
Abstract
Background
Asthma is associated with increased inflammation, oxidative stress and abnormal immune system function. We determined the distributions of several essential trace minerals and assessed their relationships to factors that are associated with the pathophysiological status of patients with mild/moderate asthma.
Methods
We enrolled 25 asthmatic patients and 25 healthy subjects. We measured: blood trace minerals, zinc (Zn), copper (Cu) and selenium (Se); oxidative stress markers thiobarbituric acid reactive substances (TBARS); antioxidant enzyme activities; percentages of CD4 and CD8 lymphocyte subsets; high-sensitivity C-reactive protein (hs-CRP); and a lung function index (FEV1/FVC%).
Results
Compared with healthy subjects, asthmatics had lower concentrations of Zn and Se; higher Cu concentrations, and Cu/Zn and Cu/Se ratios; and lower antioxidant enzyme glutathione peroxidase (GPx), glutathione reductase (GR) and catalase activities. Significantly increased concentrations of hs-CRP, TBARS and CD4/CD8 lymphocyte ratios were also observed. Furthermore, plasma TBARS or hs-CRP concentrations were negatively associated with Se concentrations, but were positively associated with Cu/Se ratios. CD4/CD8 lymphocyte ratios were inversely correlated with Se, while it was positively correlated with Cu/Se ratio. FEV1/FVC% was also significantly correlated with Se concentrations, and Cu/Se and Cu/Zn ratios.
Conclusions
Abnormal distributions of these trace minerals may aggravate oxidative damage and inflammation, increased CD4/CD8 lymphocyte ratios and decreased lung function in asthma.
Introduction
Asthma is a major public health problem of increasing concern worldwide. It is a chronic inflammatory disorder of the airways that is characterized by variable bronchial obstruction and hyper-responsiveness. 1 Infiltrations of the airway walls by mast cells, T-lymphocytes and eosinophils are involved in the inflammatory process, which correlates significantly with disease severity. 1,2 It has been shown that an imbalance of Th1/Th2 helper cells and CD4+ Th2-type lymphocyte cytokine production are involved in the recruitment of inflammatory cells and hyper-responsiveness. 3
Recently, evidence suggests that oxidative stress and inflammation play critical roles in both the initiation and development of asthma. 4,5 Oxidative stress induces inflammatory response in the respiratory system, which causes tissue injury and immune-mediated damage. 6 Reduced glutathione (GSH) is an important protective, regulatory antioxidant. 3 Decreased intracellular GSH can lower Th1 activity and increase Th2 activity. 7 Among GSH-depleted peripheral T-cells, there is a markedly increased ratio of CD4/CD8 cells. 8 In addition, different antioxidant enzymes, such as GSH peroxidase (GPx), GSH reductase (GR), superoxide dismutase (SOD) and catalase, with a wide range of activities are found in lung tissues and blood. 9,10 Compared with healthy subjects, asthmatic children have been found to have significantly increased serum oxidative stress and decreased GPx activity. 11
Essential trace minerals such as zinc (Zn), copper (Cu) and selenium (Se) are known to play important roles in the maintenance of redox homeostasis, which are also required for immune system function. Alterations in these minerals’ status may result in higher inflammatory responses and oxidative stress. 12 For example, disturbances of Zn homeostasis can lead to a shift in the Th1/Th2 balance towards a Th2 response. 13 In an animal model, an intracellular pool of Zn in airway epithelium was associated with inflammatory status. 14 Also, Se stimulates a Th1 immune response against viral infections. 15 There appears to be a lower serum concentration of Se in patients with asthma, 16 although conflicting results have been reported. 17 In addition, Cu deficiency and excess can induce oxidative stress that can lead to chronic inflammation. 18 Elevated serum Cu may be a useful marker of inflammation and immune status. 19 However, there is limited information regarding the distribution of plasma Cu in asthmatic patients.
Disturbances in plasma trace minerals’ homeostasis can influence the states of oxidative stress, inflammation and immune responses. However, asthma may create disturbances in the homeostasis of trace minerals and how these are related to the pathogenesis of asthma has given conflicting results. Abnormalities in the homeostasis of one mineral affect the distribution patterns of other minerals, 20 which is one possible reason for conflicting results. In addition, possible correlations between these minerals with oxidative stress, inflammation, immune system response and lung function in asthmatic patients have not been examined.
