
Abstract
Background
Difficulty in distinguishing congestive heart failure (HF) from other causes of dyspnoea in the emergency department (ED) may result in delay in appropriate treatment and referral. Although the diagnostic value of serum amino-terminal pro-B-type natriuretic peptide (NT-proBNP) is well documented, the impact on diagnostic certainty of providing these results to ED physicians is not well studied. We sought to determine the effect of providing NT-proBNP results on diagnostic certainty of physicians managing patients presenting to the ED with suspected HF.
Methods
A randomized controlled study was conducted in 68 patients presenting to the ED with dyspnoea. ED clinicians initially rated the probability of HF as the cause of dyspnoea without the knowledge of the result. A scale of 1–7 was used, with 1 representing a high degree of certainty of a diagnosis other than HF and 7 representing a high degree of certainty of HF being the cause of dyspnoea. In 38 patients, the ED physician then reassessed the probability of HF as the cause of dyspnoea after receiving the NT-proBNP result. A cardiologist blinded to the NT-proBNP result determined the final diagnosis after review of medical records and investigations.
Results
Providing the NT-proBNP result reduced diagnostic uncertainty, defined as a test score of 3–5, from 66% of cases to 18% of cases (P < 0.0001) and improved diagnostic accuracy from 53% to 71% (P = 0.016).
Conclusion
Measurement of NT-proBNP concentrations reduces diagnostic uncertainty and improves diagnostic accuracy in patients presenting to the ED with dyspnoea and possible HF.
Introduction
Although dyspnoea is a common presentation to the emergency department (ED), the diagnosis is often initially uncertain. Heart failure (HF) is a leading cause of dyspnoea, particularly among individuals aged >65 y. With the ageing of the population and improved survival of patients with cardiovascular disease, the health burden and number of presentations to ED with HF are likely to become more prevalent, increasing the importance of accurate diagnosis and management. 1,2 Prompt and accurate diagnosis of the cause of dyspnoea prevents delays in appropriate treatment and may reduce morbidity and mortality. 3
B-type natriuretic peptide (BNP) is secreted from the cardiac ventricles as the pro-hormone proBNP, in response to volume expansion and increased wall tension. 4 BNP is cleaved from the C-terminal end of proBNP, with NT-proBNP being cleaved from the N-terminal end. The concentrations of BNP and NT-proBNP rise with both systolic and diastolic HF and may aid in differentiating between HF and non-HF causes of dyspnoea. 5 Although the relationship between NT-proBNP concentrations and HF is well documented, few studies have examined the clinical utility of promptly providing the NT-proBNP result to ED physicians in helping to establish a diagnosis for the cause of dyspnoea.
The purpose of this study was to evaluate the effect of providing the NT-proBNP result to ED physicians on diagnostic uncertainty and accuracy in patients presenting with dyspnoea.
Methods
A prospective, randomized, controlled study was conducted of 68 patients with dyspnoea, presenting to the ED of a tertiary referral hospital. NT-proBNP was measured in all patients, with the majority being tested from the blood taken at the first venipuncture in the ED. Where blood samples taken were inadequate, a second venipuncture was performed. The ED clinician was asked to evaluate the probability of HF being the cause of dyspnoea on a scale of 1–7, prior to the knowledge of the NT-proBNP result. A score of 1 represented high certainty that the diagnosis was not HF while 7 represented a high certainty of HF being the cause for dyspnoea. Patients were preferentially recruited in whom there was a level of uncertainty as to the diagnosis.
In 38 of the patients, the ED clinician was provided the NT-proBNP result and asked to re-evaluate the likelihood of HF being the cause of dyspnoea. The diagnosis without prior knowledge of the NT proBNP concentration was deemed the ‘pretest’ score, and the diagnosis influenced by the NT-proBNP concentration was termed the ‘post-test’ score. Pre- and post-test score comparison formed the basis of this study.
