
Abstract
The last few decades have seen a significant decrease in the rates of analytical errors in clinical laboratories. Evidence demonstrates that pre- and post-analytical steps of the total testing process (TTP) are more error-prone than the analytical phase. Most errors are identified in pre-pre-analytic and post-post-analytic steps outside of the laboratory. In a patient-centred approach to the delivery of health-care services, there is the need to investigate, in the TTP, any possible defect that may have a negative impact on the patient. In the interests of patients, any direct or indirect negative consequence related to a laboratory test must be considered, irrespective of which step is involved and whether the error depends on a laboratory professional (e.g. calibration/testing error) or non-laboratory operator (e.g. inappropriate test request, error in patient identification and/or blood collection). Patient misidentification and problems communicating results, which affect the delivery of diagnostic services, are recognized as the main goals for quality improvement. International initiatives aim at improving these aspects. Grading laboratory errors on the basis of their seriousness should help identify priorities for quality improvement and encourage a focus on corrective/preventive actions. It is important to consider not only the actual patient harm sustained but also the potential worst-case outcome if such an error were to reoccur. The most important lessons we have learned are that system theory also applies to laboratory testing and that errors and injuries can be prevented by redesigning systems that render it difficult for all health-care professionals to make mistakes.
Introduction
During the past decade, after the publication of the Institute of Medicine (IOM) report,
Errors in laboratory medicine: reasons for a neglect
Most of the many different terms used in the literature to define errors in laboratory medicine (e.g. mistakes, blunders, defects, outliers, unacceptable results and quality failure) have negative connotations of blame, individual failure and culpability and, even worse, pertain to studies focusing on a limited number of total testing process (TTP) steps. A key step toward initiatives aiming to reduce errors and improve patient safety in the discipline will be made once consensus has been achieved on a comprehensive definition of errors in the laboratory testing.
Errors in laboratory medicine are intrinsically obscure as they are difficult to identify and, when found, are less easily understood than other types of medical error. Compared with adverse events related to surgery or other treatment errors that are often glaring and obvious, laboratory errors tend to be more insidious and difficult to pinpoint in time and place. The difficulties depend largely on there being several steps involved. Firstly, there is a time lapse between laboratory testing, physicians' action and patient outcomes. Potential failures in the process steps nearest to patient intervention are, in fact, more likely to result in patient injury or harm. Failures that occur earlier on in the process are more likely to result in process disruption but ‘active and passive’ defensive barriers – which rely on technology, people, procedures and administrative controls – may mitigate their potential harm or may prevent the recognition of their effect on the final adverse event. Secondly, the testing process is complex, consists of numerous steps and stretches across multiple providers. Moreover, only the analytical phase falls under laboratory control, while the pre- and post-analytic phases pertain to different stakeholders other than the laboratory such as the clinician, the nurse, the patient and others involved in patient identification, data entry, specimen collection and transport. In the postanalytic phase there is the possibility of inappropriate response to the receipt, interpretation and utilization of laboratory information. 3 Carefully designed studies, a multidisciplinary approach and teamwork are therefore required for a thorough investigation of TTP. Thirdly, physicians responsible for making clinical decisions seldom perceive laboratory errors as a harmful source of patient adverse events, nor do they understand that most laboratory defects may arise from the pre- and post-analytic steps. Fourthly, laboratory professionals are reluctant to divulge data on the frequency and types of errors observed in their own setting for fear of a sense of blame, individual failure and culpability associated with these events. 4 This, in turn, makes it difficult to evaluate the entire testing process and set quality specifications for each step in order to identify weakness in policies and procedures to provide opportunities for quality improvement through the formulation and prioritization of corrective actions. Finally, laboratory testing is no longer performed only in the clinical laboratory setting: point-of-care testing, the fastest growing segment of current clinical laboratory testing market, near-patient testing and self-monitoring are widely used alternative or complementary testing options.