In the present study, plasma trace minerals (Cu, Zn, Se concentrations, Cu/Zn and Cu/Se ratios), antioxidant enzyme activities (SOD, GPx, GR and catalase), inflammatory status by high-sensitivity C-reactive protein (hs-CRP), and immune cell CD4/CD8 ratios were compared between asthma patients and healthy controls. The relationships of trace minerals to lung function, oxidative stress, hs-CRP and CD4/CD8 lymphocyte ratios were also examined in asthmatic patients.
Methods
Patients
Between January and March 2007, 25 patients with mild/moderate asthma diagnosed according to the American Thoracic Society criteria at the otolarynology unit of Cheng-Ching Hospital (Taichung, Taiwan) were enrolled. Asthma is determined by pulmonary function parameters, including forced vital capacity (FVC) and forced expiratory volume in one second (FEV1), which is measured using a Jaeger MasterScreen (VIASYS Healthcare GmbH, Hoechberg, Germany).
None of the subjects was a smoker or had a respiratory tract infection or exacerbation of asthma. Subjects with heart disease, diabetes mellitus, liver disease, cancer and systemic inflammatory disorders, and who received immune suppressant drugs or supplementation with antioxidant vitamins/minerals were excluded. As a control, 25 volunteer healthy subjects of similar age and gender were studied. All subjects signed informed consent statements. The study protocol was approved by the ethics in human research committee of our hospital (Institution Review Board [IRB], #HP060007).
Biochemical analysis
Blood samples were drawn in the morning after an overnight fast of 12 h. Plasma concentrations of albumin, haemoglobin and immunoglobulin E (IgE) were estimated using routine laboratory techniques.
Measurement of oxidative stress and hs-CRP
Lipid peroxidation was determined by assaying the formation of thiobarbituric acid reactive substances (TBARS). Plasma samples were mixed with 3% sodium dodecyl sulphate, 0.1 N HCl, 10% phosphotungstic acid and 0.7% thiobarbituric acid and then incubated at 95°C. The TBARS were extracted into n-butanol and the fluorescence of the n-butanol layer was measured. 19
Plasma concentrations of hs-CRP were measured using the human CRP ELISA kit (E-80CRP; Immunology Consultants Laboratory, Inc, Newberg, OR, USA). The intra- and inter-assay coefficients of variation (CVs) were <3 and <4%, respectively. Briefly, 200 μL of combined enzyme–antibody conjugate and 3,3′,5,5′-tetramethylbenzidine substrate was added to each well and was incubated in darkness at room temperature. After 10 min the reaction was stopped with the addition of stop solution. The absorbance at 450 nm was measured, and readings were interpolated into the standard curve.
Determination of trace minerals
The concentrations of Zn and Cu were measured with a flame atomic absorption spectrophotometer (932 plus; GBC, Melbourne, Australia) using an air- acetylene flame without background correction at 213.9 and 324.71 nm, respectively. Samples were digested in a H2O2/HNO3 mixture in a START D microwave-assisted digestion system (Milestone Microwave Labstation ETHOS D), and the volume was increased with double-deionized water.
The accessory hydride formation system (HG 3000), from GBC, was used for determining Se concentrations. Samples were digested for a total of 6.5 h with an initial temperature of 60°C for 0.5 h, followed by increasing temperatures in 10°C increments and finally heated up to 200°C for 0.5 h in a mixture of 3.2 mL nitric acid (16 N) and 0.8 mL concentrated perchloric acid to convert all Se species to selenate. 19
Measurement of enzyme activity
Erythrocyte SOD activity was determined with a RANSOD kit (Randox, San Diego, CA, USA); one unit was defined as the amount of enzymes necessary to produce 50% inhibition in the rate of p-iodonitro-tetrazolium reduction. Catalase activity was performed with a commercially available kit (IBL Immunobiological Laboratories, Hamburg, Germany); one unit was defined as the amount of enzymes that caused the formation of 1.0 nmol of formaldehyde per minute at 25°C.
