
Abstract
Background
Both Roche and Abbott have released new glucose meter strips. They supply the entire Australian hospital market. The present study compared the performance of the new strips utilizing various specimen types (capillary, venous lithium heparin whole blood, venous lithium heparin plasma and serum) and evaluated how well they comply with the International Standards Organization (ISO) 15197 criteria.
Methods
The study included imprecision, patient comparison and interference studies. Participants with and without diabetes were recruited to evaluate the performance of various specimen types against the Beckman DxC800 glucose method. The strips were tested for different interferences: galactose, maltose, lactose, Icodextrin, Intragam, paracetamol, sodium, ascorbic acid, variable strip storage temperature, haematocrit, haemolysis and lipaemia.
Results
The imprecision of the two strips was ∼5% or less, except for the Abbott strip at very low values (1.4 mmol/L), ∼7%. In total, 78% and 84%, respectively, of the results from the finger prick capillary specimens with the Roche (Accu-Chek Performa meter) and Abbott (Optium Xceed meter) strips, not 95% or greater as recommended by the ISO guideline, were within the recommended limits compared with reference plasma estimation on laboratory analysers. Galactose, ascorbic acid, haematocrit and sodium on the Roche and ascorbic acid and haematocrit on the Abbott strip continue to interfere to a variable degree with the glucose measurement.
Conclusion
Analytically small differences exist between the glucose meter strips. The most significant analytical difference with the strips was at low glucose levels when compared with laboratory analyses and this may be of clinical importance. The impact of some of the interferences is variable between the two strips. Individuals, health-care professionals and health-care institutions should consider these data when selecting glucose meters for the management of people with diabetes mellitus.
Introduction
The American Diabetes Association (ADA) recommends self-monitoring of glucose using glucose meters or other point of care devices at least once a day to reduce the impact of complications arising from poor glycaemic control. 1 Although some studies report neither self-monitoring of blood glucose (SMBG) testing nor its frequency is associated with glycaemic benefit in type 2 diabetic patients, SMBG may still be of value in the identification and prevention of hypoglycaemia and in assisting with dose adjustments in insulin-treated patients. 2 What is clear is that encouraging SMBG in people with diabetes mellitus results in lower complication rates. 3
As the incidence of diabetes continues to increase, the number of people relying on glucose meters for improved glycaemic control will similarly increase. Furthermore, currently at any point in time in hospital 7–12% of inpatients have a diagnosis of diabetes 4,5 and the number of patients hospitalized with diabetes will continue to increase. Inpatients with diabetes often have coexisting medical conditions (e.g. hypo- or hypernatraemia, altered haematocrit and lipaemia) and on therapies (paracetamol, Intragam, peritoneal dialysis and vitamin C) that may potentially interfere with the accuracy of measurement of glucose via glucose meters. Roche Accu-Chek Performa (Roche Diabetes Care, Mannheim, Germany) and Abbott MediSense Optium (Abbott MediSense, Bedford, MA, USA) range of glucose meters currently supply the entire Australian hospital network, and hold ∼95% of the total market share between them. 6 Both manufacturers have released new modified strips and claim improved performance characteristics. The actual analytical activity occurs in the strip, thus the accuracy of the results is almost entirely dependent on the strip's composition and technical sophistication.
A common misperception by both health professionals and patients is that glucose meters correlate well with laboratory analysers. Using these results interchangeably can lead to misinterpretation of the glycaemic status. Besides the technological differences between glucose meters and laboratory analysers, the specimen type used in analysis can be a pivotal reason for differences between results; finger prick capillary blood with glucose meters versus either plasma (anticoagulated liquid component of blood) or serum (liquid component of blood post clotting completion) are used in the laboratory for glucose estimation. It is well recognized that the plasma has higher water content, and the molar concentration of glucose in the plasma is ∼11% higher than in the whole blood (provided the haematocrit and water concentration are normal). 7 Plasma is the recommended reference specimen type. 7 To compensate for the difference, a factor of 1.11 is recommended for meters to convert the concentration of glucose in whole blood to the equivalent plasma concentration when specimens are collected from the same sampling site (e.g. venous blood). This conversion factor is not applicable to arterial or capillary blood specimens analysed on glucose meters. 7 Capillary blood is therefore recommended as a substitute for venous plasma. 7 However the use of serum is discouraged as the concentration of glucose decreases during the time it takes for its preparation and the lower water content.