There is therefore an urgent need to evaluate errors in laboratory medicine within the reliable framework of the TTP. From the patient's viewpoint, the integrity of the entire process is important and there is a need to prevent any error in the pre-, intra- or post-analytic phase. From this perspective, any possible defect in TTP should be investigated in order to prevent and obviate any negative impact on patient care, irrespective of the step involved, and of whether the error has been caused by a laboratory professional (e.g. calibration or testing error) or by a non-laboratory operator (e.g. inappropriate test request, error in patient identification, blood collection and/or result interpretation). 5,6
Definition of error
The different terms used as synonyms in the literature on laboratory errors are the fruit of different study designs that have almost exclusively allowed the evaluation of analytical errors (e.g. outliers, unacceptable results) or, as in the case of the split-specimen design, are insensitive to many steps in the testing process, particularly those at the beginning and/or at the end of the cycle. One recent and interesting proposal made is to use a neutral term such as ‘quality failure’, which mitigates the negative connotations associated with previously reported terms, and the related fear of culpability and blame. According to the author, this term means ‘any failure to meet the required output quality necessary for optimum patient care anywhere in the pathway from test selection to the return of an appropriately interpreted report to requesting clinician’.
4
This definition has a clear focus on patient care and patient outcomes rather than on processes and procedures. However, the term ‘error’ is used in the medical literature, and should therefore be employed also for errors in laboratory medicine, particularly as they are part of the broader issue of diagnostic errors.
7
The Technical Specification released by the International Organization for Standardization (ISO/TS 22367) defines laboratory error as failure of planned action to be completed as intended, or use a wrong plan to achieve an aim, occurring at any part of the laboratory cycle, from ordering examinations to reporting results and appropriately interpreting and reacting to them.
8
Types of errors in laboratory medicine and their prevalence