GPx activity was measured with a kit from Cayman Chemical (cat #703102; Ann Arbor, MI, USA); the rate of decrease in absorbance at 340 nm is directly proportional to the GPx activity. GR activity was assessed by monitoring the oxidation of NADPH to NADP+ via addition of oxidized GSH; one unit was defined as the amount of enzyme that catalysed the reduction of 1 mmol of oxidized GSH.
Determination of immunological parameters
Peripheral blood T-lymphocytes of all subjects were stained with the following monoclonal antibodies, which conjugated with fluorescein isothiocyanate (FITC) or phycoerythrin (PE): CD3 FITC/CD4 PE/CD8 PE (eBioscience, San Diego, CA, USA). Briefly, 100 μL of whole blood were incubated with 20 μL of monoclonal antibody reagent for 15 min in the dark at room temperature. Following leukocyte fixation and erythrocyte lysis with the CyLyse lysing reagent kit (Partec GmbH, Münster, Germany), the percentages of lymphocyte subsets were measured using a Partec CyFlow ML flow cytometer (Partec GmbH).
Statistical analysis
Quantitative variables were expressed as mean (SD) or median (interquartile range). A two-tailed P value less than 0.05 was considered statistically significant. The Kruskal–Wallis test was applied to evaluate the distribution of variances. Data in normal distribution was analysed using Student's t-test; data in non-normal distribution was analysed by the Mann–Whitney test. In addition, Pearson's or Spearman's correlation coefficients were performed to identify correlations of blood variables.
Results
Clinical characteristics
No significant differences in age, sex, body mass index (BMI) or plasma albumin levels were found between asthmatic patients and controls (P > 0.05) (Table 1). Compared with healthy subjects, asthma patients’ haemoglobin concentrations were higher. Also, asthmatic patients had significantly higher IgE concentrations. FEV1/FVC% is used for the diagnoses of obstructive and restrictive lung diseases. For the asthmatic patients, the mean FEV1/FVC% = 78.68 ± 9.90.
Characteristics of asthmatic patients and healthy subjects*
*Values are mean (SD) unless stated otherwise.
† P < 0.05 versus controls.
FVC, forced vital capacity; FEV1, forced expiratory volume in one second; hs-CRP, high-sensitivity C-reactive protein; TBARS, thiobarbituric acid-reactive substances; IQR, interquartile range
The levels of plasma markers of oxidative stress, TBARS, were considerably increased in asthmatic patients compared with healthy subjects. We also found significantly higher hs-CRP concentrations in asthmatic patients.
Trace mineral status, antioxidant enzymes and immunological variables
The plasma concentrations of Zn and Se were significantly reduced in asthmatic patients compared with healthy subjects. Asthmatic patients had significantly higher plasma Cu concentrations. In addition, markedly higher Cu/Zn and Cu/Se ratios were observed in asthmatic patients (Table 2).
Plasma levels of trace minerals and antioxidant enzymes, and immune function in asthmatic patients and healthy subjects*
*Values are mean (SD) unless stated otherwise.
† P < 0.05 versus controls.
Zn, zinc; Cu, copper; Se, selenium; SOD, superoxide dismutase; GPx, glutathione peroxidase; GR, glutathione reductase; IQR, interquartile range
Asthmatic patients had significant decreases in erythrocyte antioxidant enzyme GPx, GR and catalase activities. There was no significant difference in SOD activity between patients and healthy controls.
The asthmatic patients had higher CD4 and lower CD8 T-lymphocyte percentages compared with healthy subjects. The CD4/CD8 ratios for asthmatic patients were significantly higher than for controls.
Correlations between minerals and other parameters in asthmatics
For asthmatic patients, TBARS values showed statistically significant relationships to Zn (r = −0.450), Cu (r = 0.503) concentrations, and Cu/Zn ratio (r = 0.483) (data not shown) and Se (r = −0.446) concentration and Cu/Se ratio (r = 0.488) (Figure 1).
