
Abstract
Background
Particle size of apoB-48 carrying lipoproteins in remnant-like lipoprotein particles (RLP) in postprandial plasma has not been well characterized.
Methods
Plasma lipids, lipoproteins and apolipoproteins in 12 healthy subjects were analysed after an oral fat load. RLP isolated by immunoaffinity gel from plasma of a normolipidaemic and a hyperlipidaemic subject in four hours after an oral fat load was fractionated by high-performance liquid chromatography (HPLC) and monitored by total cholesterol (TC), triglycerides (TG), apoB-48 and apoB-100.
Results
TC, low-density lipoprotein (LDL)-C and apoB did not change after an oral fat load, while TG, RLP-C, RLP-TG and apoB-48 increased significantly in postprandial plasma. HPLC profiles monitored by TC and TG revealed that major lipoproteins increased in RLP after an oral fat load was VLDL size particles. The percentage of RLP-TG in total TG and the ratio of RLP-TG/RLP-C were significantly increased in four hours after an oral fat load compared with the fasting state (P < 0.01). RLP in four hours after an oral fat load fractionated by HPLC and monitored by TC, TG, apoB-48 and apoB-100 revealed that VLDL size or smaller particles were the major lipoproteins.
Conclusions
ApoB-48 carrying lipoproteins in RLP isolated from a normolipidaemic and a hyperlipidaemic subject after an oral fat load showed a similar particle size with apoB-100 carrying VLDL remnants. Therefore, the most apoB-48 carrying particles found in postprandial RLP can be classified as CM remnants. The majority of remnants in the postprandial state were not CM remnants, but VLDL remnants.
Introduction
Triglyceride-rich lipoproteins (TRL) in plasma are known to contain chylomicrons (CM), very low-density lipoproteins (VLDL) and their remnants. TRL significantly increases in postprandial plasma and known to be a major risk factor for coronary heart disease (CHD) as postprandial hyperlipidaemia reported by Zilversmit in 1979. 1 CM is secreted from the intestine after food intake, carrying apoB-48 apolipoprotein (exogeneous lipoproteins), while VLDL are secreted from the liver and carry apoB-100 apolipoprotein (endogeneous lipoproteins). Remnant-like lipoprotein particles (RLP) significantly increase after food intake and remain for a longer period of time in plasma, containing both apoB-48 (CM) and apoB-100 (VLDL) as a subset of triglycerides (TG)-rich lipoproteins with the characteristics of apoE, apoCs and cholesteryl ester-rich. 2–8 Many in vitro and in vivo studies have shown the atherogenicity and proinflammatory properties of RLP, which revealed the strong similarity with oxidized LDL. 9,10
Classically, plasma CM, VLDL and their remnants have been measured by sequential density gradient ultracentrifugation 11 and many studies on postprandial hyperlipidaemia were reported using the method. In postprandial hyperlipidaemia, the most markedly increased fraction was observed in the Sf 60-400 lipoproteins as large VLDL, whether measured as TG or retinol palmitate responses. 12–14 No significant increase in small VLDL such as intermediate density lipoproteins (IDL, Sf 12-20) has been reported in the postprandial state, even though IDL has often been defined as typical remnant lipoproteins.
As RLP increases significantly in the postprandial state and its assay method uses anti apoB-100 specific antibody which does not recognize apoB-48, 2,3 the arguments have continued for many years that RLP assay measures CM, not just CM remnants in plasma in the postprandial state. Therefore, it is now necessary to clarify if postprandial RLP does or does not contain large nascent CM as a major component. We have tried to analyse the particle size of apoB-48 carrying lipoproteins and apoB-100 carrying lipoproteins in RLP fractionated by high-performance liquid chromatography (HPLC) method. Particle size is one of the definitive characteristics for distinguishing CM remnants from CM.