Laboratory medicine, as a specialty that had prioritized quality control, has always been at the forefront of error reduction. In terms of quality control and error rates, laboratory medicine has a far better record than most other fields in health care. Some studies indicate that, in the analytic phase, the average error rate is as low as 0.002%; this is functioning at the five sigma level. As a comparison, the rates of infections and medication errors are closer to three sigma, that is defect rates >3000-fold those in the clinical laboratory (Figure 1).
2
(The concept of ‘sigma’, according to stringent statistical quality control criteria, means that a process is considered to be in control if the variation – expressed as standard deviation [sigma,
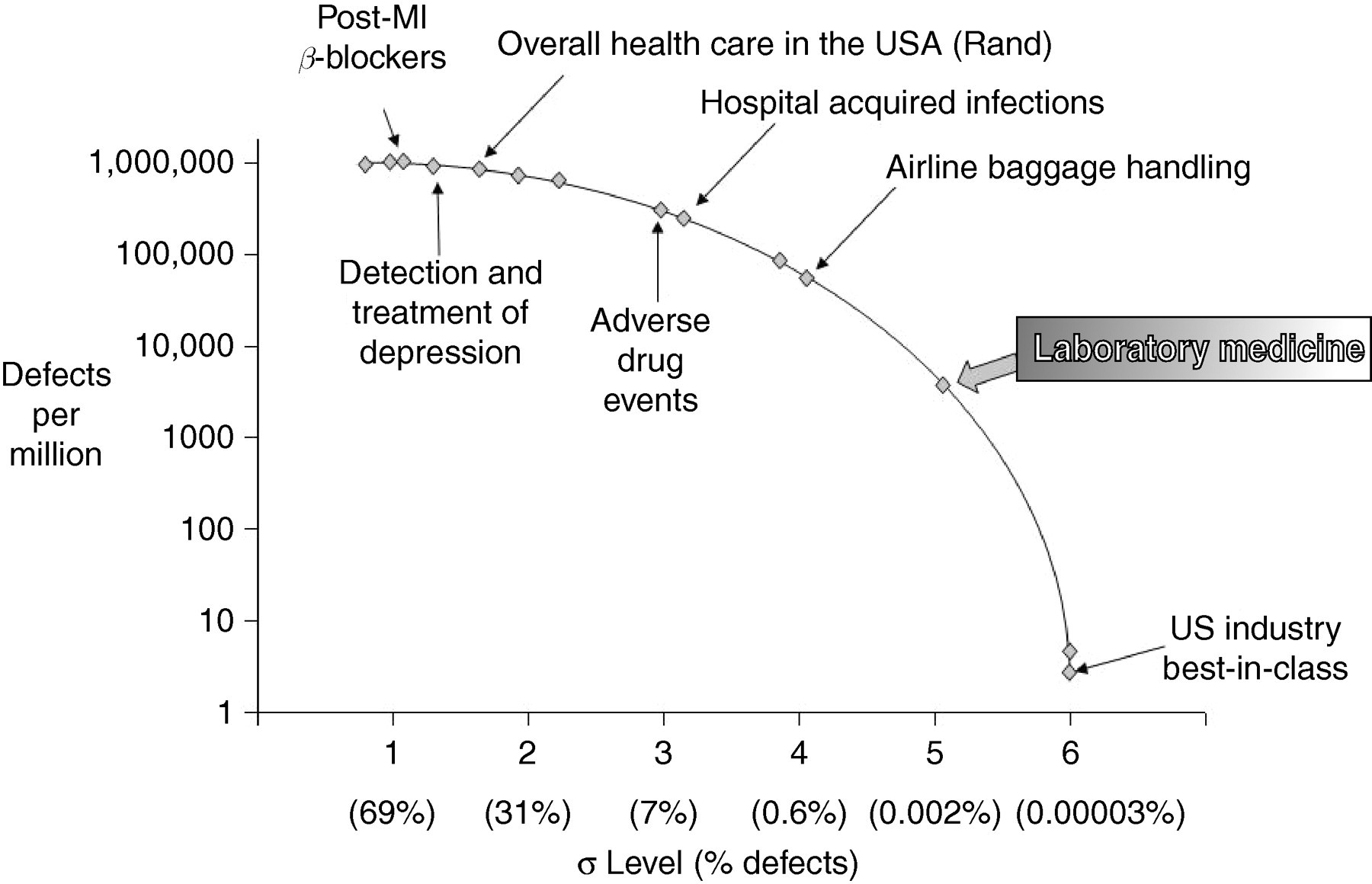
Defect rates in laboratory medicine as compared with other sectors (from reference, 2 modified)
However, the data are less impressive when one considers the entire testing process of selecting, requesting, identifying patients, collecting and transporting specimens, analysing, reporting, interpreting and utilizing laboratory results. As stated by Mark Graber 11 ‘errors related to laboratory testing are too common and constitute a significant fraction of diagnostic errors in medicine today’. Laboratory testing in modern clinical medicine is assuming an increasingly important position in the diagnostic process, and in monitoring the effects of therapy. Therefore, even a low incidence of laboratory testing errors among the billions of tests performed every day worldwide might have important health and patient safety implications. Data collected on laboratory error rates will depend critically on the study design and in particular the TTP steps investigated. It is therefore easy to understand why the error rates in the literature may vary from one identified error every 33–50 events to 1000 events, or from 214 to 8300 laboratory results. 12–16
Analytical errors
Early studies in the field of error in laboratory medicine were devoted to identifying analytical errors, the analytical phase being the ‘core’ of laboratory work and analytical processes under the control of the laboratory staff. An analysis of the data collected and reported in the literature, starting with the paper published by Belk and Sunderman in 1947 through the results collected by the College of American Pathologists in the 90s and, finally, the data published by Witte and co-workers in 1997 shows that error rates have decreased from 162,116 per million laboratory tests (part per million, ppm) to 447 ppm.
