
Abstract
Background
The aim of our study was to monitor radiofrequency catheter ablation-induced myocardial damage by measuring high-sensitivity cardiac troponin T (hs-cTnT).
Methods
Serum concentrations of hs-cTnT (Elecsys 2010 system, Roche) were measured in 73 healthy blood donors and serially in 27 patients who had samples taken both before and 24 h after radiofrequency ablation (RFA) for atrioventricular nodal re-entry tachycardia (AVNRT), atrial fibrillation (AF) or right atrial flutter (AFL).
Results
Significant increases of hs-cTnT were seen in patients after RFA (AVNRT: P = 0.0115, AF: P = 0.0011, AFL: P = 0.0009). Postprocedural serum hs-cTnT correlated with the number of radiofrequency applications and with the duration of RFA procedure. Spearman's coefficient of rank correlation (r) were as follows: hs-cTnT versus RFA duration: r = 0.771 (P < 0.001); hs-cTnT versus number of pulses: r = 0.708 (P < 0.001). Patients with the diagnosis of AVNRT had lower serum hs-cTnT concentration after RFA compared with AFL (P < 0.0001) and AF (P < 0.0001) patients.
Conclusions
Our data indicate that RFA causes a significant increase of serum hs-cTnT concentration that could be used to monitor myocardial injury.
Introduction
Radiofrequency catheter ablation (RFA) uses electrical energy to destroy tissues in the heart that are causing or perpetuating arrhythmias. It has become the treatment of choice for many types of cardiac rhythm disturbances. 1,2 It is used in recurrent atrial flutter, atrial fibrillation (AF), supraventricular tachycardia and some types of ventricular arrhythmia. RFA causes limited myocardial damage by thermal injury. When the temperature exceeds 50°C, cells become more depolarized, their transmembrane pump activity is impaired and the calcium buffering capacity is overwhelmed. RFA thus produces a small area of myocardial necrosis. 3 The thermal myocardial injury is accompanied by increases of some cardiac markers after RFA procedures. 4–6 Cardiac troponins are biomarkers of myocardial injury. According to a recent definition of myocardial infarction, 7 the cut-off value is defined as the 99th percentile of a healthy population concentration. This definition requires the use of tests with an imprecision coefficient of variation (CV) ≤10%. However, many methods used for cardiac troponin measurement do not meet this requirement. 8–10
To our knowledge, the present study is the first to measure cardiac troponin T (cTnT) concentrations using a high-sensitivity method in patients undergoing RFA. The aim of our study was to assess possible associations of cTnT serum concentrations measured by a new high-sensitivity (hs-cTnT) assay with RFA duration and the number of RFA lesions.
Materials and methods
cTnT was measured by high-sensitivity electrochemiluminiscence imunoassay using the TnT hs STAT assay for Elecsys 2010 analyzer (Roche Diagnostics, Mannheim, Germany). 11 The hs-cTnT assay had an analytical range of 0.003–10,000 μg/L. The cut-off value according to the manufacturer was 0.014 μg/L (i.e. the 99th percentile cut-off of healthy reference population values, n = 616, CV = 9.0%). Precision testing was performed using two quality control materials provided by the manufacturer (mean concentrations 0.0275 and 2.3600 μg/L), which were assayed 10 times during a 14-d period. Intra-assay precision was tested using a serum sample (mean concentration 0.0110 μg/L, n = 10).
Blood samples were obtained by venepuncture, immediately shipped to the laboratory and centrifuged (2500
Concentrations of cardiac troponins were determined in healthy blood donors and in patients undergoing radiofrequency catheter ablation. The study protocol was approved by the Ethical Committee of the Hradec Kralove University Hospital. Written informed consent was obtained from each patient or donor.
The cut-off values were determined as the 99th percentile of analysed serum concentrations from the control group of 73 blood donors without cardiovascular diseases (median age 56 ± 13 y, 48 men and 25 women).
A total of 27 patients (median age 54.8 ± 13.3 y, 14 men and 13 women) were treated by RFA for symptomatic atrioventricular nodal re-entry tachycardia (AVNRT, n = 11), right atrial flutter (AFL, n = 8) or AF (n = 8). hs-cTnT was analysed before and 24 h after the procedure (Table 1).
