
Abstract
Background
The high-dose hook effect is a well-known phenomenon of two-site immunoassays including those for human chorionic gonadotrophin (hCG). We investigated the occurrence of a high-dose hook effect in six routinely available hCG assays using a sample with a total hCG concentration of approximately 3,600,000 IU/L.
Method
Dilutions of a sample with high hCG concentration were analysed using six common methods: Advia Centaur, Immulite 2000, Dimension RxL, Unicel DxI 800, Roche E170 and Abbott Architect. The measured concentrations and corresponding assay signals were obtained for each method. Performance was compared with manufacturer claims.
Results
Four of the tested platforms demonstrated a clear high-dose hook effect, while the other methods showed no hook effect at the highest level tested.
Conclusion
Our results indicate that the hook effect may occur in some hCG assays, although the risk of reporting falsely low results was in most cases at higher concentrations than those indicated in manufacturers' product information. Assay design plays a major role in its occurrence. Laboratories should be aware of the assay limitations in this regard.
Introduction
The high-dose hook effect is a phenomenon occurring in two-site immunoassays where at high analyte concentrations there is a decrease in the assay response signal. The hook occurs because the analyte concentration exceeds the binding capacity of both the capture and the labelled antibodies in the assay reagents, which results in incomplete formation of the immune complexes required for signal creation. This gives falsely low results, which may have catastrophic implications for patient care. 1 Miles et al. 2 first described high-dose hook effect in the literature in the early 1970s with the two-site immunoradiometric assay for ferritin, 3 and it remains a problem in modern laboratory practice. We experienced a falsely low result due to a high-dose hook effect with human chorionic gonadotrophin (hCG) measurement in a sample from an adult male with extragonadal germ cell tumour. This stimulated us to evaluate this effect in six commonly used assays for hCG and compare the results with the manufacturer claims.
Methods
Serum samples from a patient with extragonadal germ cell tumour with an hCG concentration of about 3.6 million IU/L (Advia Centaur-Total hCG) and normal male serum pool were mixed in varying proportions to produce samples of different hCG concentrations. Due to inadequate sample volume, the dilutions for the Roche analyser were performed using a different sample from the same patient with a concentration of approximately 2.3 million IU/L (Advia Centaur). The male pool had an hCG concentration below 2 IU/L. Samples were measured on the following analytical systems: Advia Centaur-Total hCG, Immulite 2000-Total hCG, Dimension RxL-Intact hCG (Siemens Diagnostics Solutions, Bayswater, VIC, Australia), Unicel DxI 800-Total hCG (Beckman Coulter, Yeerongpilly, QLD, Australia), Roche E170-Total hCG (Roche Diagnostics, Castle Hill, NSW, Australia) and Architect-Total hCG (Abbott Diagnostics, North Ryde, NSW, Australia). The instrument readouts and measurement signals were recorded for each sample. The instrument signal corresponding with the upper limit of the instrument reporting range was determined by extrapolation from the results and the measurement signal data for each analyser was expressed relative to that determined for the upper limit of the reporting range (which is the concentration at which dilution is indicated).
Results
The signal readings from the analysers clearly demonstrated the hook effect for the Advia Centaur, Unicel DxI 800, Immulite 2000 and E170 with a peak signal occurring at about 20,000 IU/L for Advia Centaur and DxI 800, and at about 300,000 IU/L on the Immulite 2000 and E170. At higher hCG concentrations, the signal fell towards the range where a result may be produced (Figure 1a). By contrast, no hook effect was seen with the Dimension RxL and Architect up to the concentration level tested, although the signal did reach a plateau in both assays (Figure 1b).