17–20
This dramatic and impressive reduction in errors, by about 300-fold, derives from automation, improved laboratory technology, assay standardization, well-defined rules for internal quality control, effective quality assurance schemes and better trained staff. However, recently collected data demonstrate that analytical quality is still a major issue. Westgard has demonstrated that estimates on a
As already stressed, there is no discrepancy between the impressive reduction in analytical errors achieved over the last few decades and current evidence that analytical quality is not satisfactory when evaluated on the sigma scale, the Six Sigma being one of the best available approaches for providing objective estimates and metrics in several industries. 11,26 Therefore, despite the impressive improvement achieved in analytical quality, a body of evidence demonstrates that further improvements are needed. This should be achieved by setting down and using evidence-based analytical quality specifications in every-day practice; if this were done, rules for internal quality control and external quality assessment procedures would be more appropriate. Moreover, there is an urgent need for standardization programmes aiming at improving metrological traceability and correcting biases and systematic errors. Finally, more stringent metrics, such as the Six Sigma, should be introduced into clinical laboratories to improve upon current analytical quality.
Pre- and post-analytical phases
While the frequency of laboratory errors varies greatly, depending on the study design and TTP steps investigated, a series of papers published between 1989 and 2007 drew the attention of laboratory professionals to the pre- and post-analytical phases, which currently appear to be more vulnerable to errors than the analytical phase. Our group published two papers, in 1997 and 2007, using one study design that allowed us to investigate most TTP steps in the same clinical context; it also used the same menu of tests (stat laboratory). 27,28 The results (Table 2) demonstrate a significant, although not dramatic, decrease in the error rates in 2007 but a similar distribution of errors. The pre-analytic phase had the highest error rate, the most frequent problems arising from mistakes in tube filling, inappropriate containers, and requesting procedures. Identification errors were noted for three patients and 14 related tests (875 ppm) in the 2007 study. There was a significant reduction in the proportion of specimens collected inappropriately from the infusion route in the later study. The main reasons for errors in the postanalytic phase were an excessive turnaround time in the later study, errors in keyboard entry and missed correction of erroneous findings in the earlier study. Thanks to improved information procedures, a reduction has been achieved in errors in test transcription and ward identification. However, in both the pre- and post-analytic phases, new types of error have emerged, particularly those attributable to the staff's application of novel information system procedures. Further studies confirm that the pre- and post-analytical phases are much more error-prone than the analytic phase. 29,30
Frequency and types of errors according to the phase of the TTP (data from reference 28 )
Pre-pre and post-post-analytical steps
While the concept of brain-to-brain loop was developed by Lundberg in 1981, laboratory professionals were not concerned enough about the initial and final TTP steps, namely the appropriateness of test requesting, patient and specimen identification and, respectively, the physician's reaction to the laboratory report, and the interpretation and utilization of laboratory results. 31,32 However, on exploring the beginning and the end of the loop, it emerges that currently these steps, performed neither in the clinical laboratory nor, at least in part, under the control of laboratory personnel, are more error-prone than others. 33,34 Recent data on errors in the pre-pre analytical phase – initial procedures performed neither in the clinical laboratory nor, at least in part, under the control of laboratory personnel – underline that failures to order appropriate diagnostic tests, including laboratory tests, accounted for 55% of observed incidents of missed and delayed diagnoses in the ambulatory setting and 58% of errors in the Emergency department. 35–38
In the final steps of the loop, the incorrect interpretation of diagnostic or laboratory tests was found to be responsible for a high percentage of errors in the ambulatory setting as well as in Emergency departments (Table 3). A very recent paper underlined that failure to inform outpatients of clinically significant abnormal test results or to document that the relevant information has been given, appear to be relatively common, occurring in one of every 14 tests. Examples include patients not being informed of results of total cholesterol as high as 8.2 mmol/L (318 mg/dL), a haematocrit level as low as 28.6% and a potassium level as low as 2.6 mmol/L. The overall rate of failure to inform the patient or record/document communication of information was 7.1%, ranging between practices from 0% to 26%. 40 This failure to inform patients of clinically important results hinders a move away from the traditional paternalistic role of physicians towards a new model incorporating ‘shared decision-making’ in which the physician attempts to provide the patient and family with the full range of information, including laboratory results, about the clinical condition. 41 Further evidence of errors in reacting to laboratory information is given in a study on the prescription of potassium despite the presence of hyperkalemia. 42 Another study found that more than 2% (2.6% in 2000, 2.1% in 2007) of patients with thyrotropin (TSH) results higher than 20 mU/mL had no follow-up. 43 Finally, an interesting study of hospital inpatients showed almost half of 1095 discharged patients had laboratory and radiology test results pending and that 9% of these results were potentially actionable. 44 Overall, the above data demonstrate that the initial and final steps of the TTP process, in particular test requesting and reaction to laboratory results, not only are more error-prone than all the other steps, but are more important causes of potential adverse outcomes for patients. Currently available data on the relative frequency of errors in the TTP are summarized in Table 4.