Duration of radiofrequency ablation (RFA) and the number of radiofrequency pulses in the treatment of different conduction disturbances
AVNRT, atrioventricular nodal re-entry tachycardia, AFL, right atrial flutter; AF, atrial fibrillation
Statistical analysis of data was performed using the MedCalc software (MedCalc Software, Mariakerke, Belgium). Results of serum hs-cTnT concentrations in blood donors and patients undergoing RFA are presented as the median and interquartile range. Statistical comparisons were performed using unpaired Wilcoxon test for the comparison of blood donors with patients before RFA and paired Wilcoxon test for pre- and postprocedure data. Concentrations of hs-cTnT measured after different RFA procedures in patients with AVNRT, AFL or AF diagnosis were compared using unpaired T-test (these data had normal distribution). A P value <0.05 was considered statistically significant. The relationship between hs-cTnT concentration and RFA duration or number of RF pulses was studied using Spearman's rank correlation analysis.
Results
Inter-assay CVs were in the range 2.0–3.8% for the manufacturer's material and the intra-assay CV was 9.6% for the serum sample. The 99th percentile of serum concentrations in our control group of 73 blood donors was 0.017 μg/L. Serum hs-cTnT concentrations in 43 (59%) healthy blood donors were below the limit of detection (0.003 μg/L).
Significant differences were detected in serum hs-cTnT concentrations between samples taken before and after RFA in the patient groups (Table 2). During baseline measurement in patients before RFA, hs-cTnT was increased above the cut-off value (0.014 