
Abstract
Background
Connective tissue growth factor (CTGF) may be a potential marker of fibrosis. However, platelet-derived CTGF may be released into the plasma by platelet activation during or after blood collection, thereby interfering with accurate determination of the true plasma CTGF level. Plasma CTGF exists as the N-terminal CTGF fragment (N-fragment), composed of modules 1 and 2, whereas platelet CTGF exists as full-length CTGF (full-length), composed of modules 1–4. We perceived the need to develop a method for distinguishing between the N-fragment and full-length CTGF levels, so that the true plasma and serum CTGF (N-fragment) levels could be accurately determined.
Methods
Full-length levels were determined by a sandwich enzyme-linked immunosorbent assay (ELISA) using two monoclonal antibodies recognizing modules 1 and 4, respectively (M1/4 ELISA). Total CTGF (full-length CTGF plus N-terminal CTGF) levels were determined by a sandwich ELISA using two monoclonal antibodies recognizing modules 1 and 2, respectively (M1/2 ELISA). N-terminal CTGF levels were determined by subtracting the full-length levels from the total CTGF levels.
Results
Both the M1/2 and M1/4 ELISAs showed good analytical performance. When the CTGF levels of plasma and serum collected simultaneously from the same subject were compared, the N-fragment levels determined by the subtraction method were the same, in spite of the fact that full-length CTGF was present in the sample.
Conclusion
N-fragment levels in plasma and serum can be accurately determined by this subtraction method, even if full-length CTGF in platelets is released during or after blood collection.
Introduction
Connective tissue growth factor (CTGF/CCN2), a member of the CCN family, is known as a multifunctional growth factor that plays important roles in extracellular matrix production, cartilage regeneration, angiogenesis, cell adhesion, migration and proliferation. 1–3 The CTGF level in blood is considered to reflect fibrosis in a variety of organs, because CTGF expression, induced by transforming growth factor beta (TGF-β) in inflammatory lesions, causes fibrogenesis in tissues, with production of extracellular matrix. 4–8 CTGF is also known to be present in platelets at a very high level, and it is released into the blood plasma as a result of platelet activation. 9,10 Therefore, accurate determination of the CTGF level in blood plasma requires either complete inhibition of CTGF release from platelets or specific measurement of the true CTGF level in plasma by excluding platelet-derived CTGF. Complete inhibition of platelet activation requires strict, careful performance of blood collection so as not to damage the vascular wall. 11–13 Subsequent handling of the collected blood samples must also be very strict and careful. For example, collected blood must be transferred gently and immediately into ice-cooled blood tubes containing special antiplatelet reagents, followed by immediate separation of the plasma to prevent CTGF release from platelets. 5,9
CTGF in platelets is known to be a full-length molecule consisting of four conserved domains, i.e. insulin-like growth factor-binding protein domain (module 1), von Willebrand factor type C domain (module 2), thrombospondin type I repeat domain (module 3) and C-terminal cysteine-knot I repeat domain (module 4), whereas CTGF in plasma is an N-terminal fragment consisting of modules 1 and 2. 5,9,10 We first developed two sandwich enzyme-linked immunosorbent assays (ELISAs): an M1/2 ELISA and an M1/4 ELISA. The M1/2 ELISA measures the total CTGF level, including both the N-terminal CTGF fragment and full-length CTGF, using anti-CTGF module 1 and anti-CTGF module 2 monoclonal antibodies. The M1/4 ELISA measures only the full-length CTGF level by using anti-CTGF module 1 and anti-CTGF module 4 monoclonal antibodies. The plasma N-terminal CTGF level is then determined by subtracting the full-length CTGF level from the total CTGF level.
In the present study, we examined the analytical performance of that ELISA system to determine whether both plasma, and serum including a large amount of full-length CTGF, can be used as the clinical sample. We also examined the stability of the plasma N-terminal CTGF level after plasma separation to determine the utility of the ELISA system. Finally, we examined whether there was any gender-based difference in the N-terminal CTGF level and analysed for a correlation between the N-terminal CTGF level and age using plasma from healthy volunteers.
Methods
Study subjects and blood collection
Eighty-five healthy volunteers (55 men and 30 women, aged 24–60 y) were recruited from among the workers of Sekisui Medical Co Ltd. The subjects fasted overnight, and then venous blood samples were drawn into four kinds of vacuum blood collection tubes (Terumo Corporation, Tokyo, Japan) for plasma (EDTA-2Na, heparin-Na and citrate-Na) and serum. The blood samples for plasma were separated by centrifugation at 3000 rpm (2080
Written informed consent was obtained from all of the volunteers at entry, in accordance with Sekisui Medical's code of ethics.