Post-post analytical errors: frequency of incorrect interpretation of diagnostic tests in different clinical settings
Types and relative frequency of errors in the different phases of the TTP (data from reference 7 )
Errors in POCT and alternative site testing
In the literature, data on errors in POCT are scarce, the main focus being on analytic errors. The claimed advantage of POCT, in addition to its reduced turnaround-time is that it calls for fewer steps in producing laboratory results. In addition, ‘errors originating during transport are substantially reduced and post-analytical errors are practically totally eliminated, since results are presented directly to the care-giver’. 45 This, in turn, should reduce associated errors. However, despite the illusion of simplicity, POCT devices are affected by several environmental and operator-related factors. Managing the pre-, intra- and post-analytic processes is a major challenge in POCT, just as it is in centralized laboratories. Recently we analysed errors and patient safety problems related to POCT adopting a modified Kost error classification framework that takes into account all steps of the testing process, thus demonstrating that POCT reduces errors and risks of error only in a few steps of the entire testing process. 46,47 Furthermore, from a risk management perspective, POCT has given rise to new and serious challenges, particularly in relation to operator competence and non-adherence to procedures. A potentially more dangerous possibility is that the rapid availability of results and immediate therapeutic intervention might amplify the clinical impact of errors and translate into adverse events for patients. 48,49 Recently, we have demonstrated a significant number of errors in data transcription and incomplete data reported using portable glucose meters in the hospital setting, thus stressing the vulnerability of post-analytical phase when using POCT. 50 While these errors do not arise in the laboratory, they pertain to the utilization of results by clinicians and care-givers and, as part of the overall testing and diagnostic process, should be taken into consideration and managed according to a patient-centred perspective. TTP thus provides the unique framework for analyzing and reducing errors and the risk of errors, not only in ‘centralized’ laboratory testing but also in POCT and all other alternative site testing options.
Impact of errors in laboratory medicine
It seems likely that only a small proportion of laboratory errors results in actual patient harm and adverse events thanks to the several barriers and defensive layers present between the release of laboratory information, the decision-making process and, ultimately, the action on the patient. The data reported in the literature on the impact of laboratory errors on patient care are summarized in Table 5.
Impact of errors in laboratory medicine on patient outcomes
The risk of adverse events and inappropriate care due to laboratory errors ranges from 2.7% to 12%, while in a larger percentage of cases (24.4% to 30%), the laboratory error translates into a patient care problem. In the studies published by our group, errors resulted in inappropriate admission to critical care units, inappropriate transfusions, modifications in heparin and digoxin therapies. 27,28 The impact of laboratory error on the patient's journey as regards further inappropriate investigations (both laboratory and imaging examinations) and more invasive testing and additional consultations is much higher and although not necessarily harmful, creates discomfort and incurs higher costs for both patients and the health-care system. From a risk management viewpoint, the great majority of laboratory errors with little direct impact on patient care provide important learning opportunities. In fact, any error, regardless of its apparent triviality, might indicate weaknesses in policies and procedures that may not lead to adverse events in their particular context, but might cause the patient harm in slightly different circumstances. Therefore, a suitable system for grading laboratory errors according to their seriousness should help identify priorities for quality improvement and focus corrective/preventive actions; the grading system would be designed to consider not only the real patient harm sustained but also the potential worst-case outcome if such an error were to recur. 52 According to the ISO Technical Specification ‘Medical laboratories-reduction of error through risk management and continual improvement’, any clinical laboratory must implement processes for: (a) identifying high-risk processes where the potential error could lead to a safety risk for patients; (b) identifying actual incidents associated with deviations from standard requirements; (c) estimating and evaluating the associated risks to patient safety; (d) controlling these risks and (e) monitoring the effectiveness of the control undertaken. 8 In addition to the ISO/TS 22367, a recent proposal, with several merits, suggests that it is possible to assign both an actual (A) and a potential (P) score to describe the seriousness of an individual laboratory error by grading it according to a 5 point severity scoring system based on patient outcome. 4 The lower score identifies ‘no change in patient management; no adverse clinical outcome’ as a result of the individual error; and the higher score, ‘significant adverse clinical outcome’. In a recent study using this score system over a 30-month period and considering 714,988 requests for laboratory tests received and 658 errors, 75% of errors were given an ‘A’ score of 1 (no adverse event) while 67.9% were allocated on a ‘P’ score of 5 (potential significant adverse clinical outcome). Once again, these data demonstrate that laboratory errors may play a significant role in affecting the overall quality of patient care, including its safety.