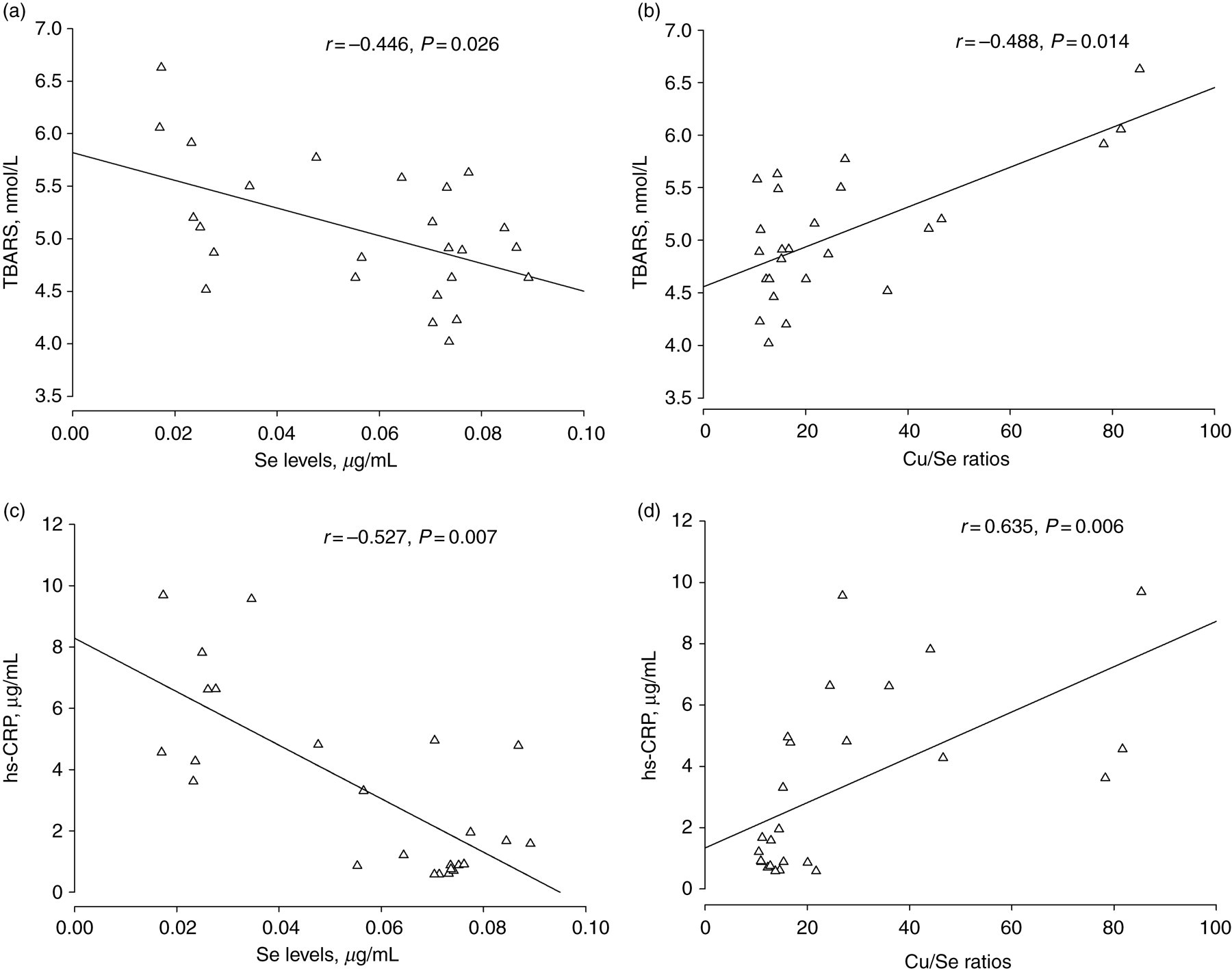
Correlations of TBARS or hs-CRP with trace mineral levels Se (a and c), and Cu/Se ratios (b and d) in asthmatic patients. TBARS, thiobarbituric acid-reactive substances; hs-CRP, high-sensitivity C-reactive protein
Significant correlations between hs-CRP concentrations and Se (r = −0.527) and Cu/Se ratio (r = 0.635) were also obtained (Figure 1). Plasma Zn, Cu and Cu/Zn ratio were not significantly related to hs-CRP levels. The hs-CRP levels were also strongly associated with TBARS (r = 0.415) (data not shown).