Materials
Ninety-six-well plates for ELISA were purchased from Thermo Fisher Scientific Inc. (Waltham, MA, USA). Anti-CTGF monoclonal antibodies were prepared by cDNA immunization according to the method of Tang et al. 14 which yielded antibodies recognizing the native conformation of CTGF, as described previously. 15 Briefly, plasmid DNA containing human full-length CTGF was injected intradermally to Balb/c mice using a gene gun. After three immunizations at biweekly intervals, the mice were sacrificed to establish hybridoma cell lines which produced anti-CTGF monoclonal antibodies (1–30D2, recognizing module 1 of CTGF; 2–13, recognizing module 2 of CTGF; 4–42, recognizing module 4 of CTGF) according to the method of Kohler and Milstein. 16 The 2–13 and 4–42 monoclonal antibodies were biotinylated using EZ-Link Sulfo-NHS-LC-Biotin (Thermo Fisher Scientific Inc, Waltham, MA, USA) and then used for ELISA. HRP-streptavidin was purchased from Thermo Fisher Scientific Inc. (Waltham, MA, USA). Recombinant CTGF proteins of N-fragment (modules 1 and 2), C-fragment (modules 3 and 4) and full-length, used for specificity tests of the ELISA, were produced using mammalian CHO cell lines transfected with a mammalian cell expression vector encoding the cDNA of each fragment or full-length CTGF. A FLAG epitope sequence was fused to the N-terminus of each of constructs. The proteins were purified using anti-FLAG agarose beads (Sigma-Aldrich, St. Louis, MO, USA). The recombinant protein of full-length CTGF was also used as the standard for the ELISA. The protein concentration of the standard was determined by the BCA method (Thermo Scientific), using bovine serum albumin (BSA) as the standard. The concentration of CTGF was expressed as picomoles per litre by dividing the protein concentration by its molecular weight, 38,000. Phosphate-buffered saline (PBS) containing 0.15 mol/L NaCl, pH 7.2, was used to dilute the monoclonal antibodies. PBS with 0.05% Tween 20 (PBST) was used as the wash buffer for each step. PBST with 1% BSA (BSA-PBST) was used as the blocking buffer and dilution buffer for diluting biotin-labelled antibodies and HRP-streptavidin. BSA-PBST containing HBR (Scantibodies Laboratory Inc, San Diego, CA, USA) and Heteroblock (Omega Biologicals Inc, Bozeman, MT, USA) was used as the dilution buffer for the calibrator and the plasma and serum samples. Citrate buffer (pH 5.0) containing o-phenylenediamine and H2O2 was used as the substrate solution for the HRP reaction.
CTGF assay
Full-length CTGF levels were determined by a sandwich ELISA using antimodule 1 and anti-module 4 antibodies as, respectively, the capture antibody and the labelled antibody (M1/4 ELISA). Total CTGF levels were determined by a sandwich ELISA using anti-module 1 and anti-module 2 antibodies as, respectively, the capture antibody and the labelled antibody (M1/2 ELISA). N-terminal CTGF levels were calculated by subtracting the full-length levels from the total CTGF levels (Figure 1). Each sandwich ELISA was performed as follows. Anti-CTGF module 1 antibodies (50 μL/well), diluted to 5 μg/mL with PBS, were added to a 96-well ELISA plate, followed by incubation at 4°C overnight. The wells were washed three times with 400 μL of PBST, 100 μL of BSA-PBST (blocking buffer) was added and the plate was incubated for one hour at room temperature. After discarding the blocking buffer, 50 μL of the recombinant full-length CTGF solution as the standard or 50 μL of sample solution diluted with the dilution buffer (BSA-PBST containing HBR and Heteroblock) was added to each well, followed by incubation for one hour at room temperature. Plasma and serum samples were diluted 11- and 31-fold, respectively. After washing the wells three times with PBST, 50 μL of biotin-labelled anti-CTGF module 2 antibody (2–13) for the M1/2 ELISA or biotin-labelled anti-CTGF module 4 antibody (4–42) for the M1/4 ELISA, diluted to 1 μg/mL with BSA-PBST, was added to each well, followed by incubation for one hour at room temperature. After washing the wells, 50 μL/well of HRP-streptavidin, diluted to 1 μg/mL with BSA-PBST, was added to each well, followed by incubation for 30 min at room temperature. The wells were washed again, and then 50 μL of substrate solution containing o-phenylenediamine and H2O2 was added to each well, followed by incubation for exactly 10 min at room temperature. Then, 1.5 N sulphuric acid was added to each well to stop the enzymatic reaction of HRP. The amount of total or full-length CTGF in each well was determined by measurement of the absorbance at 492 nm.