Paradigms of error and strategies to improve patient safety
The human error problem, particularly error in medicine, can be viewed in three ways: the person, the legal and the system model. 53
Person approach
The longstanding and widespread tradition of the person approach focuses on the unsafe act, errors and procedural violations of individuals at the sharp end: nurses, physicians, surgeons, anaesthetists, pharmacists and, in rare cases, laboratorians. It views unsafe acts as arising primarily from aberrant mental processes such as forgetfulness, inattention, poor motivation, carelessness, negligence and recklessness. Countermeasures, directed mainly at reducing unwanted variability in human behaviour include disciplinary measures, threat of litigation, retraining, blaming and shaming. The person approach, the dominant tradition in medicine, has serious shortcomings: it precludes a detailed analysis of mishaps, incidents, near-misses and isolates unsafe acts from their system context, thus precluding an effective risk management policy. 54
Legal approach
According to this model, responsible professionals should not make errors as this is part of the duty of care. Such errors are rare but sufficient to cause adverse events to patients. Errors with negative consequences are considered due to negligence or even recklessness and therefore call for sanctions. From this perspective, the connection between proximal actions and bad outcomes is far easier to prove than that between organizational issues and management decisions. The convenience for lawyers in chasing individual errors rather than collective ones is further reinforced by the willingness of professionals, including physicians, to accept responsibility for their actions. This model has several drawbacks, including the fact that often the best people make errors. Even worse, it prevents any initiative designed to disclose medical errors. Hospitals fear public disclosure of reports, which damage reputation, and cause loss of business, and litigation, while experts agree that a voluntary system for the reporting of medical errors and adverse events has great potential for improving safety. 55,56 The legal approach, furthermore, encourages defensive medicine which can, in the laboratory setting, translate into excessive and inappropriate testing, thus leading to excessive costs and related inefficiencies.