μg/L) in five (19%) patients. There was a significant increase 24 h after RFA in the concentrations of hs-cTnT in 25 patients (93%). All patients had lower hs-cTnT before RFA than after the procedure. Patients with AVNRT diagnosis had lower serum troponin concentrations after RFA than did AFL or AF patients: AVNRT versus AFL (0.0570 versus 0.4465, P < 0.0001) and AVNRT versus AF (0.0570 versus 0.7130, P < 0.0001).
Serum hs-cTnT concentrations (μg/L) in blood donors and in patients before and after radiofrequency ablation (RFA)
AVNRT, atrioventricular nodal re-entry tachycardia; AFL, right atrial flutter; AF, atrial fibrillation; hs-cTnT, high-sensitivity cardiac troponin T
Postprocedural serum concentrations of hs-cTnT significantly correlated both with the number of radiofrequency pulses and with the RFA duration. Spearman's coefficients of rank correlation (r) were as follows: hs-cTnT versus RFA duration: r = 0.771 (P < 0.001) and hs-cTnT versus number of pulses: r = 0.708 (P < 0.001) (Figures 1 and 2).
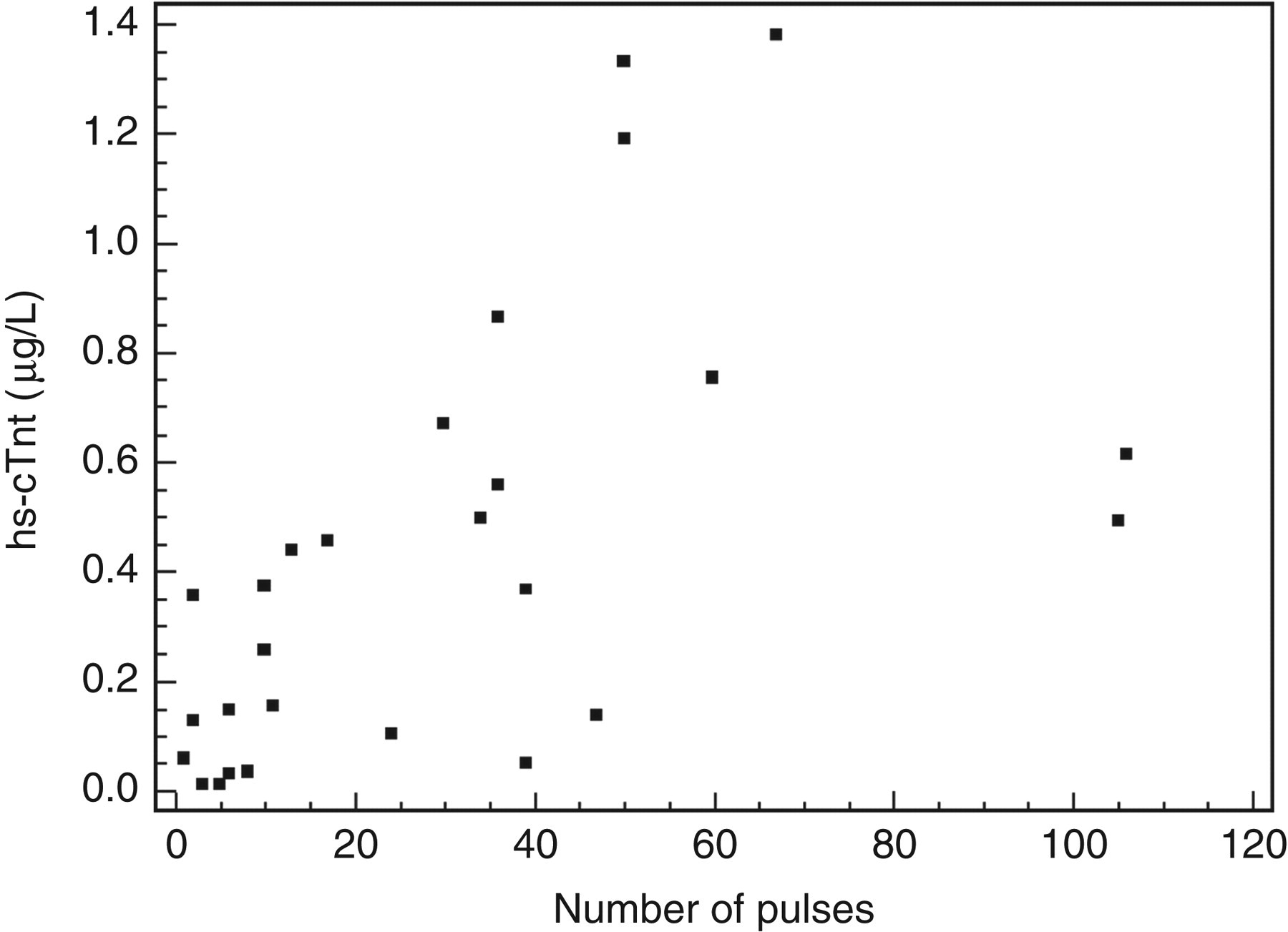
Relationship between postprocedural serum concentrations of hs-cTnT and the number of radiofrequency pulses. hs-cTnT, high-sensitivity cardiac troponin T
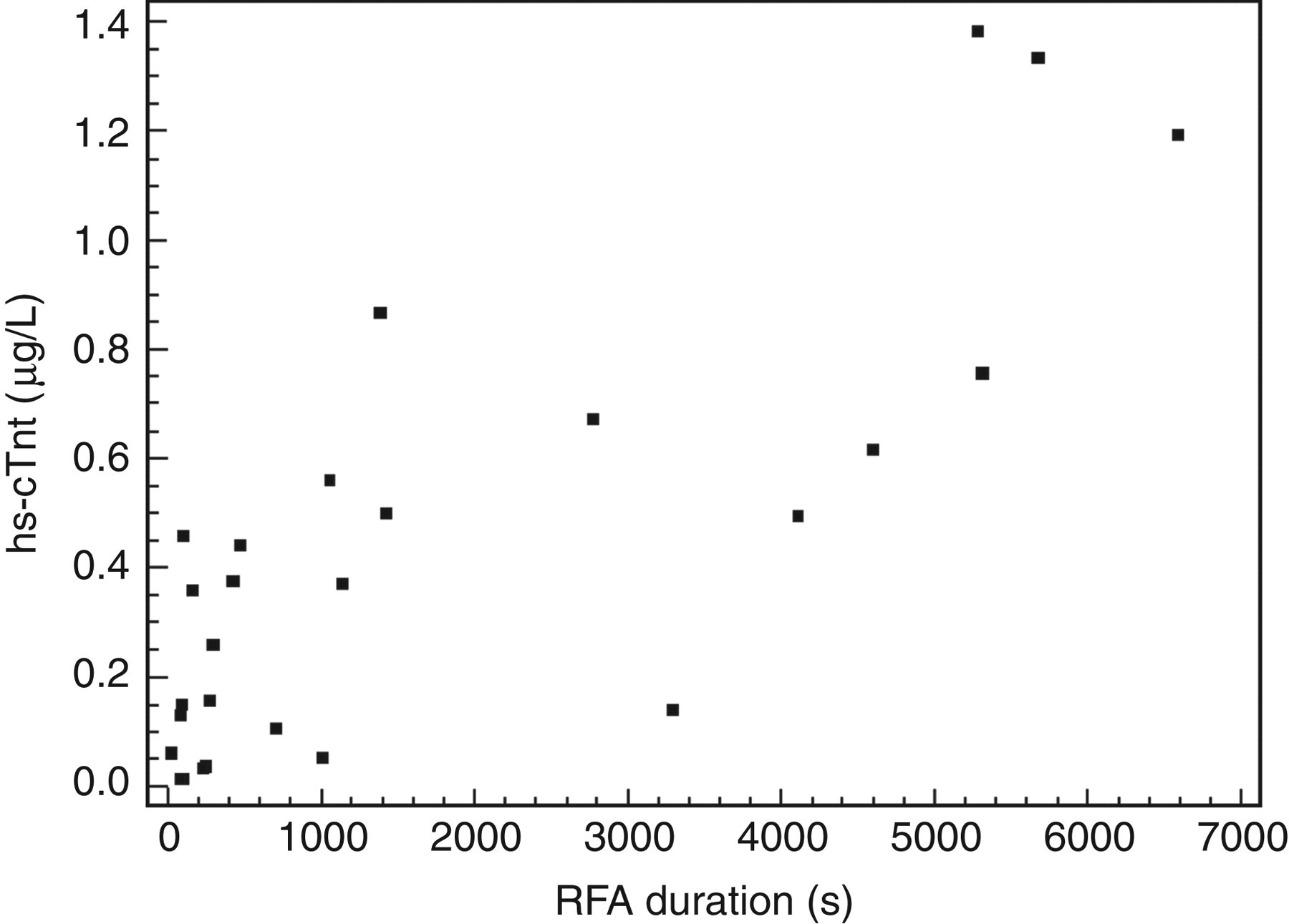
Relationship between postprocedural serum concentrations of hs-cTnT and the RFA duration. hs-cTnT, high-sensitivity cardiac troponin T; RFA, radiofrequency ablation
Discussion
Recent data highlight the important role of new markers in the diagnosis of ischaemic myocardial injury. 12–14 We present the first study to measure cTnT concentrations using a highly sensitive analytical method in patients undergoing radiofrequency catheter ablation treatment for supraventricular arrhythmias.