There have been numerous studies on the performance of different glucose meters and the manufacturers have responded by improving the strips and the meters technology to ensure accuracy and precision are improved. The accuracy of blood glucose measurement can be clinically significantly altered by substances that interfere with blood glucose measurements such as maltose, galactose, Icodextrin (a maltose precursor commonly used as an osmotic agent found in peritoneal dialysates), Octagam or Intragam (immunoglobulin solutions containing high maltose concentrations). 8 These interfering substances can give a falsely elevated blood glucose result resulting in undetected hypoglycaemia. Previously, maltose interfered with the measurement of glucose on Roche strips but the newer strip in now stated not to have this problem. Another factor interfering with the accuracy of glucose measurement is haematocrit. One supplier, Nova Bio-medical produces a strip (Nova StatStrip #42214) reported to be unaffected by changes in haematocrit when used with the Nova Xpress meter (Nova Bio-medical, Waltham, MA USA). 9 Adjustment equations for abnormal haematocrit to the normal of 0.43 are available (0.84/(0.93–0.22) × measured haematocrit) but this relies on the haematocrit being available. 7
The performance expectations for glucose meters have been defined by a number of professional bodies without an agreement between these bodies. The ADA has set the most stringent analytical goal, stating that the difference between capillary and laboratory samples should be <5%. 10 The Clinical Laboratory Improvement Amendments of 1988 (CLIA 88) guidelines recommend that results should be within 10% or 0.3 mmol/L of target, whichever is larger. 1 The International Standards Organization (ISO) 15197 standard stipulates that <5% of results should fall outside the limits of <±20% or <±0.83 mol/L if the specimen result is <4.2 mmol/L from the reference specimen type, i.e. plasma value. 11
In this study we evaluated the performance of the newly released glucose strips from Roche and Abbott in both healthy and diabetic participants. The performance of the new strips was compared with the glucose result as measured on a general chemistry analyser (Beckman DxC800) utilizing various specimen types (capillary, venous lithium heparin whole blood, venous lithium heparin plasma and serum). The evaluation of the new strips was performed as close as possible to real-life situations as emphasized in the ISO 15197 standard. 11
Materials and methods
Measuring principles of the strips and comparative ‘reference’ method
The glucose meters tested were Roche AccuChek Performa with strip Cat No 05225469, Lot No 370029, and the Medisense Optium Xceed with strip Cat No 80114-35, Lot No 44451.
Literature insert information from both suppliers on the new strips
The imprecision of the meters was determined by using external quality assurance glucose meter specimens from the Royal College of Pathologist of Australasia (RCPA) Quality Assurance Program, rather than aqueous quality control material specimens provided by the two suppliers. The consecutive runs were performed with three levels, 10 times within 30 min. A patient specimen with a glucose concentration (∼1.4 mmol/L) was used to assess the imprecision performance at the very low concentration end. The between-run imprecision was assessed using two RCPA specimens analysed 20 times over eight days.