The pulmonary function indicator FEV1/FVC% was positively correlated with plasma Se concentrations (r = 0.504). There were significant inverse correlations between FEV1/FVC% and Cu/Zn (r = −0.412) and Cu/Se ratios (r = −0.417). There was also an inverse relationship between FEV1/FVC% and TBARS (r = −0.397)(Figure 2).
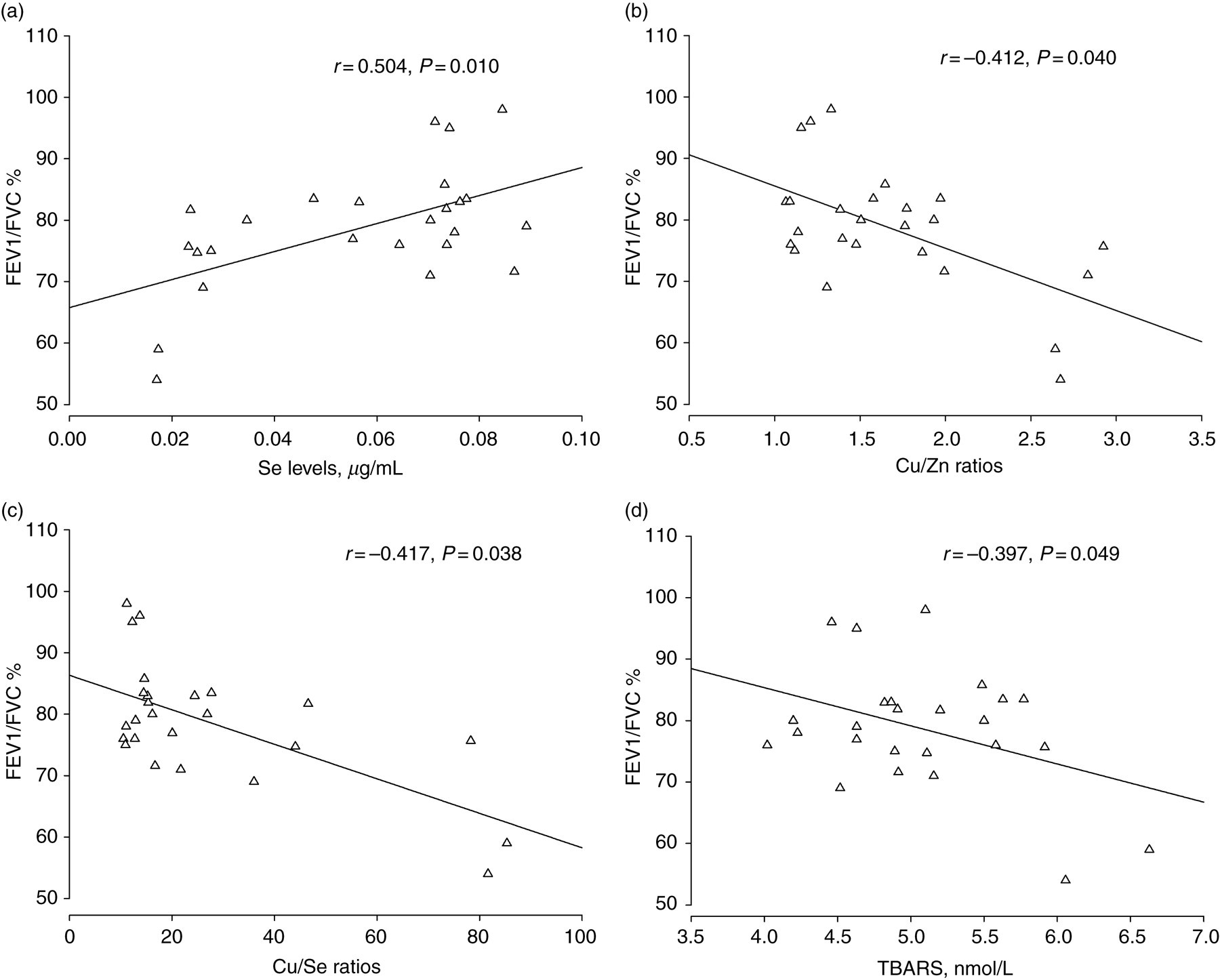
Associations between lung function FEV1/FVC% and blood variables Se (a), Cu/Zn ratio (b), Cu/Se ratios (c) or TBARS (d) in asthmatic patients. FVC, forced vital capacity; FEV1, forced expiratory volume in one second; TBARS, thiobarbituric acid-reactive substances
Se concentrations were negatively correlated with CD4/CD8 lymphocyte ratios. Plasma Cu/Se ratios were significantly positively related to CD4/CD8 lymphocyte ratios (Figure 3). In addition, CD4/CD8 ratios were related to plasma levels of TBARS (r = 0.298, P = 0.150), hs-CRP (r = 0.319, P = 0.119) and FEV1/FVC% (r = −0.211, P = 0.300), although this was not statistically significant (data not shown).
