolyneuropathy, vitamin B12 deficiency was now considered unlikely.
Further biochemical investigations, however, showed an undetectable caeruloplasmin (<0.085 g/L), a very low serum copper (1.1 µmol/L) and a markedly raised serum zinc (38.2 µmol/L) (Table 1 and Figure 1). Copper deficiency secondary to zinc excess was considered the likely diagnosis. There were no clinical features of malabsorption, no history of any bowel surgery and he was not taking any zinc supplements. On detailed questioning it became apparent that he had ill fitting dentures, requiring excessive use of the denture fixative Poligrip Ultra (GlaxoSmithKline, Brentford, UK), known to have high zinc content (38 mg of zinc per gram). 1 The manufacturer's recommendations are that a 40 g tube should last six weeks. 1 Our patient had been using approximately 2–3 tubes per week, for three to four years. Immediately he was advised to switch to a non-zinc containing denture fixative and a copper supplement was sourced from Holland and Barrett (Nuneaton, UK) (2 mg daily).
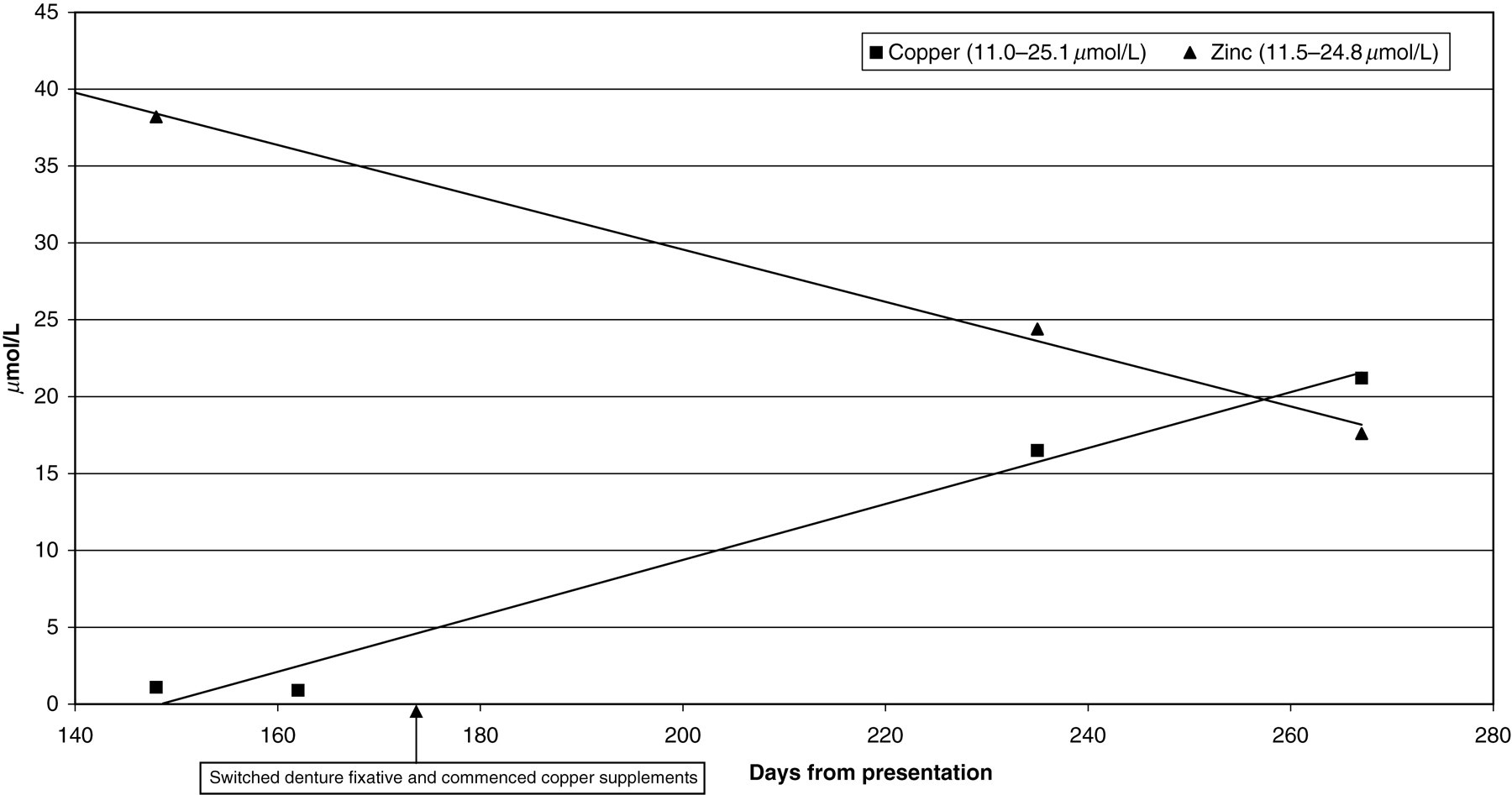
Serum zinc and copper concentrations at presentation and after the cessation of zinc-containing denture fixative and the commencement of copper supplements
On follow-up three months later, the clinical neurological features were unchanged with an ataxic gait, positive Romberg's sign, impaired co-ordination and proprioception. Of note there had been no further neurological deterioration. Within three months from initiation of treatment, the anaemia, leucopenia and neutropenia had resolved and the caeruloplasmin, copper and zinc concentrations are now falling within the respective healthy population reference ranges (Table 1 and Figure 1). The copper supplements were stopped and two months later zinc and copper serum concentrations were re-measured (Table 1).