Patient sample comparative studies were conducted with specimens obtained by consent, and approved by the Princess Alexandra Hospital ethics committee. In total, 45 volunteers were recruited, consisting of healthy laboratory staff and diabetic hospital outpatients. The meters were checked using the two levels of control materials prior to any participant specimen testing, as part of the between-run imprecision protocol. The finger collection site of each participant was cleaned with an alcohol wipe, and allowed to thoroughly dry before piercing with a spring loaded sterile lancet. There was minimal squeezing or milking of the selected finger. The blood was applied directly onto the two strips (Roche and Abbott), one after the other for almost simultaneous analysis on each meter in random order. Three different laboratory staff were involved in the collection of the finger prick specimens, one with no previous experience with any blood glucose meters to ensure there was no bias in specimen collection. From each participant the following specimens were collected: a finger prick capillary, and from the antecubital vein a venous lithium heparin whole blood which was also used to provide the plasma, and a serum in Greiner Vacutainer Tubes (Greiner Bio-one, Kremsmünster, Austria). Participants were sampled individually and the venous specimens were collected by an experienced phlebotomist. The tubes were immediately gently inverted five to 10 times as recommended by Greiner. The capillary sample followed within a few minutes by the lithium heparin whole blood were analysed on the glucose meters. The venous lithium heparin whole-blood tube was then immediately centrifuged at 3000
Interference study
In total, 11 different potential interferents were tested based on previously reported effects on some glucose meters: galactose (Sigma #G0750), maltose (Sigma M5885), lactose (Sigma #L3625), Icodextrin (Baxter #AHB 5546, 7.4% w/v Extraneal Perioneal Dialysis Solution), Intragam (Intragam CSL Bioplasma #68632), paracetamol (Sigma #A73002), sodium chloride (Fisons #S/3160/63) and ascorbic acid (Sigma #255564). A pooled plasma specimen was spiked with increasing concentrations of each interferent. The ascorbic acid studies were performed with two different concentration ranges (study A 0.00–0.57 mmol/L, and study B 0.00–6.84 mmol/L). Ascorbic concentration in the plasma is <0.09 mmol/L with an adequate intake of vitamin C but it can be raised to >20 mmol/L in patients where high doses are administered. 12 To test the effect of sodium, a lithium heparin whole-blood specimen with low sodium was aliquoted into equal volumes. Then to each aliquot the same volume of aqueous stock sample containing increasing sodium concentration was added, providing a sodium range up to ∼170 mmol/L, while maintaining the same glucose concentration. The whole-blood samples were immediately analysed on the glucose meters then centrifuged and the plasma was measured on the Beckman DxC800 analyser for sodium and glucose.
To assess the effect of haematocrit, lithium heparin whole-blood specimens were centrifuged for two minutes, and then most of the buffy coat (white cell and platelets) and plasma was removed. The specimens were well mixed and divided into small volume aliquots to which increasing volumes of the aliquoted plasma were added to change the cell to plasma ratio haematocrit. The haematocrit was measured on a Sysmex XE-5000 (Sysmex, Norderstedt, Germany). The whole-blood specimens were immediately analysed on the two glucose meters. The aliquots were centrifuged and glucose was measured on the Beckman DxC800.
The effect of haemolysis was assessed by preparing increasing levels of haemolysis using lithium heparin whole-blood specimens subdivided into small volume aliquots and the aliquots were haemolysed using the shearing technique. 13 These glucose concentrations were measured on glucose meters, then the specimens were centrifuged and analysed on the Beckman DxC800 analysers for semi-quantitative levels of free haemoglobin in the plasma. A haemolysis index of one is equivalent to <50 mg/L of free haemoglobin.
Similarly, the effect of lipaemia was determined using lithium heparin whole-blood specimens and aliquoting it into small volume aliquots. A patient lithium heparin plasma specimen with very high triglycerides concentration was adjusted to contain the same glucose concentration as the lithium heparin whole-blood specimen for aliquoting. The whole-blood specimen was aliquoted in equal volumes and centrifuged for two minutes. An accurate and increasing volume of plasma was aspirated from each aliquot and replaced with the exact equal volume of plasma from the grossly lipaemic specimen so as to provide increasing triglyceride concentrations. The spiked aliquots were well mixed, analysed immediately on the two glucose meters, centrifuged and analysed on the Beckman analyser for glucose and triglyceride concentrations.
Finally, with the extreme range of temperatures experienced within Australia there is a potential for strips to be stored outside the recommended temperatures and still be used for specimen analysis. The effects of temperature on glucose analysis were assessed by storing the strips (3 strips at each temperature) at 4°C and 40°C and compared the results of the same lithium whole-blood specimen measured within 15 min to strips from the same pack stored at 21°C (room temperature). For the interference studies we used the CLIA 88 limit; expected results should be within 10% or 0.3 mmol/L of target (baselines), 1 if the difference was to be considered clinically not significant.
Statistical analysis was performed using the Microsoft Excel and Analyse-It statistical add-on for Microsoft Excel (Analyse-It, UK). The patient specimen comparisons were assessed by Passing Bablok Regression correlation equations for the different specimens and the Bland Altman difference plots 14 only for the finger prick capillary specimens versus lithium heparin plasma specimens.