The presence of CM remnants in postprandial plasma was first reported by Redgrave. 15 The half-life of CM has been shown to be 5–10 min in plasma, indicating very short half-life as compared with other lipoproteins. The presence of apoB-48 and ratio of apoB-48/apoB-100 in RLP were reported by Marcoux et al. 7 and Campos et al. 8 by using a semi-quantitative sodium dodecyl sulphate-polyacrylamide gel electrophoresis method, isolating RLP from hyperlipidaemic plasma. These results revealed significant predominance of apoB-100 in RLP compared with apoB-48. However, the particle sizes of apoB-48 and apoB-100 carrying lipoproteins in RLP were still unknown from these results. As a highly sensitive apoB-48 enzyme-linked immunosorbent assay (ELISA) was developed by Kinoshita et al., 16 we have evaluated the usefulness of measuring apoB-48 in human plasma and atherosclerotic plaques. 17,18 This apoB48 ELISA made it possible to measure apoB-48 protein in large TG-rich lipoprotein particles in serum by detergent treatment (0.1% Triton X-100) 16 and highly correlated with values obtained by gel scanning of TRLs (r = 0.82). 17 In this manuscript, we have further elucidated the particle size of apoB-48 carrying lipoproteins in postprandial RLP using the HPLC method 19,20 and compared the particle size with apoB-100 carrying lipoproteins in RLP.
Materials and methods
Subjects
Oral fat load was carried out in six male and six female (postmenopausal) Japanese volunteers aged 39–60 (mean 52 y) who were generally healthy with no apparent disease. Among 12 volunteers, three cases were with mild hyperlipidaemia (Type IIb). The study was conducted following the informed consent and was approved by the Ethical Committee of the Gunma University School of Medicine. All participants performed an oral fat tolerance test (OFTT) as previously reported. 21 Briefly, after a 12-h fasting, the subjects ingested 17 g fat/m2 body surface area (OFTT cream, Jomo Foods, Takasaki, Japan). The test meal (OFTT cream) had a water content of 56.9%, while lipids accounted for 32.9%, protein for 2.5%, carbohydrates for 7.4% and minerals for 0.3%. The fat was 64.3% saturated, 29.3% monounsaturated and 3.5% polyunsaturated.
Blood samples were drawn before and two, four and six hours after an oral fat load. Plasma samples were kept frozen at −80°C until assay and isolation and fractionation of RLP.
Isolation of RLP from postprandial plasma
RLP was isolated by an immunoseparation method by Nakajima and co-workers. 2,3 Briefly, 0.2 mL aliquots of plasma were applied to columns containing 2 mL (1.0′2.5 cm) of immunoaffinity mixed gel containing two clones of monoclonal antibodies, Mab JI-H raised against human apoB-100 and Mab H-12 raised against human apoA-I (Japan Immunoresearch Laboratories, Takasaki, Japan). The plasma samples were incubated with the immunoaffinity mixed gels at room temperature for 30 min. Lipoproteins unbound to the gel (containing primarily CM and VLDL remnants) were eluted with 3.5 mL of 10 mmol/L phosphate-buffered saline (pH 7.2). The unbound fraction was concentrated by Amicon Ultra filter (Millipore, MA, USA) for HPLC analysis.
HPLC fractionation of RLP
RLP fractionation by HPLC was carried out by using a HPLC system, equipped with gel permeation columns (TSK Lipopropak XL, Toso, Tokyo, Japan). 20 RLP was fractionated into 0.35 mL of aliquot by this HPLC system for the determination of total cholesterol (TC), TG, apoB-48 and apoB-100.
Analyses of plasma lipids and lipoproteins
Plasma TC and TG concentrations were determined enzymatically by Determiner L-TC and Determiner L-TG (Kyowa Medex, Tokyo, Japan) on a Toshiba Auto-Analyser TBA-20R (Toshiba, Tokyo). RLP-C and RLP-TG were determined as described previously. 3 Briefly, the RLP fraction was obtained from plasma by using an immunoaffinity mixed gel containing monoclonal anti apoB-100 and anti apoA-I (JIMRO, Takasaki, Japan). Cholesterol and TG concentrations in the RLP fractions were determined by sensitive enzymatic assays (Determiner L-TC and Determiner L-TG, respectively; Kyowa Medex, Tokyo, Japan). ApoB-100 (JIMRO, Takasaki, Japan) and apoB-48 (Shibayagi, Shibukawa, Japan) were measured by ELISA. 16 Apolipoproteins A-I, A-II, B, C-II, C-III and E were determined by immunoturbidimetric assays (Sekisui Medical, Tokyo, Japan). The LDL-C and HDL-C were measured by homogeneous assay kits (Kyowa Medex, Tokyo, Japan).