Relationship between hCG concentration and assay signal for assays showing a hook effect (a) and not showing hook effect (b). The signal is expressed as multiples of the signal associated with the top of the assay reportable range. (a) Advia Centaur, Unicel DxI 800, Immulite 2000 and Roche E170. (b) Abbott Architect and Dimension RxL. hCG, human chorionic gonadotrophin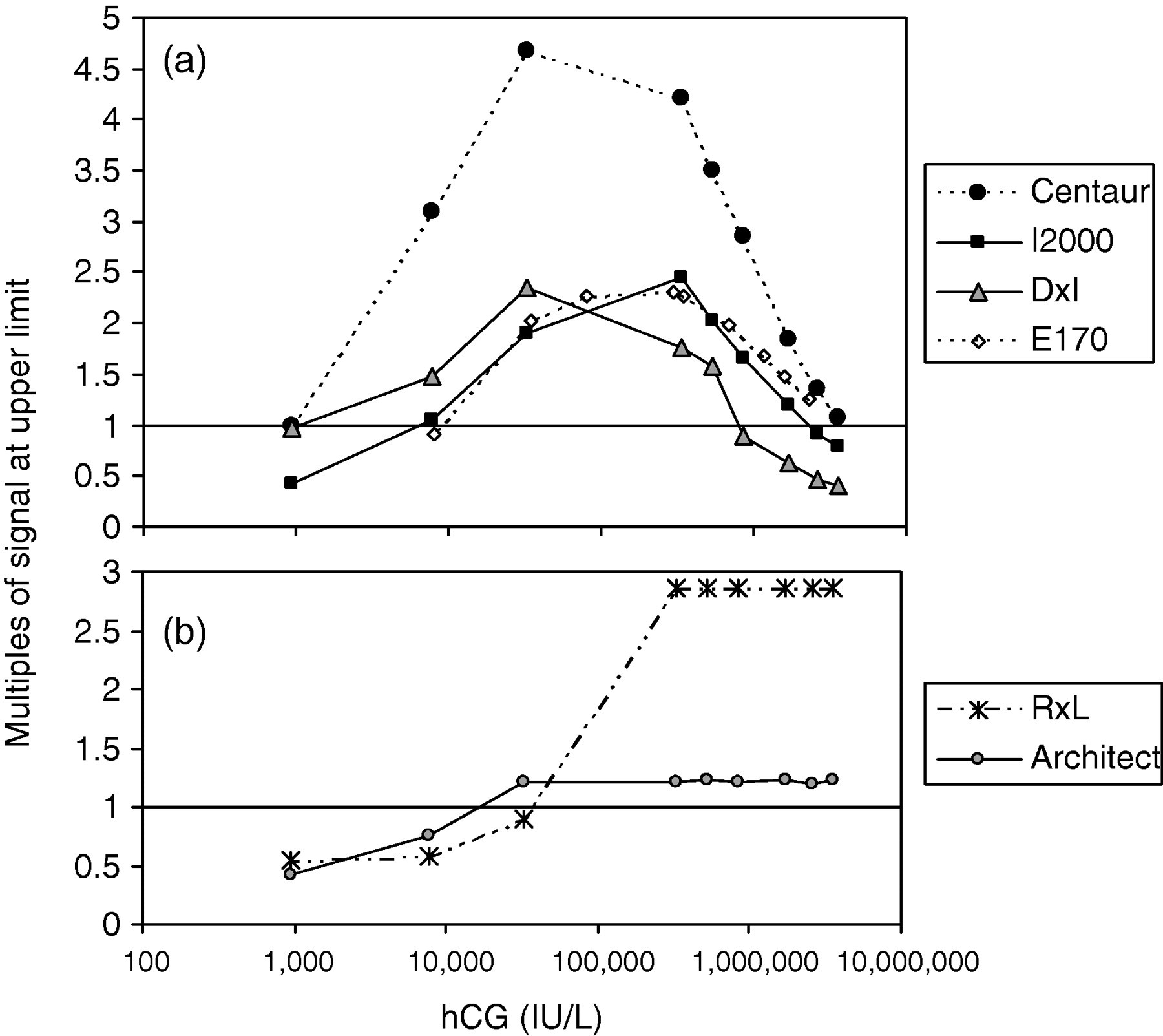
hCG assay details
hCG, human chorionic gonadotrophin
Note: (1) PI - product information; (2) Not provided by the manufacturer; (3) concentration at which a falsely low result may be obtained and (4) no evidence of hook effect up to 3.6 × 106
The samples at the greatest dilutions returned into the measuring range of the assay for all analysers. With one exception, the highly diluted samples gave values close to those expected based on the starting concentration and the dilutions performed. The exception was the Dimension assay with a claimed upper limit of 1000 IU/L (Table 1) where a sample with an expected value over 10,000 IU/L produced a measurable result (Figure 1b).