Results
Imprecision
Imprecision studies data
The levels 2 and 3 used on the two different strips were different samples
RCPA, Royal College of Pathologist of Australasia; CV, coefficient of variation
Patient comparison
The specimens collected in lithium heparin were analysed with minimal time delay (<60 min). The degree of agreement between the two glucose meters and the different specimen types compared with the Beckman DxC800 glucose oxidase method is summarized in Table 3. In fact, 22% (10/45) of specimens with the Roche Accu-Chek Performa analyser and 16% (7/45) with the Abbott Optium Xceed analyser were outside the ISO 15197 standards for patient specimen comparison. The Roche strip showed slightly more finger prick capillary specimens with positive bias across the measuring range (Figure 1a) when compared with the Abbott strip (Figure 1b).
Bland-Altman difference plots of the finger prick capillary specimens measured on (a) Roche Accu-Chek Performa and (b) Abbott Optium Xceed meters versus lithium heparin plasma measured on Beckman DxC800 general chemistry analysers Patient comparison data with the different sample types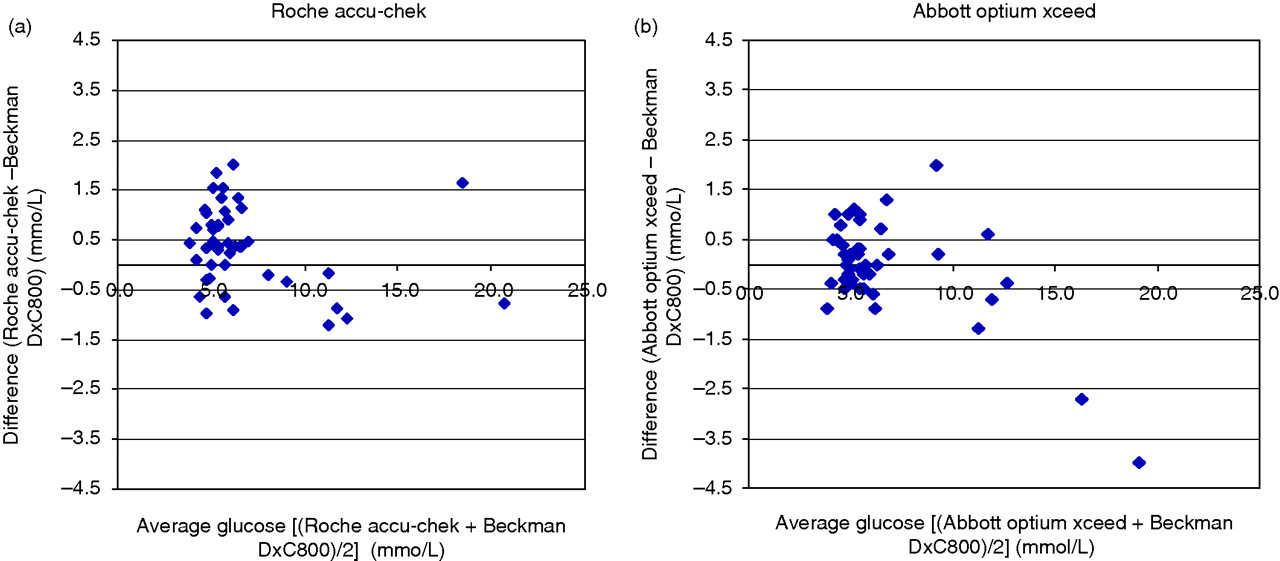
We performed linearity checks at both low (<2.0 mmol/L) and high glucose concentrations (>25 mmol/L) with pooled plasma either by diluting or by spiking it serially, and the results validate the stated limits by both suppliers (data not shown).
Interference studies
Results of interferents causing significant effect (bold)
E-1 – error message
*Ketones – values indicating should check for ketones
Discussion
This study assessed the performance of the newly released Roche and Abbott strips under conditions that reflect those encountered in routine clinical situations as stipulated by the ISO 15197. The imprecision of both strips are considered acceptable; hence, health-care providers and patients can use these strips with confidence to guide diabetic management.