The remaining 30 patients were allocated to the control group, with the clinician remaining blinded to the NT-proBNP result. Randomisation to either the study or control groups was based on a pre-assigned enrolment number on the patient consent form, with allocation to the study or control group alternating between odd or even enrolment numbers on a weekly basis. Weekly variation in the number of patients enrolled in the study was therefore the main factor influencing the difference in numbers between the two groups. Not all patients who were eligible consented to inclusion in the study.
In addition to the assessment by the ED clinician, an independent cardiologist made a retrospective diagnosis for the cause of dyspnoea, blinded to the NT-proBNP result. The appraisal was based on review of the notes, examination findings and investigation results as documented by the ED and treating clinicians. Chest radiography was classified as indicating left ventricular failure in the presence of pulmonary venous congestion, pulmonary interstitial oedema or bilateral pleural effusions. New ischaemic changes on the electrocardiograph (ECG) were defined as Q waves, ST segment depression or elevation, or T wave inversion not present on previous ECGs.
Patients were classified as having a history of cardiac failure based on medical records and history as given by the patient at the time of review in the ED. The diagnosis made by the cardiologist was deemed the accurate diagnosis for the cause of dyspnoea. Using the cardiologist's final diagnosis, patients were classed into one of three categories, based on classifications as described in previous studies. 6 The categories were (1) no history of HF and non-HF cause of dyspnoea; (2) history of HF, but non-HF cause of dyspnoea; and (3) HF as cause of dyspnoea.
Written consent was obtained from all patients included in this study, and approval was obtained from the Hospital Ethics Committee.
NT-proBNP measurement was performed by an electrochemiluminescence immunoassay on the Modular Analytics E170 analyser (Roche Diagnostics, Australia), with analytical variation CVa 4.5% and 4.0% at 220 and 700 ng/L, respectively.
Statistical analysis
Analysis of statistical significance was performed by χ 2 test and paired t-test using Sigma Stat. A P value of <0.05 was considered statistically significant.
Results
The demographics for the study population are shown in Tables 1 and 2. The age range was 27–95 y, with a mean of 73 ± 16 y. Thirty-eight were women (56%) and 30 (44%) were men. A history of HF was present in 24 (35%) of the participants. The final diagnosis for the cause of dyspnoea, as determined by the independent cardiologist, was HF in 27 (40%) of cases. Causes of dyspnoea other than HF included exacerbation of chronic obstructive pulmonary disease, pneumonia, malignant pleural effusion, interstitial lung disease, lung cancer, primary pulmonary hypertension, anaemia and diaphragmatic weakness. Since prior studies have shown that NT-proBNP concentrations increase with age, 7,8 the following age-defined values for the diagnosis of HF were used, as defined in previous studies 9 : age <50 y, NT-proBNP >450 pg/mL; age >50 to <75 y, NT-proBNP >900 pg/mL; age >75 y, NT-proBNP >1800 pg/mL. Using these values as a cut-off and the cardiologist's diagnosis as reference, sensitivity was 81%, specificity was 66%, positive predictive value was 61% and negative predictive value was 84%.
Clinical characteristics and pretest probability
HF, heart failure; CCF, congestive cardiac failure; MI, myocardial infection; PND, paroxysmal nocturnal dyspnoea; JVP, jugular venous pressure; ECG, electrocardiograph
*All patients reported exertional dyspnoea
Clinical characteristics in NT-proBNP blinded (control) and NT-proBNP revealed groups
HF, heart failure; CCF, congestive cardiac failure; MI, myocardial infection; PND, paroxysmal nocturnal dyspnoea; JVP, jugular venous pressure; NT-proBNP, amino-terminal pro-B-type natriuretic peptide; ECG, electrocardiograph
*All patients reported exertional dyspnoea
The NT-proBNP concentration matched the cardiologist's diagnosis in 77% (23/30) of patients in the control group, and 68% (26/38) in the experiment group.
In 13 of the 14 patients in whom the NT-proBNP was elevated, but HF was not diagnosed by the cardiologist, an alternate cause for the elevated values was readily identifiable. These causes included the presence of atrial fibrillation, an acute coronary syndrome, renal impairment, sepsis and a history of HF. 10–14 When patients with the above causes of NT-proBNP elevation were excluded, the NT-proBNP matched the diagnosis of the cardiologist in 49 of 55 of cases (89%).