Statistics
Data were analyzed with Stat View software (Version 5.0; SAS Institute Inc, Cary, NC, USA). The statistical significance of differences was determined by the Mann-Whitney U test. The test was used in variables with Gaussian distribution like plasma RLP-C and RLP-TG concentrations. P < 0.05 was considered statistically significant.
Results
Postprandial plasma lipid and lipoprotein levels in healthy volunteers
Postprandial plasma lipids and lipoproteins were significantly increased in two, four, six hours after an oral fat load in 12 volunteers. TC, LDL-C and apoB did not change; however, TG, RLP-C, RLP-TG and apoB-48 increased significantly in two, four, six hours after an oral fat load (P < 0.05 and P < 0.001, respectively, Table 1). Figure 1 indicates the statistical deference between the levels of TG, apoB-48 and apoB before and after an oral fat load. Similar increases after an oral fat load were observed between TG and apoB-48; however, no correlation was found between apoB. The percentage of RLP-TG in total TG was significantly increased from 12% to 48% in four hours, while RLP-C in total TG was slightly decreased after an oral fat load (t-test versus 0 h, *P < 0.05 and **P < 0.01, respectively, Table 2). There was a striking increase in the ratio of RLP-TG/RLP-C, which reflected the increase of particle size with the increase of TG, from 2.8 to 12.3, in four hours after an oral fat load (Table 2).
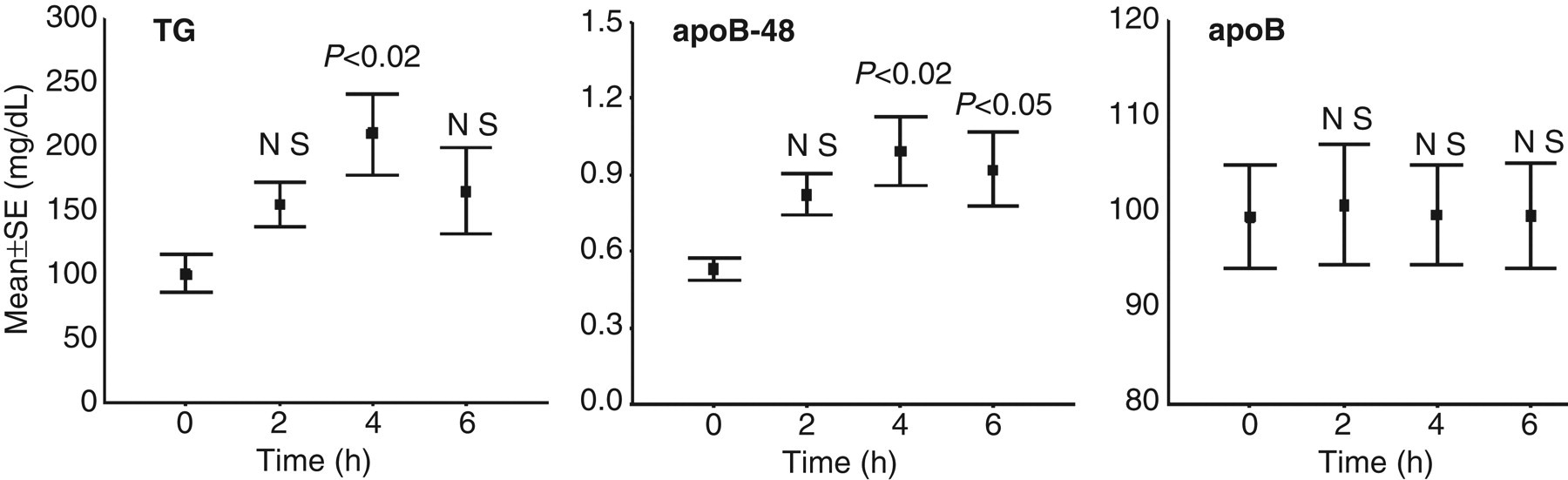
Postprandial differences of plasma TG, apoB-48 and apoB between before and after an oral fat load. TG showed very similar correlation with apoB-48, but not with apoB. TG, triglycerides
Serum levels of lipids and lipoproteins after an oral fat load in 12 normal Japanese volunteers (mg/dl)