The correlations between finger prick capillary and plasma glucose measurements indicate the difference between the glucose meters with the new strips and the laboratory analyser are still significant. In this study we found 78% and 84%, respectively, of the results with the Roche and Abbott strips not 95% or greater as recommended by the ISO guideline were within the recommended limits. 11 The more ambitious limit set out by the ADA, the difference between specimen pairs should be <5% 10 is unlikely to be met even with laboratory analysers for all specimens. However this goal should be supported to provide impetus for further improvement in the glucose strip technology. Although the imprecision studies using quality control materials achieved tight limits; whole-blood samples are complex matrices and this may explain some of the differences observed in the patient comparison studies. The differences are most clinically relevant at the low glucose concentration where a glucose below the critical limit ∼<2.5 mmol/L 16 may be reported as >2.7 mmol/L (based on observations in differences during our studies), falsely comforting the user that no immediate action need to be taken. Based on our findings on the performance of the strips, we would support the ADA's definition of hypoglycaemia and recommend hypoglycaemia treatment be initiated if the glucose result on a glucose meter is <3.9 mmol/L. 17
These data re-enforce the fact that these glucose meters, even with improved strips, are an aid in monitoring diabetes control but are not suitable for diagnostic and screening purposes. The difference is likely to be partially influenced by the differences in the specimen matrix, whole blood on glucose meters versus a cleaner plasma matrix used on general chemistry analysers. Clinicians should also be aware that analysis of glucose on specimens processed in the laboratory can be altered if the specimens are not collected, handled and processed properly and promptly. 18
The interference studies clearly demonstrate that maltose, from maltose itself, Icodextrin or immunoglobulin preparations, e.g. Intragam, do not interfere with the accuracy of the Roche strip. Galactose interference as stated by Roche and confirmed in this study is still capable of causing clinically significant interference in the measurement of glucose. Galactosaemia is a disease present at birth caused by a genetic lack of an enzyme needed to metabolize galactose into glucose. Galactosaemia is usually diagnosed by the newborn
Ascorbic acid affects both the Roche and the Abbott strips. The strips should therefore not be used in patients taking high dosages of vitamin C supplements and measurement of glucose in the laboratory needs to be performed on a system free from ascorbic interference.
Unlike the Nova strip, both the Abbott and the Roche strips continue to be affected by changes in haematocrit. Variations in haematocrit are far more common in hospitalized patients than in outpatients. When these glucose meters are used routinely by patients or care providers, the haematocrit is unknown. The interference mechanism is thought to be due to glucose redistribution between plasma and red cells with haematocrit changes. 8 For this exact reason, both Abbott and Roche indicate in their strip insert that the results can be affected in severely dehydrated patients (hyperglycaemia – diabetic ketoacidosis or hyperglycaemic hyperosmolar non-ketotic coma), severe hypotension, in shock or decompensated heart failure. Additionally the IFCC (International Federation of Clinical Chemistry) outlines that greater difference in glucose results may be observed with subgroups such as neonates or pregnant women, who may have slightly higher than average plasma water concentrations. 7 High sodium concentrations were confirmed to negatively decrease glucose results with the Roche strip, and this may be clinically relevant in the severely dehydrated patient.
We have confirmed that the strips tested in this study can be used with confidence in the presence of haemolysis up to 450 mg/dL, lipaemia with triglycerides concentration up to 27.4 mmol/L, paracetamol up to 500 mg/L and when stored at temperature ranging between 3°C and 40°C.
Although the new strips are currently only available on the Roche Accu-Chek Performa and Abbott MediSense Optium meters used in this study, they are likely to be rolled out in the near future on the remaining range of glucose meters.
Neither strip fulfills all the expectations desired of it. Due to the small analytical differences between the two strips, it is advisable when institutions or individuals are choosing a glucose meter that consideration be given to the data presented in this study. It is also advisable that patients utilize strips from the same company for the day to day assessment of blood glucose and not switch between different meters and strips.
Conclusion
This study highlights both Abbott and Roche still do not meet the ISO recommendation of <5% of the specimens from a finger prick results being <±20% or <±0.83 mol/L if the specimen result is <4.2 mmol/L compared with the reference specimen type, i.e. plasma. Maltose (tested up to 14.6 mmol/L) no longer interferes with the new Roche strip but it continues to have interference by galactose. Although only Roche state it on their package insert, ascorbic acid interferes with glucose estimation on both strips. Otherwise, analytically, small differences exist between the strips. When selecting glucose meters, end users should determine what is most suitable for their individual or group of patients needs, based on their own data and from the data provided in this report.
DECLARATIONS