The median NT-proBNP result was 406.5 pg/mL for patients with no previous history of HF, and 3411.5 pg/mL for patients with a known previous history of HF.
The median NT-proBNP result was 3458 pg/mL for the ‘HF as cause of dyspnoea’ group, 1670 pg/mL for the ‘history of HF, but non-HF cause of dyspnoea’ group and 1652 pg/mL for the ‘no history of HF and non-HF cause of dyspnoea’ group (Figure 1).
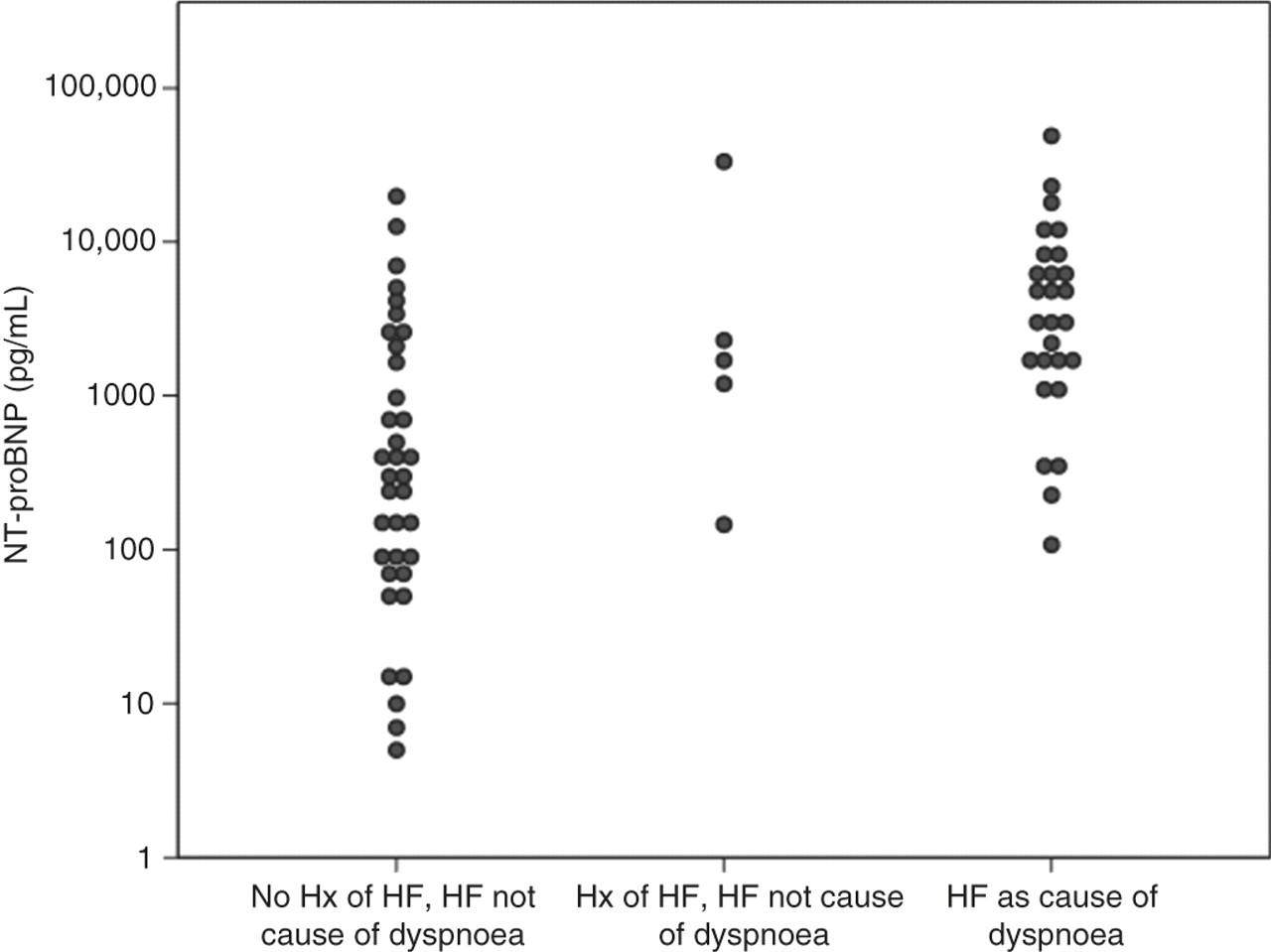
Relationship between cause of dyspnoea and NT-proBNP concentration. NT-proBNP, amino-terminal pro-B-type natriuretic peptide
NT-proBNP was elevated in 33% (12/36) with ‘no history of HF and non-HF cause of dyspnoea’, 40% (2/5) with ‘history of HF, but non-HF cause of dyspnoea’ and 81% (22/27) with ‘HF as cause of dyspnoea’ (Figure 2).