TG, triglycerides; TC, total cholesterol; RLP, remnant-like lipoprotein particles
n = 12, by t-test verses zero h
*P<0.05, **P<0.01
Different ratios between TG and remnant lipoproteins after an oral fat load
TG, triglycerides; TC, total cholesterol; RLP, remnant-like lipoprotein particles
By t-test verses 0 h
*P<0.05, **P<0.01
Characteristics of RLP isolated from postprandial plasma
RLP isolated from plasma in 12 subjects after an oral fat load by the immunoaffinity mixed gel was significantly increased. Figure 2 shows typical profiles of RLP particle size in the range of VLDL to LDL in zero, two, four and six hours after an oral fat load when monitored by TC and TG with HPLC, using the same aliquots of immunoaffinity gel suspension solution in a normolipidaemic and hyperlipidaemic subject, respectively. CM or CM remnants (apoB-48) could be detected if any at void volume (retention time at 15 min). Figure 3a shows typical RLP profiles isolated from plasma of a normolipidaemic subject in four hours after an oral fat load. RLP was fractionated by HPLC and monitored by TC, TG apoB-48 and apoB-100 in each aliquot. As the isolated amount of RLP in normolipidaemic case was very small, the accuracy of TG and TC analysis was not satisfactory. Figure 3b shows typical RLP profiles in a mild hyperlipidaemic subject with Type IIb among the volunteers. The peak of TC and TG retention time in RLP fractionated by HPLC was almost identical with apoB-100 peak, but not with apoB-48 peak in Figure 3b. ApoB-48 concentration in RLP was much lower (almost 1/20) compared with apoB-100 in RLP. Also apoB-48 particle size was similar or smaller than that of apoB-100. Normolipdaemic case in Figure 3a had a peak of TG at similar retention time with apoB-48 and apoB-100, but not so clear as in Figure 3b (hyperlipidaemic case). These results clearly indicated that postprandial RLP have no apoB-48 particles in void fraction, which is categorized as nascent CM by this HPLC system. 