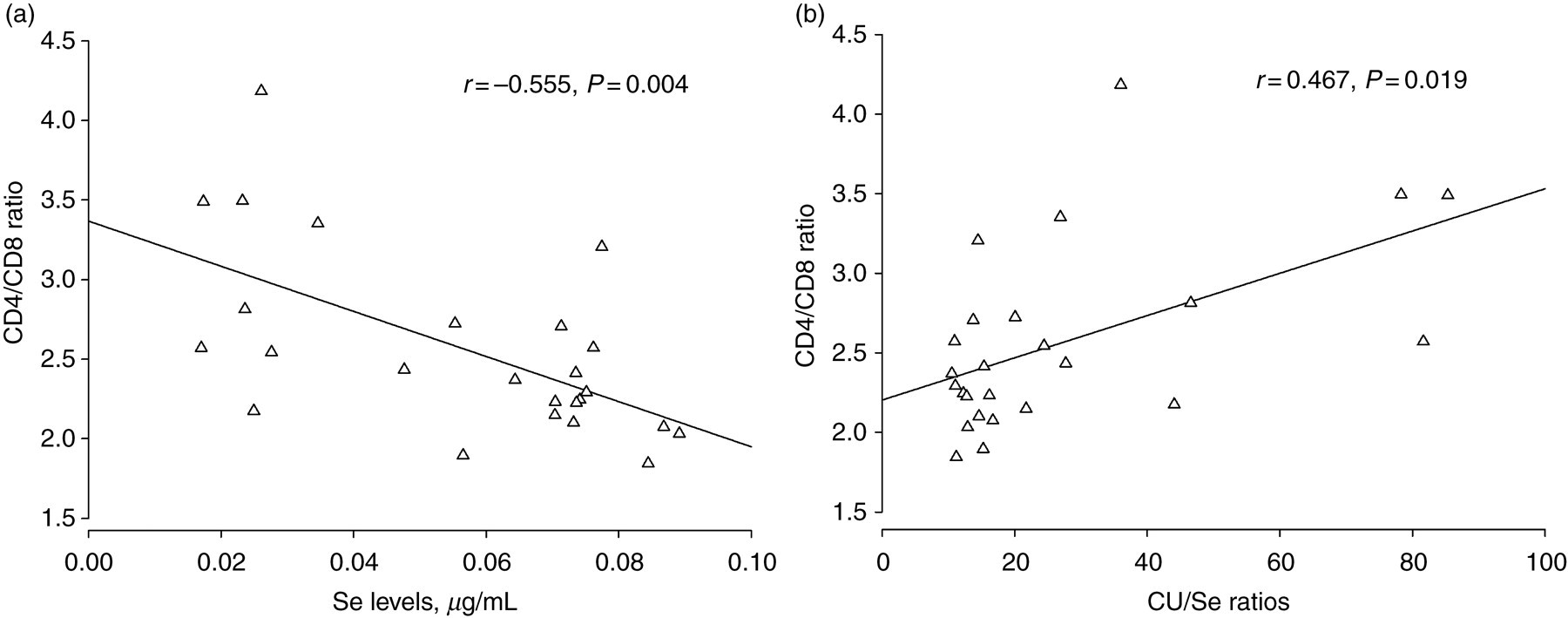
Relationships between immune index CD4/CD8 ratio and Se levels (a), and Cu/Se ratios (b) in asthmatic patients
Discussion
In the present study, patients with mild-to-moderate asthma had abnormal levels of three trace minerals (Cu, Zn and Se), higher TBARS values (indicator of oxidative stress), lower levels of antioxidant enzymes, increased hs-CRP levels, and higher CD4/CD8 lymphocyte ratios compared with controls. In addition, in these asthma patients, we found that disturbances of these trace minerals were associated with altered lung function, oxidative stress, inflammation status and immune response.