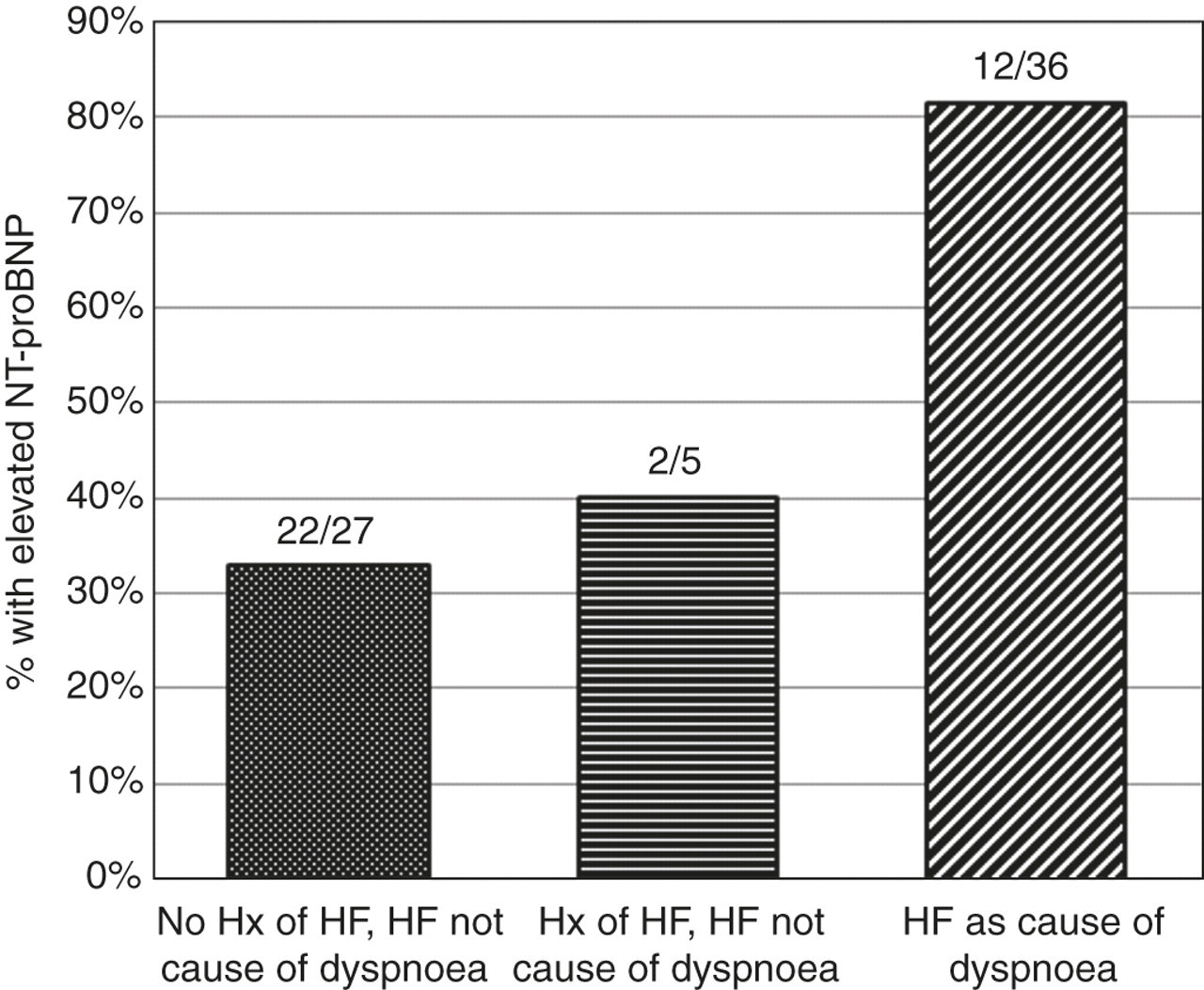
Percentage of patients with elevated NT-proBNP. NT-proBNP, amino-terminal pro-B-type natriuretic peptide; HF, heart failure
Overall, the ED clinician made the correct diagnosis for the cause of dyspnoea in 59% (40/68) of patients without knowledge of the NT-proBNP result, using the cardiologist's diagnosis as the accurate diagnosis (Table 3).
Diagnostic accuracy
NT-proBNP, amino-terminal pro-B-type natriuretic peptide
In the experiment group, the ED clinician made the correct diagnosis in 53% (20/38) of patients prior to knowing the NT-proBNP result (pretest). Diagnostic accuracy increased to 71% (27/38) after feedback of the NT-proBNP result (P = 0.016) (Table 3).
No adverse events from measurement of NT-proBNP concentration were recorded.
Diagnostic certainty
Overall 62% (42/68) were initially given a pretest score of 3, 4 or 5, indicating uncertainty as to whether HF was the cause of dyspnoea. In the control group, 57% (17/30) were given a score of 3, 4 or 5, with the clinician