19,20 ApoB-48 particles showed similar or smaller particle sizes (similar retention time) with apoB-100 particles in postprandial RLP. The scale (perpendicular axis) of apoB-100 (left) and apoB-48 (right) concentration is 20 folds different, but shows similar areas under the curve. Therefore, significantly higher concentrations of apoB-100 than apoB-48 in postprandial RLP with similar particle size were found in both normolipidaemic and hyperlipidaemic cases.
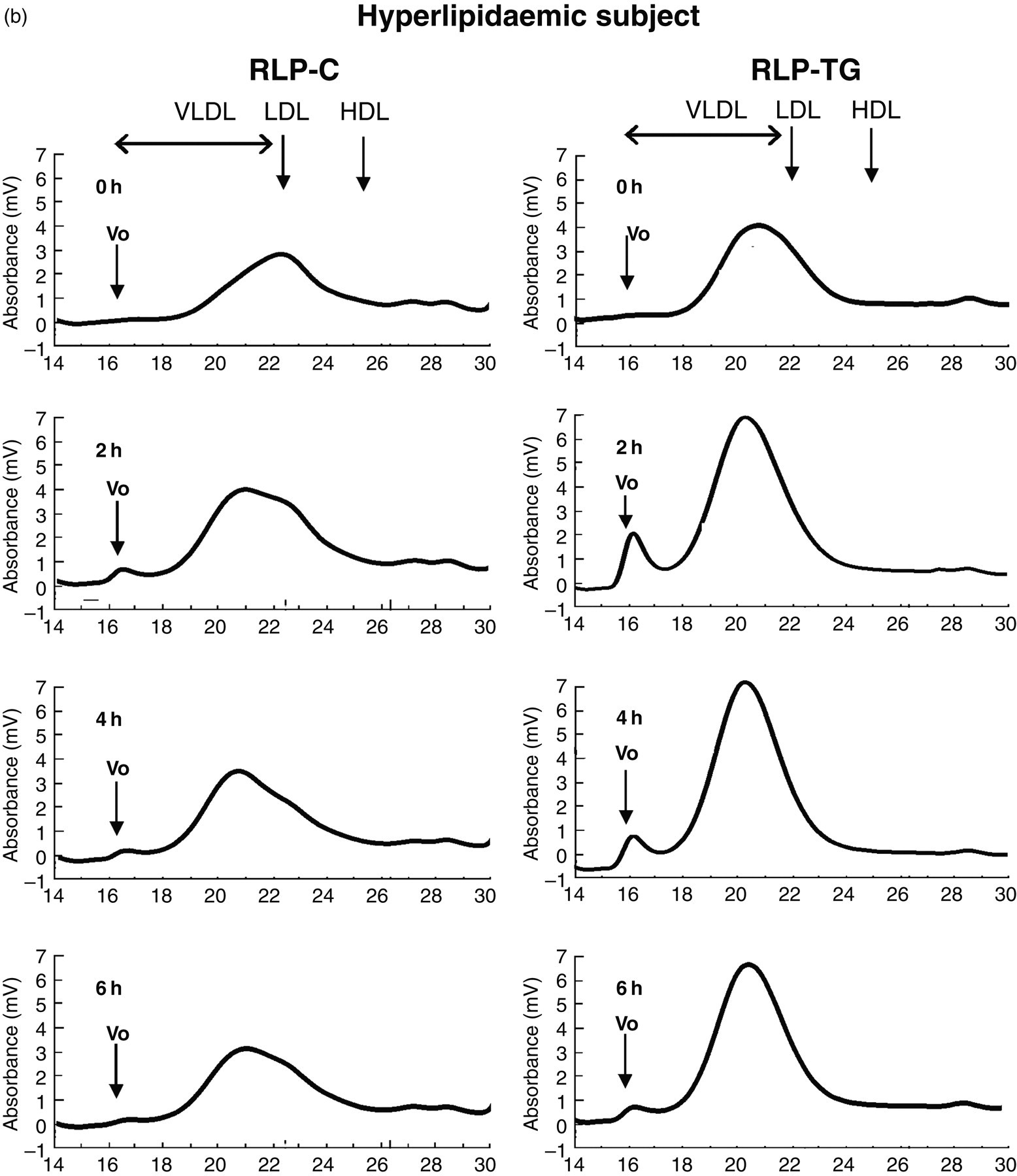
Typical RLP profiles monitored by TC (RLP-C) and TG (RLP-TG) in a normolipidaemic subject (a) and a hyperlipidaemic subject (b). The particle sizes were shown in the range of VLDL to LDL before (0 h) and after (2, 4, 6 h) an oral fat load. A small peak at void retention time was detected in two and four hours in both cases as TG-rich large lipoproteins. The clearance of VLDL fraction was significantly delayed in a hyperlipidaemic subject compared with a normolipidaemic subject. Elution positions of LDL and HDL particles were shown by arrows, respectively. RLP, remnant-like lipoprotein particles; TC, total cholesterol; TG, triglycerides
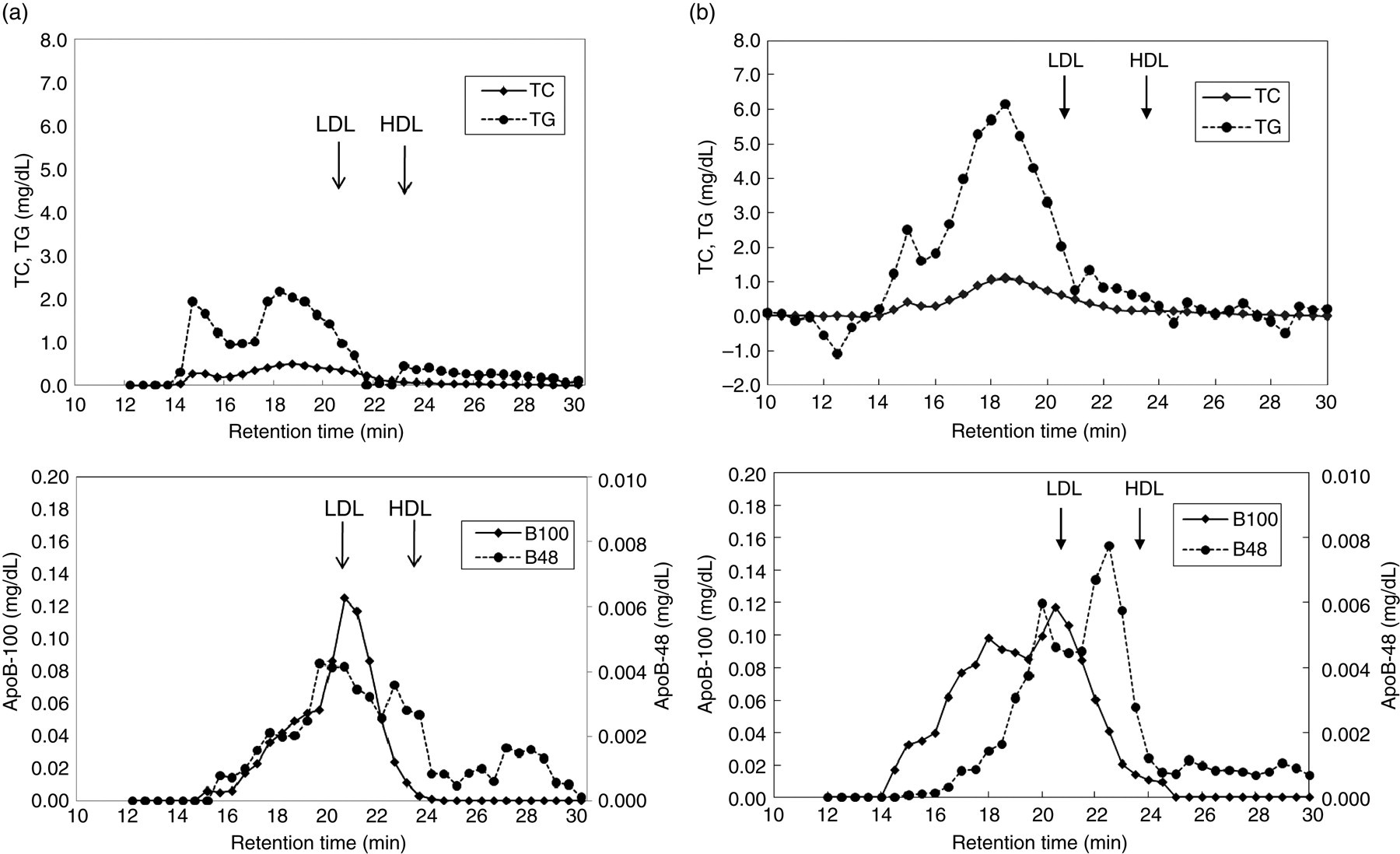
(a) A typical profile of postprandial RLP in a normolipidaemic subject. RLP was isolated and fractionated by HPLC from postprandial plasma of a normolipidaemic subject (fasting level: TC; 191, TG; 91, HDL-C; 69, LDL-C; 103, RLP-C; 5.0, RLP-TG; 16, apoB; 98, apoB-48; 0.44 mg/dL) in four hours after an oral fat load. RLP fractionated by HPLC was monitored by TC and TG (top) and monitored by apoB-48 and apoB-100 (bottom). The scale (perpendicular axis) of apoB-100 (left) concentration is 20 folds higher than that of apoB-48 (right), but shows similar areas under the curve. The major particles in RLP were VLDL size monitored by apoB-100, and comparatively smaller size of CM monitored by apoB-48. (b) A typical profile of postprandial RLP in a hyperlipidaemic subject. RLP was isolated and fractionated by HPLC from postprandial plasma of a hyperlipidaemic subject (fasting level: TC; 238, TG; 196, HDL-C; 53, LDL-C; 111, RLP-C; 7.0, RLP-TG; 69, apoB; 92, apoB-48; 0.86 mg/dL) in four hours after an oral fat load. RLP fractionated by HPLC was monitored by TC and TG (top) and monitored by apoB-48 and apoB-100 (bottom). The scale (perpendicular axis) of apoB-100 (left) concentration is 20 folds higher than that of apoB-48 (right), but shows similar areas under the curve. The major particles in RLP were VLDL size monitored by apoB-100, and comparatively smaller size of CM monitored by apoB-48. RLP, remnant-like lipoprotein particles; TC, total cholesterol; TG, triglycerides; HPLC, high-performance liquid chromatography
Discussion
Postprandial hyperlipidaemia has been known to be one of the major risk factors for CHD. 1,22 With this in mind, the principal objective of this study was to clarify whether RLP consists of nascent CM or remnants of apoB-48 carrying particles in the postprandial state. It has been discussed for many years ‘which are the major apoB-48 carrying particles in postprandial RLP, either CM or CM remnants’, because anti-apoB-100 antibody for RLP assay does not recognize both apoB-48 in CM and CM remnants. 2,3 To our knowledge, this is the first study that was aimed at determining the particle size of apoB-48 carrying lipoproteins in postprandial RLP.