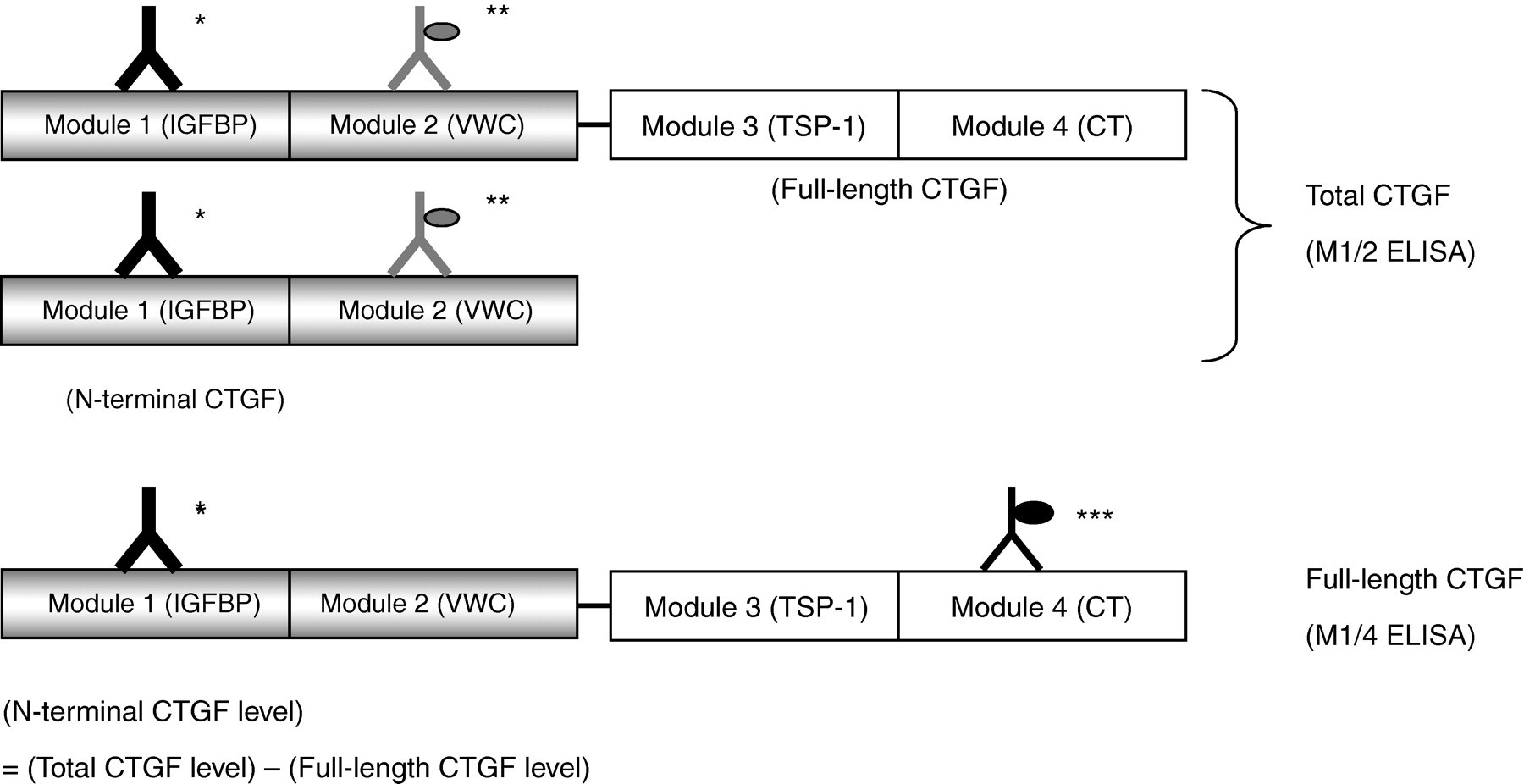
Subtraction method for determining N-terminal CTGF levels in blood plasma/serum. N-terminal CTGF levels were determined by subtracting the level of full-length CTGF from the level of total CTGF (including both full-length CTGF and N-terminal CTGF). The total CTGF level was measured by a sandwich ELISA using anti-CTGF module 1 and anti-CTGF module 2 monoclonal antibodies (M1/2 ELISA). The full-length CTGF level was measured by a sandwich ELISA using anti-CTGF module 1 and anti-CTGF module 4 monoclonal antibodies (M1/4 ELISA). CTGF, connective tissue growth factor; IGFBP, insulin-like growth factor binding protein; VWC, von Willebrand factor type C; TSP-1, thrombospondin type 1 repeat; CT, carboxy-terminal cysteine knot. *Anti-CTGF module 1 monoclonal antibody (1–30D2); ELISA, enzyme-linked immunosorbent assay. **Biotin-labelled anti-CTGF module 2 monoclonal antibody (2–13). ***Biotin-labelled anti-CTGF module 4 monoclonal antibody (4–42)
Statistics
Statistical analyses were performed using Stat Flex for Windows ver. 5.0 (Artech Inc, Osaka, Japan). All values were expressed as the mean ± standard deviation (SD). Differences between groups were assessed using Student's paired t-test. Relationships between parameters were examined using Pearson's correlation coefficient. For all analyses, P < 0.05 was considered statistically significant.
Results
Analytical performance of ELISA
The reactivity for each recombinant protein, i.e. N-fragment (modules 1 and 2), C-fragment (modules 3 and 4) and full-length CTGF (modules 1–4), in the M1/2 ELISA and the M1/4 ELISA was investigated to confirm the specificity of each ELISA. The M1/2 ELISA showed reactivity for the N-fragment and the full-length CTGF. The M1/4 ELISA showed reactivity for only the full-length CTGF. Neither ELISA showed reactivity for the C-fragment (Figure 2). The measurement range was 7.81–500 pmol/L in both ELISAs. The dilution linearity tests of the M1/2 and M1/4 ELISAs showed that the curve produced by serially diluted plasma or serum samples was parallel to the original standard curve (Figure 3). Plasma and serum samples with different concentrations of CTGF were measured 16 consecutive times in the assays. The coefficient of variation was 5.5–6.1% for the M1/2 ELISA and 2.9–4.3% for the M1/4 ELISA.