remaining blinded to the NT-proBNP at all times. In the experiment group, 66% (25/38) of patients were given a score of 3, 4 or 5, which reduced to 18% (7/38) after the NT-proBNP result was revealed (P < 0.0001) (Figure 3, Table 4).
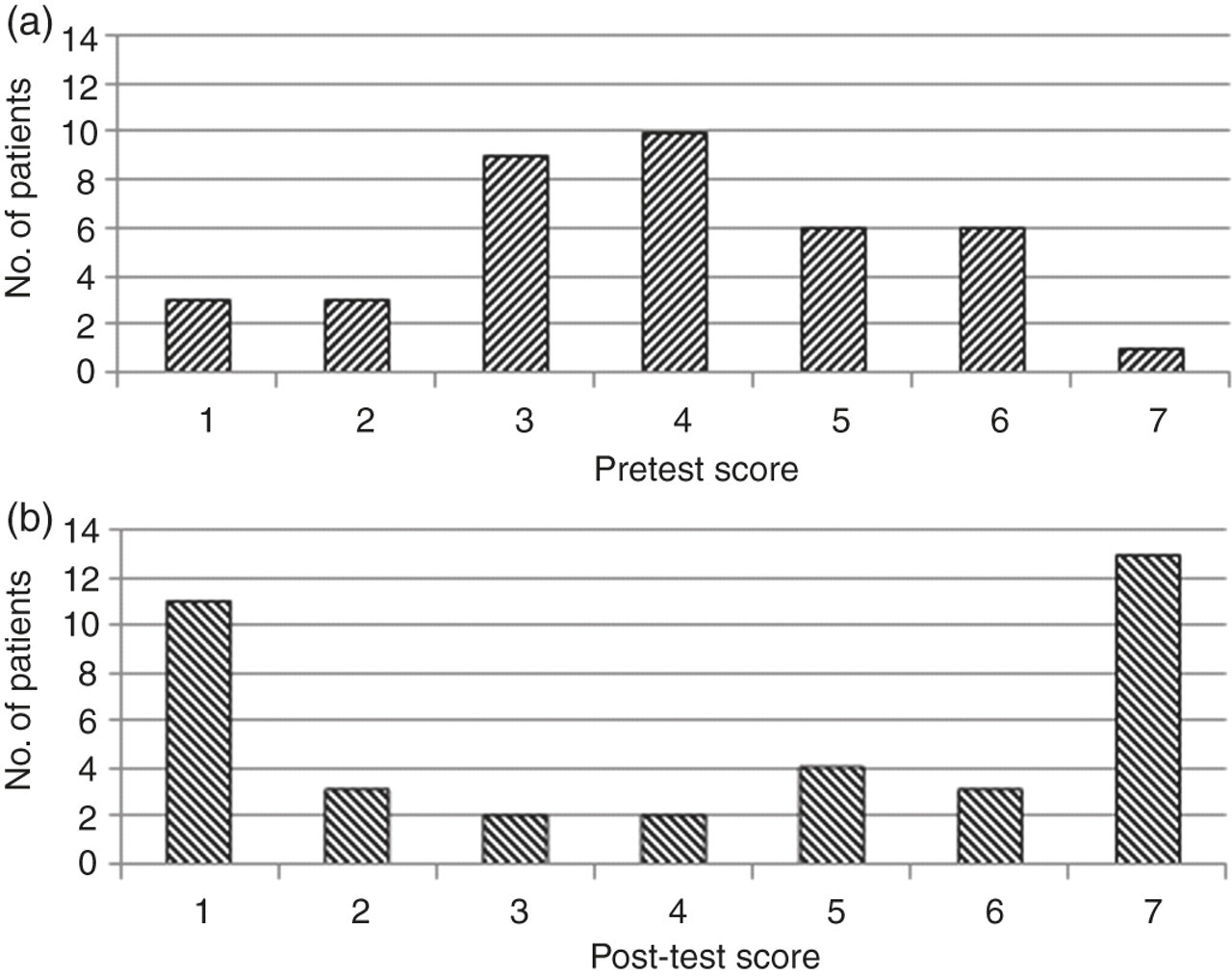
(a) Pretest probability of HF. (b) Post-test probability of HF. Diagnostic certainty expressed as Likert score (1–7) where 1 is high probability that diagnosis is not HF, 7 is high probability that diagnosis is HF and scores 3–5 represent diagnostic uncertainty. Provision of NT-proBNP results led to a significant reduction in diagnostic uncertainty (from 66% to 18% with score of 3–5, P < 0.0001). NT-proBNP, amino-terminal pro-B-type natriuretic peptide; HF, heart failure
Diagnostic uncertainty
NT-proBNP, amino-terminal pro-B-type natriuretic peptide
When a score of 4 alone was considered to be indicative of diagnostic uncertainty, overall 24% (16/68) of patients received this score as a pretest score. Considering the control group alone, 20% (6/30) of patients were given a score of 4 (Table 4).
In the experiment group, 26% (10/38) of patients were initially given a pretest score of 4, which reduced to 5% (2/38) after the NT-proBNP result was made available (P = 0.007).
In cases where the pretest score was rated 1, 2, 6 or 7 reflective of the ED clinician's confidence in their diagnosis for the cause of dyspnoea, only two clinicians changed their diagnosis after feedback of the NT-proBNP result, and, in one of these cases, the diagnosis was changed to the incorrect diagnosis.
The average duration of hospital admission was 8.1 ± 9.0 d in the group where the NT-proBNP was blinded throughout the length of admission, and 8.6 ± 6.4 d in the group where the NT-proBNP was made available after initial assessment.
Using Spearman's test there was a statistically significant correlation between the NT-proBNP concentration and the length of hospital admission (r s = 0.324, P = 0.007), with an elevated NT-proBNP concentration being associated with an increased length of hospital stay (Figure 4).