The postprandial increase in TG has often been considered to be an increase in CM or CM remnants since Zilversmit 1 proposed postprandial chylomicronaemia as a risk of atherogenesis. Also as shown in Figure 1, apoB-48 increases significantly in parallel with TG in the postprandial state. Therefore, it has been often believed that a major subset of postprandial lipoproteins is CM or CM remnants, and not VLDL remnants. Furthermore, it is also known that apoB or LDL does not increase, rather slightly decrease in the postprandial state. 14 As the absolute concentration of apoB-100 is much greater than that of apoB-48 (more than 100 folds) in plasma, the slight decrease of apoB-100 (or total apoB) may hide the increase of apoB-100 in VLDL or VLDL remnants in the postprandial state.
Plasma concentration of TG, RLP-C, RLP-TG and apoB-48 in this study (Table 1) increased significantly after an oral fat load. Especially, apoB-48 increased in parallel with TG and remnant lipoproteins. Also the particle size of RLP predicted as RLP-TG/RLP-C ratio by Okazaki et al. 19 increased significantly in two, four hours and decreased in six hours after an oral fat load in normolipidaemic subjects as shown in Table 2 and Figure 2a, following the changes of total TG. The largest particles (highest RLP-TG/RLP-C ratio) were always detected at the highest concentration of RLP-C and RLP-TG after an oral fat load (Table 2). Judging from these results, large RLP may be derived from the liver, namely VLDL with apoB-100, but not CM with apoB-48 from the intestine. Because half-life of CM is only five minutes in blood and may not stay as nascent CM particles for longer period of time in blood. Only small amount of CM remnants that were not cleared through the receptors remained in blood in four hours as the particles with a similar half-life of VLDL.
As anti apoB-100 antibody used in RLP assay does not recognize apoB-48 because of the epitope specificity of this antibody, 2,3 it has been long suspected that RLP may contain large amount of nascent CM together with CM remnants. However, CM containing apoA-I are principally deleted from RLP by anti-apoA-I antibody coexisted in the immunoaffinity gel. 3 Only CM without apoA-I has been measured as RLP. However, it was still necessary to confirm if apoB-48 particles in RLP satisfied the definition of remnant lipoproteins. ApoB-48 particles found in significantly longer retention time than void retention time (smaller particles) can be classified as CM remnants followed by the remnant definition of Redgrave. 15
RLP isolated from postprandial plasma in this study was found to be rich in apoE and contained significantly less apoB-48 relative to apoB-100, indicating a very similar electrophoretic profiles (data not shown) to RLP detected in hyperlipidaemic or CHD patients in the fasting state as already reported. 2,3,23 The concentrations of apoB-48 and apoB-100 in RLP in plasma from sudden cardiac death (SCD) cases were determined by ELISA and compared with non-SCD, control death cases in our previous report. 24 The results indicated the predominance of RLP apoB-100 more than seven folds as compared with the concentration of RLP apoB-48 in postmortem plasma in SCD cases. Also the apoB-48/ apoB-100 ratio in RLP was shown to be significantly different under various physical conditions such as in Type III cases 7 and in drug-treated cases. 22
However, these results still forecast the possibility that apoB-48 particles may carry much more lipids in one particle, having significantly large particle size, than in one apoB-100 particle in RLP. Because CM or CM remnants are believed to carry significantly more lipids in one particle than in one VLDL particle. RLP-C and RLP-TG levels may reflect a large amount of lipids with a small amount of apoB-48 particles. Therefore, the determination of particle sizes of apoB-48 and apoB-100 carrying lipoproteins in postprandial RLP was necessary to be pursued by HPLC analysis. Figures 3a and b clearly show that the particle size of apoB-48 particle was not detected at void retention time, which reflects nascent CM, but was very similar or rather smaller than apoB-100 particles in postprandial RLP. These data were very similar to the profile of apoB-48 and apoB-100 in cardiovascular disease and SCD cases as we reported previously. 25 Interestingly, we often found apoB-48 peak fraction at large HDL retention time in RLP fractionated by HPLC, which may associate with the formation of HDL from CM.