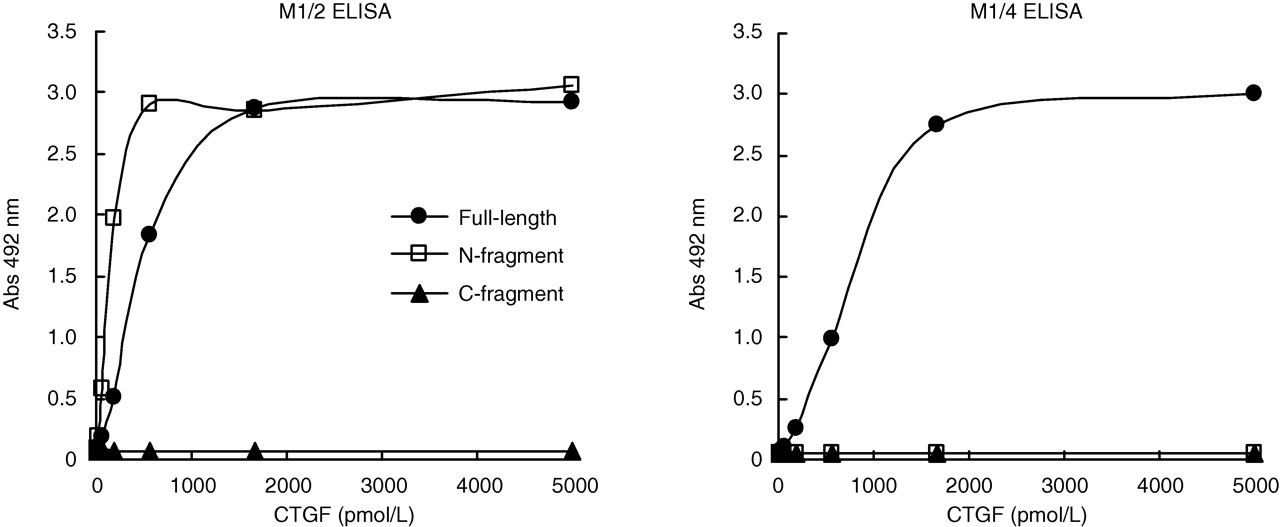
Reactivity of M1/2 and M1/4 ELISAs for the recombinant CTGF proteins of the full-length (modules 1–4), N-fragment (modules 1 and 2) and C-fragment (modules 3 and 4). Each point represents the average of duplicate values, which differed by less than 5%. CTGF, connective tissue growth factor; ELISA, enzyme-linked immunosorbent assay
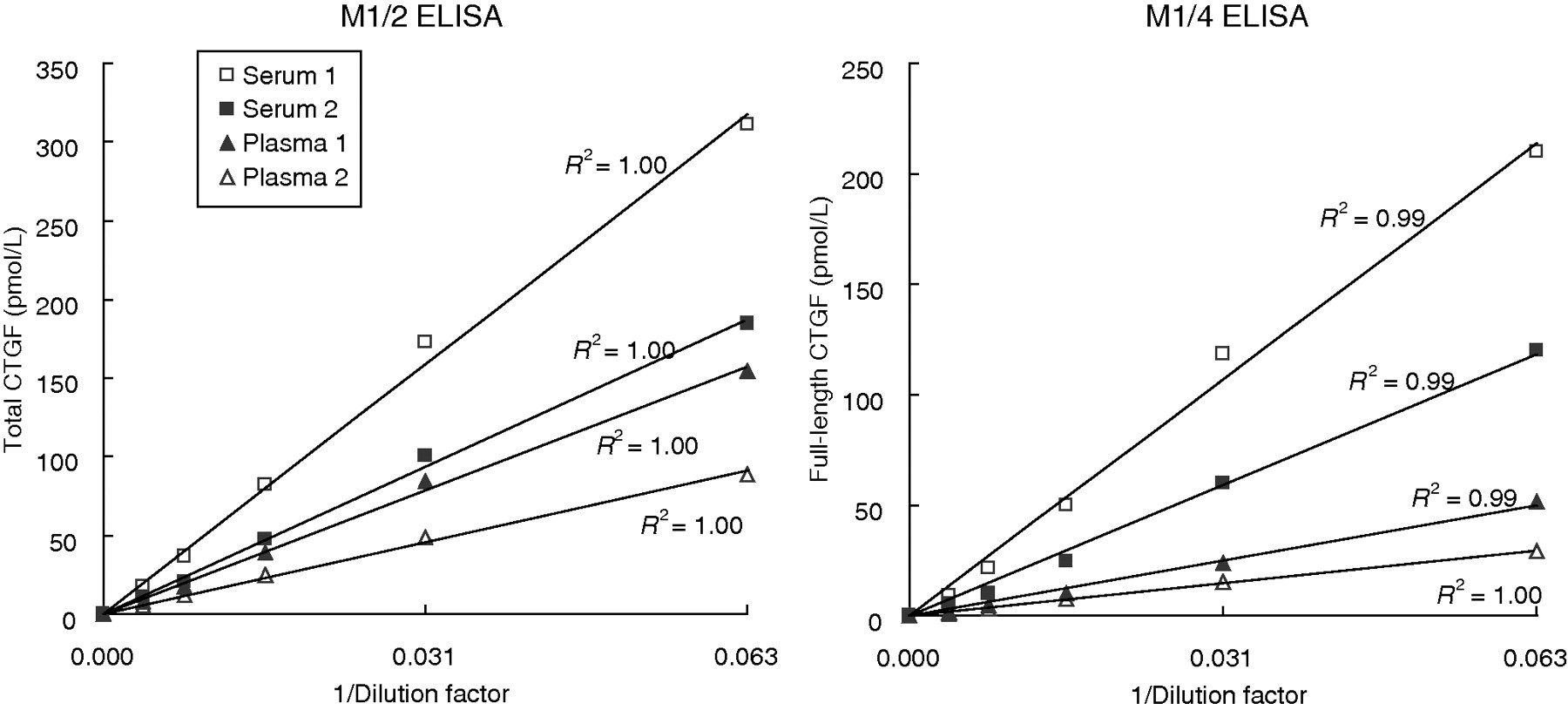
Dilution linearity of CTGF levels of plasma and serum samples in the M1/2 and M1/4 ELISAs. Plasma and serum samples obtained from two randomly selected subjects were first diluted 16-fold, and then diluted stepwise, four times, using a factor of 2. Those five dilutions were subjected to each assay. The measured CTGF levels were plotted. Each point represents the average of duplicate values, which differed by less than 5%. CTGF, connective tissue growth factor; ELISA, enzyme-linked immunosorbent assay
Comparison of CTGF levels in plasma and serum samples
CTGF levels were compared between the plasma and serum samples. Blood was drawn and immediately incubated for one hour in ice water for plasma, or at room temperature for plasma and serum before centrifugation. The total, full-length and N-terminal CTGF levels in the plasma and serum were determined after centrifugation. The total CTGF level measured by the M1/2 ELISA was a little higher in the plasma incubated at room temperature before centrifugation and markedly higher in the serum than in the plasma incubated in ice water (Figure 4a). Full-length CTGF measured by the M1/4 ELISA was hardly detected in the plasma in ice water, but clearly detected at levels of 141–376 pmol/L in the plasma incubated at room temperature before centrifugation and at levels of 2138–3502 pmol/L in the serum (Figure 4b). On the other hand, the N-terminal CTGF levels determined by the subtraction method were the same in the plasma and serum samples (Figure 4c).