Relative to healthy controls, our asthma patients had significantly higher levels of haemoglobin, which may have been due to a compensatory need to carry more oxygen. The aetiology of asthma is dependent on numerous risk factors, including alterations in oxidant-antioxidant balances. 4 Essential trace minerals, such as Cu, Zn and Se, are key co-factors for regulating certain antioxidant enzyme expressions. We found that asthma patients had significantly lower plasma Zn and Se concentrations, and higher Cu concentrations compared with healthy controls.
Suboptimal Zn status is typically associated with many inflammatory diseases. 21 Increased expression of intracellular metallothioneins following oxidative stress or inflammation can sequester plasma Zn. 22 Increased Zn uptake may be needed to counteract the loss of Zn in the airways and to meet an increased demand for Zn-dependent proteins. 23 Up-regulation of Zn transporter genes is found in the inflammatory cells and can also reduce the levels of plasma Zn. 21 Moreover, increased plasma Cu concentrations may be explained by the release of Cu during inflammatory tissue damage, 19 and that high plasma Cu significantly inhibits the influx of Zn across small intestinal brush border membranes. 24
Plasma Zn concentrations were not found to be significantly different between patients with childhood asthma and controls. 25 However, hair and serum concentrations of Zn were markedly lower in wheezy infants than in healthy controls, suggesting that Zn deficiency may alter the risk of wheezing in early childhood. 26 Maternal intake of Zn during pregnancy is also negatively associated with wheezing illnesses in their childhood. 27
Se is also a potent antioxidant and acts as an anti-inflammatory agent. Increased inflammation may decrease the absorption of Se resulting in low Se status. 28 Decreased Se intake and serum levels in patients with asthma have been observed; 29 although, this finding was not confirmed by Jacobson et al. 17 In clinical intervention studies, opposite results on the clinical benefits to asthma patients after Se supplementation have also been observed. 30 These results suggest that the distributions of trace minerals and the pathogenesis of asthma may not be simply dependent on a single mineral.
Our results showed that, relative to healthy controls, asthmatic patients had significantly higher products of oxidation, TBARS and lower levels of antioxidant enzymes. We also found higher concentrations of plasma hs-CRP, a marker of inflammation, in these asthma patients.
Increases in oxidative stress can initiate and augment inflammation, and play an important role in inflammatory diseases, including asthma. 31 Decreased antioxidant enzyme GR activity was found to be significantly associated with asthma symptoms. 31 Also, antioxidant GSH status affects the early asthmatic reaction and airway hyper-responsiveness. 32 Supplements with Se could significantly reduce oxidative stress and increase the antioxidant enzyme activity of GPx in asthmatic patients. 11
As expected, we found that the plasma concentrations of Cu, Zn and Se, and the ratios of Cu/Zn and Cu/Se were significantly correlated with TBARS in asthmatic patients. Increased serum Cu concentrations and Cu/Zn ratios are associated with oxidative stress in some diseases. 19 The Cu/Zn or Cu/Se ratios may therefore be a clinical predictor of oxidative stress and inflammatory status. 19,33
Recent studies have found that serum hs-CRP concentrations were significantly higher in patients with mild-to-moderate asthma than in healthy controls. Increased serum hs-CRP levels are associated with airflow obstruction and airway inflammation, and may serve as a marker of airway inflammation and asthma severity. 34 Associations between increased levels of serum hs-CRP with a high frequency of airway hyper-responsiveness and lowered FEV1 or FEV1/FVC% (lung function indices) were also found. 35 Thus, hs-CRP may be related to asthma exacerbations and allergic inflammation.