Discussion
Although high-dose hook effect is not frequently encountered in laboratory practice, it is crucial for the laboratory scientist to be vigilant and aware of its possible occurrence as it may directly influence patient management. 1,4 The assay design plays a major role in the occurrence of this effect. It is more commonly found in single-step, two-site immunometric assays, a popular format chosen for its specificity and speed, particularly with high-throughput analysers. 2,5 The assays most affected are those that have analyte concentrations that may range over several orders of magnitude, such as ferritin, urine albumin, tumour markers and some hormones. The incidence of high-dose hook effect can be reduced by adopting a sequential assay format with a washing step, e.g. Abbott Architect and Dimension RxL. The risk of issuing falsely low results can also be reduced by restricting the reporting range of the assay so that higher concentrations are required to bring the signal down to the reportable range where a result is reported without a warning flag.
In this article, we report levels of hCG at which high-dose hook effect may occur in six different methods and compare it with manufacturer claims. Advia Centaur, Unicel DxI 800, Immulite 2000 and E170, which employ a single-step sandwich immunoassay, showed a hook effect with a downturn of signal occurring at about 20,000 IU/L for the Centaur and DxI, at about 500,000 IU/L for Immulite 2000 and the E170. However, the level at which these analysers may produce an erroneous results occur at approximately 800,000 IU/L for the DxI, 2.3 million IU/L for the Immulite 2000 and 3.6 million IU/L for the Centaur and E170. These values are higher than those at which the hook occurs as there is an upper limit placed on the evaluation of the signal such that higher values are not reported and the need for dilution indicated. For the Immulite 2000, the concentration at which a false result might be obtained corresponded to the manufacturer claim, for the Unicel DxI 800 was below the manufacturer's claim, while for the Advia Centaur and E170 falsely low results were only seen at levels significantly higher than that quoted by the manufacturer. The Abbott Architect and Dimension RxL did not even show a downturn in signal at concentrations up to 3.6 million IU/L, which was the highest concentration we tested. Both Abbott Architect and Dimension RxL include a washing step before the addition of the second antibody, which removes excess antigen, thus decreases the likelihood of a hook effect. In both these analysers, however, the signal did reach a plateau, which may be due to limited amount of antibody or a limitation of the signal generation or detection. The assays also differ in the hCG variants detected with all assays reacting with intact hCG, the Architect and Centaur also reacting with hCGβ and the E170 and Immulite reacting with hCGβ and the Beta core fragment; 6 however, these specificities did not correlate with the different responses.
The manufacturers' product information showed that most manufacturers only claimed suitability for testing in pregnancy, with the exception of the Roche E170 hCG assay, for which a claim is made for use in oncology as well as in pregnancy. Thus, the assay limitations described here may not be relevant for the claimed assay uses as the concentrations tested are very unlikely in pregnancy. If the assays are used for non-pregnancy testing, then users should be aware of these limitations. It is also possible that the molecular form(s) of hCG in this oncology patient may not reflect those seen in pregnancy or in other cancer patients, which may lead to different assay responses. 7,8 Indeed, this may be a possible explanation for the lower recovery seen on the highly diluted samples measured on the Dimension analyser, which only detects intact hCG. 6
In summary, we have used serum from a patient with very high concentrations of hCG to investigate common assays for high-dose hook effect, with four out of six methods demonstrating the effect, but in most cases at higher hCG concentrations than claimed by the manufacturers.
DECLARATIONS