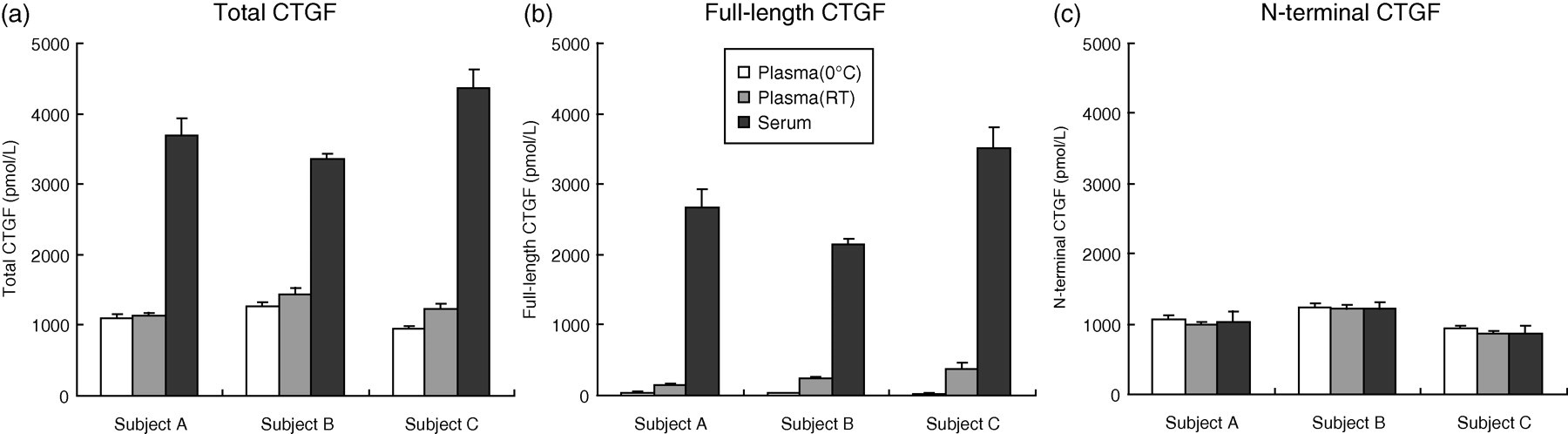
Comparison of CTGF levels among plasma and serum samples. Blood samples obtained from three volunteers (subjects A–C) were incubated for one hour in ice water for plasma or at room temperature for plasma and serum before centrifugation. The total, full-length and N-terminal CTGF levels in the samples were determined by the M1/2 ELISA, the M1/4 ELISA and the subtraction method, respectively. Values are presented as the mean value ± SD of quadruple determinations. CTGF, connective tissue growth factor; ELISA, enzyme-linked immunosorbent assay; SD, standard deviation
Stability of CTGF in blood plasma and effect of anticoagulants
The stability of CTGF in centrifuged plasma was investigated. First, the effect of freezing and thawing was examined. Plasma samples obtained from four volunteers were subjected to one or two cycles of freezing at −80°C and thawing. The N-terminal CTGF levels in the samples were determined by the subtraction method. The levels were not changed by up to two cycles of freezing and thawing (Figure 5a). Second, the effects of the storage temperature and duration were examined. Plasma samples obtained from four volunteers were incubated at 4°C or 25°C for a maximum of 24 h. Samples were then taken at intervals during the incubation, and the N-terminal CTGF levels were determined by the subtraction method at each sampling time point. The levels were found to be stable for at least 24 h at both 4°C and 25°C (Figure 5b). Third, the CTGF levels were compared among EDTA-, heparin- and citrate-plasma to examine the effects of the anticoagulants. Blood was drawn into three kinds of tubes containing EDTA-2Na, heparin-Na or citrate-Na and immediately separated by centrifugation. The N-terminal CTGF levels in the plasma were determined by the subtraction method. The N-terminal CTGF level did not differ between EDTA- and citrate-plasma, but it was significantly higher in the heparin-plasma than in the EDTA- and citrate-plasma (Figure 5c).