The copper–zinc conflict
Dietary copper is found in a variety of foodstuffs including meat, fish, nuts, seeds and legumes. 2 Dietary deficiency is therefore rare. When it is detected, up to one-half of cases have had previous gastrointestinal surgery, as copper is absorbed in the stomach and proximal duodenum. 2,3 Copper functions as a prosthetic group, allowing electron transfer in essential enzyme pathways. 3 It is present in a number of key enzymes and proteins throughout the body, especially associated with the functioning of the nervous system including: caeruloplasmin (promotes haematopoiesis by oxidation of Fe2+ to Fe3+), cytochrome C oxidase (a mitochondrial electron-transport chain enzyme), dopamine beta-hydroxylase (catecholamine biosynthesis), monoamine oxidases (catecholamine metabolism), lysyl oxidase (essential for collagen elastin cross-linking) and superoxide dismutase (antioxidant). 2–4 Copper deficiency therefore leads to neurological and haematological dysfunction, and may present with clinical features of myelopolyneuropathy (which resembles subacute combined degeneration of the spinal cord as a result of vitamin B12 deficiency). 3,5,6 Reduced levels of cytochrome C oxidase are considered to be the cause of the neurological dysfunction. 3 Treatment with copper supplementation stops further deterioration, but recovery is minimal and often subjective whereas the haematological abnormalities promptly resolve. 3,4,6
Zinc induces the expression of intracellular metallothionein, a chelator in the gut enterocytes. Copper has a higher affinity for metallothionein than zinc and will therefore displace any bound zinc, and will be lost in the faeces when the enterocyte is sloughed off. 2–5 Excess zinc therefore reduces copper absorption resulting in a negative copper balance. This mechanism is exploited in using zinc for the treatment of Wilson's disease patients. 2,3,5 Documented sources of high zinc intake include excess administration in enteral/parenteral nutritional support, 4 excess supplementation as a cold/flu preventive 3,4 and swallowing zinc coins. 3 However, a proportion of reported hyperzincaemia cases still have no source identified. Only recently has the excessive usage of zinc-containing denture fixative been considered or identified. 4–6
Zinc-containing denture fixative
Modern denture fixatives contain variable amounts of zinc (between 17–38 mg/g) 1,6 in the form of calcium–zinc polymers, which on exposure to saliva are hydrated and establish cohesion with the gums to fix the denture in place. 6 Zinc is not absorbed through the gums. 1 The denture fixative becomes soluble over time with small pellets being swallowed, thus allowing zinc absorption via the gut. 1,6 Reported cases have in common a long-term use of fixatives, usually with poor-fitting dentures, often requiring excessive and regular application, using an average of more than two tubes per week. 4–6 As in our case, these patients were treated by switching to a non-zinc containing fixative and with the administration of copper supplements. In all cases there was a prompt resolution of the haematological abnormalities (i.e. anaemia, leucopenia, neutropenia). Although further neurological deterioration is halted, there is often little improvement. 4–6 In March 2010, a UK Consumer Advisory warning was issued with GlaxoSmithKline voluntarily withdrawing production and distribution of the Poligrip zinc-containing fixatives. 1
Conclusions
Early identification of zinc poisoning due to the excessive use of denture fixative may have potentially prevented further irreversible neurological damage and could have avoided two invasive procedures. It is advisable in patients who wear dentures and present with either myelopolyneuropathy and/or bone marrow suppression without vitamin B12 deficiency, to question their historical and current denture fixative usage, especially if long term and excessive. Patients may still have access to zinc-containing fixatives from alternative sources to pharmacies, e.g. markets, online shopping or from brands that still use a zinc polymer. Information on the composition of the denture fixative should be sought and if it contains zinc we would recommend measurement of serum caeruloplasmin. If this is found to be low, then both serum copper and zinc should be analysed immediately. Of further note, as Poligrip zinc-containing products have been withdrawn, there may now be a cohort of patients with neurological damage who have been ‘treated’ by a switch to non-zinc containing denture fixative. By removing the zinc source, resolution of the hyperzincaemia, hypocupraemia and bone marrow suppression would occur within a few months, thus preventing any conclusive diagnosis by laboratory testing. There is the possibility that such patients could be misdiagnosed and receive inappropriate investigation and treatment or remain without a definitive diagnosis for their neurological condition. We believe this may be the first case of zinc poisoning from excessive use of denture fixative reported in the literature from the UK.
DECLARATIONS