The two cases shown in Figures 3a and b were the typical cases we experienced among 12 volunteers in this study. ApoB-48 profiles were variable including a number of peaks and the peak retention time, while interestingly the retention time of apoB-100 was very consistent and stable at VLDL and large LDL peak. These results were observed as extreme examples with extremely small apoB-48 particles in postmortem plasma. 18 Judging from these results, apoB-48 carrying lipoproteins in postprandial RLP are all CM remnants, not containing nascent large CM. Therefore, the particle number of apoB-48 and apoB-100 can be directly compared with RLP-C and RLP-TG concentration. Havel et al. 26 previously reported that CM is very rapidly metabolized into CM remnants in plasma with the dissociation of apoA-I. Therefore, we can define that most apoB-48 particles in RLP observed in postprandial plasma consisted of CM remnants.
As being reported by Karpe et al. 27 and Karpe, 28 CM is more susceptible to be lipolyzed by lipoprotein lipase (LPL) than VLDL. Therefore, the competition of lipoproteins to LPL superior to CM rather than VLDL may cause the formation and accumulation of VLDL remnants more easily than those of CM remnants in the postprandial state. Therefore, the accumulation of large RLP particles in four hours after an oral fat load may be the results of delayed metabolism of VLDL by LPL activity.
The increase in the number of apoB-100 particles in RLP (VLDL remnants) is actually far greater than that of apoB-48 particles (CM remnants) in the postprandial state as reported previously. 4,24 Of note, the accumulation of large TRL apoB-100 particles seems to be a particular characteristic for hypertriglyceridaemic patients with CHD compared with healthy hypertriglyceridaemic subjects, suggesting a link between accumulation of large VLDL and development of atherosclerosis. 27,28
In this study, we have clarified that large VLDL remnants with apoB-100 monitored by TC and TG in RLP are the major subset of remnants increased in the postprandial plasma. ApoB-48 lipoproteins in RLP are small sized and are present in small amounts in postprandial RLP as CM remnants. The increase of IDL as remnants in the postprandial plasma has not been observed after food intake. 12–14 Therefore, IDL may not be an adequate subset of remnant lipoproteins to determine in the postprandial plasma. Recently, the prospective studies in large populations in Japan, Denmark and the USA have shown that remnant lipoproteins in non-fasting plasma play an important role for the cardiovascular events. 29–31 This phenomenon is associated with the high correlation between postprandial TG and RLP-TG, indicating that increased TG in the postprandial state is mostly derived from increased RLP-TG. 32 Therefore, the measurement of remnant lipoproteins for diagnostic purpose is most meaningful in postprandial hyperlipidaemia. Type III is a typical postprandial dyslipidaemia associated with the highly increased apoB-48 in plasma. 7
In conclusion, these results suggested that apoB-48 carrying particles in RLP isolated from healthy subjects after an oral fat load showed similar particle size with apoB-100 carrying VLDL remnants. Therefore, apoB-48 particles in RLP are mostly CM remnants, not containing nascent CM. The majority of remnants in the postprandial state are not CM remnants, but VLDL remnants.
DECLARATIONS