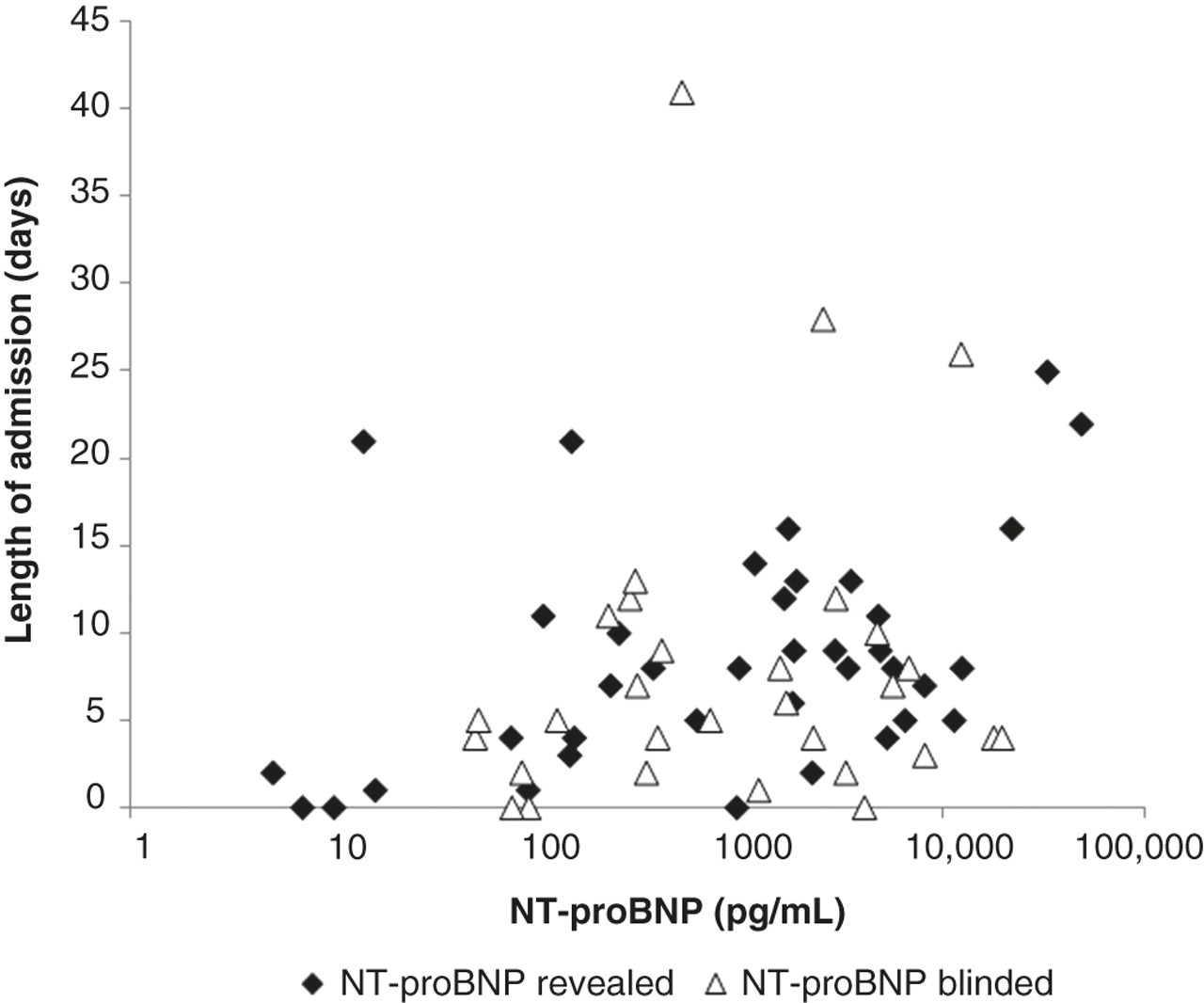
NT-proBNP concentration and length of admission. There was a statistically significant correlation between the NT-proBNP concentration and the length of hospital admission (r s = 0.324, P = 0.007) (Spearman's test). NT-proBNP, amino-terminal pro-B-type natriuretic peptide
Discussion
The measurement of NT-proBNP reduced the diagnostic uncertainty of emergency room regarding the diagnosis of HF. Diagnostic uncertainty, expressed as a score of 3–5 on a 7-point Likert scale, was reduced from 66% to 18% (P < 0.0001) with provision of the NT-proBNP concentrations. This reduction of uncertainty was associated with an increase in the correct diagnosis (53–71%, P = 0.016), with a cardiologist blinded to the BNP result as the reference. While these findings are consistent with previous reports that have highlighted the potentially important role of NT-proBNP testing, 3,5,6,8,15–19 few studies have specifically focused on diagnostic uncertainty. Green et al. 3 demonstrated the clinical importance of reducing diagnostic uncertainty in patients presenting with dyspnoea, by showing that clinical uncertainty is associated with increased morbidity and mortality in patients presenting with dyspnoea, and that NT-proBNP testing could reduce clinical uncertainty. These findings are supported by data from this study, and suggest that NT-proBNP testing in patients presenting with dyspnoea may result in reduced morbidity and mortality.