Recent studies have also indicated that the phosphatidylinositol 3-kinase (PI3K) pathway plays an important role in the expression and activation of inflammatory mediators, inflammatory cell recruitment, immune cell function and airway remodelling. 36 Cu may activate the PI3K pathway, stimulate interleukin (IL)-6 production, and enhance the expression of intercellular adhesion molecule-1. 37,38 In contrast, Se may reduce inflammation via its antioxidant action and by modulating the expressions of selenoprotein genes. 15 Se status is significantly associated with suppressed IL-6 levels in disabled older subjects. 29 Se supplementation stimulated GPx enzyme activity and reduced NF-kB activation in HIV-infected patients. 39 Our results also indicated significant associations between hs-CRP, TBARS, Se and the Cu/Se ratio in asthma patients. This suggests that plasma Se concentrations and Cu/Se ratios may accurately reflect both oxidative stress and the degree of inflammation severity in patients with asthma.
Our results indicated significant associations between peripheral lymphocyte CD4/CD8 ratios with Se concentrations, and Cu/Se ratios in asthmatic patients. Increased CD4/CD8 ratios in the peripheral blood, bronchoalveolar lavage lymphocytes, and lung biopsies of asthma patients have been observed, and the CD4/CD8 ratio was negatively correlated with lung function. 40 In addition, activated CD4 T-cells increase and produce type 2 cytokines, such as IL-6 and tumour necrosis factor (TNF-α), which are involved in the recruitment of inflammatory cells and hyper-responsiveness. 41 Oxidative stress may alter the Th1/Th2 immune response and result in the activation of pro-inflammatory genes. 42 A trend for a positive correlation between the CD4/CD8 lymphocyte ratio and TBARS was observed in our study. These results suggest that increases in oxidative stress induced by an abnormal status of Se and Cu, resulting in higher CD4/CD8 ratios, can alter the balance between Th1/Th2 responses; however, we did not evaluate the production of Th1 and Th2 cytokines.
We found a significant negative correlation between oxidative stress and lung function (FEV1/FVC%) in these asthmatic patients. In addition, significant associations between FEV1/FVC% with plasma Se concentrations, and Cu/Zn and Cu/Se ratios were also found in asthma patients. Indeed, inflammation driven by increased oxidative stress has been implicated in the pathogenesis of asthma. Evidence indicates that inflammatory status is negatively associated with FEV1/FVC% in asthma patients. 43
An inverse association between TBARS with pulmonary function and a positive association between the antioxidant enzyme activity of GPx with pulmonary function have been observed. 44 A negative correlation between serum Se concentrations and attacks of wheezing has also been reported, 15 along with a positive relationship between serum Cu/Zn ratio and wheezing in respiratory diseases. 45 In our asthmatic patients, the plasma Se concentration, but not Cu or Zn, was associated with parameters of lung function, although the Cu/Zn and Cu/Se ratios were correlated with lung function. It appears that an inter-dependency among these trace minerals (Cu, Zn and Se) is a factor that may be important for the pathogenesis and severity of asthma.
The present investigation found that patients with mild to moderate asthma had significant disturbances in trace mineral (Cu, Zn and Se) homeostasis, and that this was presumably related to their oxidative stress status. A disruption of the Se status and the Cu/Se ratio may be responsible for inflammatory responses and increased CD4:CD8 lymphocyte ratios and, thus, decreased lung function in asthmatics. Therefore, Se or Cu/Se ratio may be a potentially important marker for mild to moderate asthma. Additional large-scale studies will be needed to clarify the exact roles of these trace minerals, Cu in particular, to evaluate conventional antioxidant therapeutic strategies for asthmatic patients.
Footnotes
DECLARATIONS