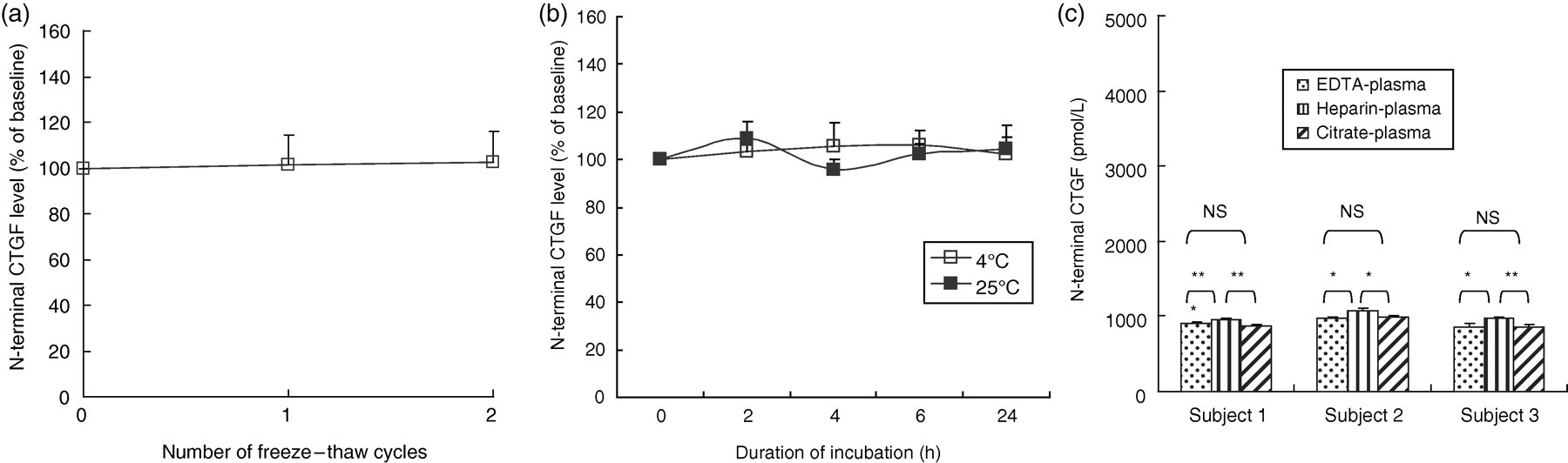
CTGF stability in blood plasma and effect of anticoagulant. (a) Effect of freezing and thawing. The plasma was subjected to one or two cycles of freezing at −80°C and thawing. The N-terminal CTGF levels in the samples were determined by the subtraction method. Each value is presented as a percent of the baseline level. Values are presented as the mean value ± SD for the four subjects. (b) Effects of storage temperature and duration. The plasma was incubated at 4°C or 25°C for a maximum of 24 h. The N-terminal CTGF levels in samples taken at intervals were determined by the subtraction method. Each value is presented as a percent of the baseline level. Values are presented as the mean value ± SD for the four subjects. (c) Effect of anticoagulants. Blood samples from three volunteers (subjects 1–3) were drawn into three kinds of vacuum blood collection tubes containing either EDTA, heparin or citrate. The N-terminal CTGF levels in the plasma samples were determined by the subtraction method after centrifugation. Values are presented as the mean value ± SD of triplicate determinations. The asterisk denotes a significant difference (**P < 0.01, *P < 0.05). NS: no significant difference; CTGF, connective tissue growth factor; SD, standard deviation
Effects of gender and age on plasma N-terminal CTGF levels in healthy subjects
The N-terminal CTGF levels in the plasma were determined for blood samples obtained from all 85 volunteers. The mean value ± SD was 1177 ± 233 in the total subjects. The maximum and minimum values were 1750 and 776 pmol/L, respectively. We compared the N-terminal CTGF levels between the men and women, but no significant difference was found between them (1185 ± 223 versus 1162 ± 254 pmol/L, P = 0.667).