The benefits of NT-proBNP testing on diagnostic accuracy have been established in previous studies. 3,15–17,19 In our study, where we particularly focused on recruiting patients with a high level of initial uncertainty, ED clinicians made the correct diagnosis for the cause of dyspnoea in only 59% of patients. This reinforces the view that diagnosing the cause of dyspnoea can be difficult and that measures to enhance accuracy of diagnosis are needed. Earlier and more accurate diagnosis of HF in patients presenting to the ED could facilitate earlier treatment, and allow improvements in clinical outcomes. 3
The use of BNP testing in patients presenting to the ED with dyspnoea has been shown to be cost-effective, with improvements in diagnostic accuracy leading to reduced costs of treatment. 16,17
The findings of this study reinforced the accuracy of the age-defined cut-off values for NT-proBNP elevation used, while also highlighting the need to consider non-HF causes of elevated NT-proBNP.
In the present study, the positive predictive value of 61% and negative predictive value of 84% for NT-proBNP indicate that the level must be used in conjunction with other clinical data. In 13 of 14 patients, an alternative cause could be found for an elevated concentration in the absence of a current HF diagnosis. These conditions, which included atrial fibrillation, an acute coronary syndrome, sepsis and renal impairment, 10–14 were not uncommon in this study population. A history of HF can also result in an elevated NT-proBNP in the absence of an acute decompensation, when dyspnoea is not due to HF. 15,18
In patients with a prior history of HF, knowledge of the baseline NT-proBNP concentration could assist in differentiating between NT-proBNP elevation due to clinically stable disease, or due to an acute decompensation causing dyspnoea. 18 This was not available in the present study.
Normal concentrations of NT-proBNP are accurate for excluding HF as a cause of dyspnoea. Accordingly, given its negative predictive value, NT-proBNP measurement in patients with non-HF causes of NT-proBNP elevation is a powerful tool in clinical practice.
Limitations
The main limitation in the study is the small number of patients enrolled, which resulted in inadequate power to examine differences in length of stay, or cost-efficacy measures that would reflect the benefits of earlier and more accurate diagnosis. Despite the small number of participants the study was still able to demonstrate statistically significant improvements in diagnostic uncertainty and accuracy.
The negative predictive value of 84% for proBNP is less than that seen in other studies; however, it may reflect the subject population and the use of a single cardiologist reviewing clinical notes of varying quality retrospectively. The emphasis on recruiting patients in whom a high level of diagnostic uncertainty was present may also have contributed to the reduced specificity.
Conclusion
In patients presenting to the ED with dyspnoea, there is often uncertainty as to the correct diagnosis. In a randomized, prospective, controlled study, NT-proBNP testing reduces diagnostic uncertainty and improved accuracy. The study findings lend support to the value of measuring NT-proBNP in patients presenting with dyspnoea, especially when there is initial uncertainty regarding the diagnosis. In view of potential non-HF causes of raised NT-proBNP, this measurement needs to be considered together with the history, clinical findings and other diagnostic tests.
DECLARATIONS