Our study demonstrates that hs-cTnT is increased in patients undergoing radiofrequency catheter ablation for supraventricular arrhythmias 24 h after the procedure. In the group of patients undergoing RFA, five patients had preprocedural elevation of hs-cTnT, while 25 had postprocedural elevation of hs-cTnT. The serum concentrations of hs-cTnT after RFA were 25.0 ± 23.5-fold higher than the cut-off value. These findings are in agreement with previous studies, 3,4 which quantified myocardial damage induced by RF ablation using creatine kinase MB isoenzyme (CK-MB) and cardiac troponins.
Correlations between cTnI or CK-MB levels and procedure-related variables (number of RF applications and the total duration of RF current) have recently been reported, 13–16 and are also confirmed by our study. We found a significant correlation of postprocedural hs-cTnT concentration with the number of RF applications and duration of RFA procedure.
Our study was a pilot non-randomized study with relatively small number of patients with heterogeneous types of arrhythmias. Nevertheless, our results show that first,even a minor degree of myocardial injury caused by radiofrequency catheter ablation is associated with a significant increase of hs-cTnT concentration and this increase persists for at least 24 h after the procedure, and second serum hs-cTnT concentration is associated with the number of lesions and with the duration of the RF current.
In conclusion, the hs-cTnT assay may be a useful method for monitoring myocardial injury after an RFA procedure.
DECLARATIONS