We then examined for correlation between the N-terminal CTGF level and age. No significant correlation was found in the male subjects aged 24–60 y or in the female subjects aged 25–42 y (Figure 6).
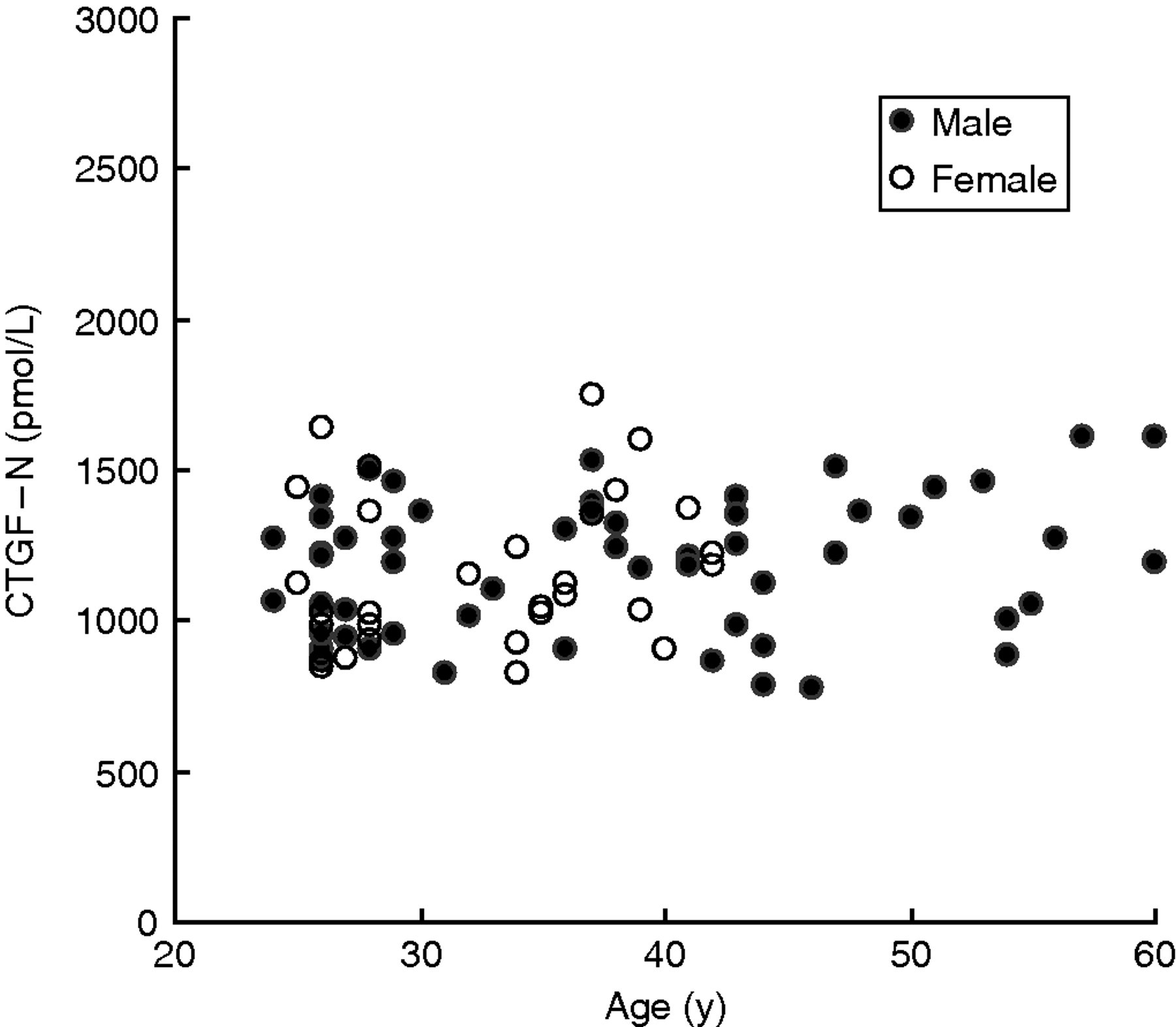
Correlation between the plasma N-terminal CTGF level and subject age. In the total subjects (n = 85), r = 0.198, P = 0.069; in men (n = 55), r = 0.204, P = 0.135; In women (n = 30), r = 0.201, P = 0.288. CTGF, connective tissue growth factor
Discussion
CTGF is considered a potential diagnostic marker reflecting fibrosis in a variety of organs because CTGF expression, induced by TGF-β in inflammatory lesions, leads to extracellular matrix production and fibrogenesis in tissues. 4–8 Several methods for measuring CTGF levels in blood have been reported. 5,17–19 However, some did not distinguish between N-terminal CTGF circulating in blood and platelet-derived full-length CTGF. Others did not sufficiently examine the accuracy of the N-terminal CTGF level calculated from the difference between the total CTGF and the full-length CTGF levels, even though they were measured separately. In the present study, we first developed two ELISA systems, an M1/2 ELISA measuring the total CTGF level, including both the N-terminal CTGF and full-length CTGF levels, and an M1/4 ELISA measuring only the full-length CTGF level. Then, we determined the N-terminal CTGF level by subtracting the full-length level from the total level. This method enables accurate determination of the N-terminal CTGF level even if the sample also contains platelet-derived full-length CTGF.
Here, we investigated the analytical performance of the M1/2 and M1/4 ELISAs. Both ELISAs showed good performance in terms of specificity (Figure 2), dilution linearity (Figure 3) and reproducibility. We next compared the total CTGF, full-length CTGF and N-terminal CTGF levels between the plasma and serum samples obtained from the same individual volunteers. Full-length CTGF was detected at a high concentration in the serum (Figure 4b), whereas little was detected in plasma held in ice water before centrifugation. Cicha et al. 9 reported that a large amount of CTGF, which has a molecular weight of 38 kDa, was released from platelets upon their activation. Kubota et al. 10 reported that a large amount of CTGF was released from platelets into the serum as a result of blood coagulation. Those reports are comparable to our finding in the present study indicating that a considerable amount of CTGF was released upon platelet activation. Another finding of our present study is that a certain amount of full-length CTGF was released from platelets into the plasma during storage for one hour at room temperature before centrifugation, even when using an anticoagulant (Figure 4b). This suggests that chilling blood in ice water immediately after drawing blood is required to completely prevent CTGF release. We tested the use of blood collecting tubes containing heparin or citric acid instead of EDTA as the anticoagulant, but CTGF release from platelets was not completely prevented (data not shown,). Roestenberg et al. 5 reported that full-length CTGF was not detected in the plasma samples when blood was collected in tubes containing prostaglandin E1 and theophylline and immediately stored on ice in order to prevent platelet activation. However, a variety of precautions are required to completely prevent platelet activation, not only after blood collection but also during blood collection. 11–13 For example, careful venipuncture so as not to injure the vascular wall is required to prevent in vitro activation of platelets during blood collection. Therefore, it may be difficult to draw blood from patients with thin vessels or obese patients whose vessels are hard to find. In addition, we cannot distinguish whether platelets in each blood sample are activated or not, during or after blood collection, unless we measure the levels of platelet activation markers such as beta-thromboglobulin and platelet factor 4. 12,13
We showed that plasma N-terminal CTGF levels determined by the subtraction method, which we developed in the present study, were identical with the levels in the serum samples obtained from the same individual subjects (Figure 4c). This indicates that N-terminal CTGF levels in circulating blood can be accurately determined by this method, even in plasma or serum samples that contain full-length CTGF released from platelets during or after blood collection. We have preliminary results showing that the diagnostic accuracy was improved by the subtraction method for measurement of the plasma N-terminal CTGF level when several patients with hepatic fibrosis were used (data not shown.).
We then examined the stability of the N-terminal CTGF level in plasma, determined by the subtraction method. The level was not changed by up to two cycles of freezing and thawing (Figure 5a), and it remained constant for 24 h at 4°C or 25°C (Figure 5b). These findings suggest that plasma samples can be safely stored in a freezer until assay, or at 4°C or room temperature for at least 24 h after plasma separation. We tested the use of heparin and citrate instead of EDTA to examine for a possible effect of the anticoagulant. The N-terminal CTGF level was slightly but significantly higher in the heparin-plasma than in the EDTA- and citrate-plasma (Figure 5c). We repeated the experiment three times and the results were the same. It is not clear what causes the slight elevation in heparin-plasma, but heparin may affect the reactivity of the anti-CTGF antibody for the N-terminal CTGF. This finding suggests that heparin-plasma should not be used for this assay.
We next determined the plasma N-terminal CTGF levels of 85 volunteers by using this ELISA and subtraction method. We first compared the levels between men and women, and found no significant difference between them. Also, no significant correlation was found between the N-terminal CTGF level and age, at least in the male subjects (Figure 6). Two earlier studies reported the plasma N-terminal CTGF levels of healthy subjects. 5,20 The mean levels were 103 pmol/L (n = 21) in the study of Roestenberg et al. 5 and 25 ng/mL (n = 18), which converts to 1250 pmol/L when the molecular weight of N-terminal CTGF is 20 kDa, in the study of Dziadzio et al. 20 Our result for the plasma N-terminal CTGF level was similar to that of Dziadzio et al. 20
In summary, we demonstrated that platelet-derived full-length CTGF is released into the plasma depending on the holding conditions after blood collection. Moreover, using our newly established subtraction method, the N-terminal CTGF level in plasma can be accurately determined, even if the sample contains full-length CTGF released from platelets. Our results suggest that the subtraction method has great potential for use in elucidating the clinical significance of measuring plasma N-terminal CTGF levels in a variety of fibrotic disorders.
DECLARATIONS