System approach
The basic premise in the system approach is that humans are fallible and errors are to be expected, even in the best possible organizations. Errors, seen as consequences rather than causes, originate in systemic factors, including recurrent error traps in the workplace and the organizational processes that give rise to them. Countermeasures are based on the assumption that although the human condition cannot be changed, the conditions under which humans work can be improved upon. In particular, defence, barriers and safeguards occupy a central role in this approach. High-technology systems, including clinical laboratories, have many defensive layers but sometimes they are riddled with holes like slices of Swiss cheese and the holes in the numerous layers may momentarily line up to permit a trajectory of accident opportunity, bringing hazards into damaging contact with victims. 57 The practice of laboratory medicine is highly complex. Of the factors linked to the complexity of TTP, perhaps the most significant are the several steps and the different professionals involved in those steps, which are only partially under the control of the laboratory professionals. Figure 2 shows the Swiss cheese model adapted to the specific setting of laboratory medicine, focusing on the most important gaps, and defence layers, the most effective of which are the identification and documentation of all processes and procedures, automation and simplification, adequate personnel training, supervision and quality indicators. According to this model, the ability to detect the incipient indicators and the collective will to implement corrective measures are essential prerequisites of an effective risk management programme. Process control and proactive hazards analysis tools such as FMEA (failure mode and effect analysis), HACCP (hazards analysis and critical control points) and HAZOP (hazards and operability studies) have already demonstrated their effectiveness in identifying weaknesses in laboratory processes and minimizing the risk of errors. 58–60
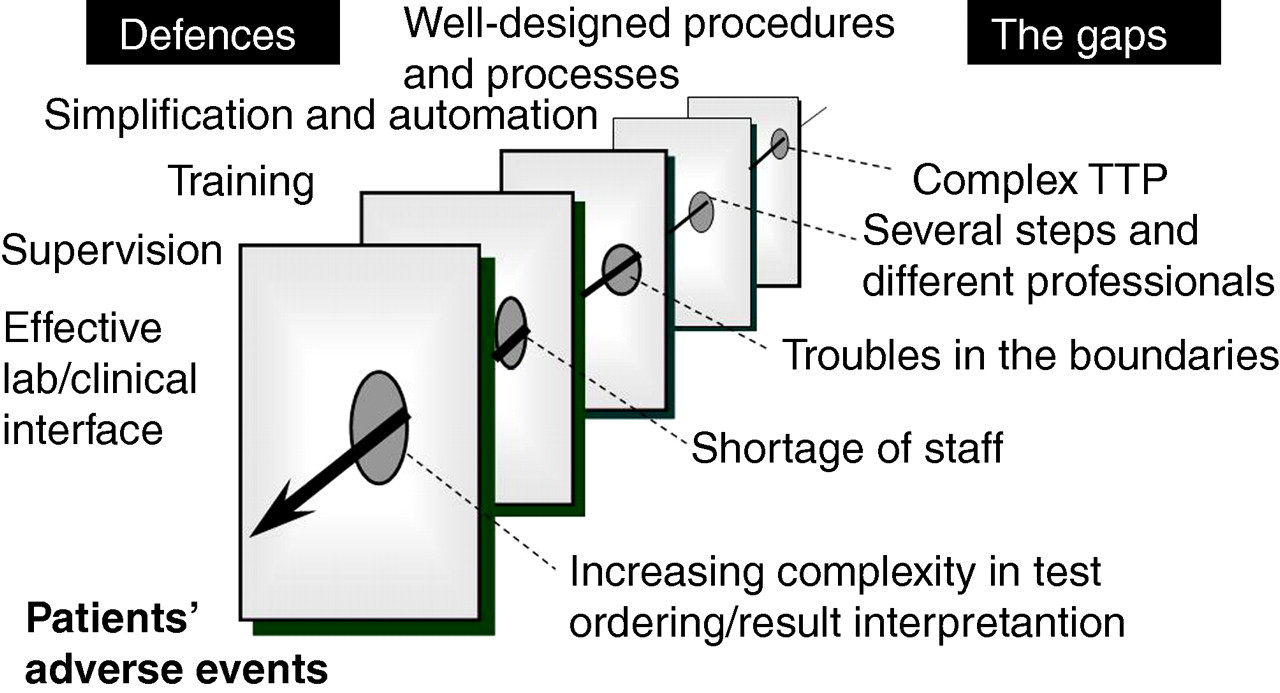
The Swiss cheese model applied to laboratory medicine: the gaps and defences. According to the model described by Reason 57 , the presence of holes in any one defensive layer does not normally cause adverse events. Usually this happens only when the holes in many layers line up to permit a trajectory of accident opportunity
Processes to reduce errors in laboratory medicine
In the last few years, in addition to efforts aiming to reduce analytic errors and improve analytic quality, important achievements have been made in addressing errors in laboratory medicine. Thanks to the introduction of pre-analytic workstations, a significant reduction has been achieved in pre-analytic errors in the automation of procedures such as specimen preparation, centrifugation, aliquoting, pipetting and sorting. 61,62 The increasing interest shown in developing guidelines and standard operating procedures for patient identification, blood collection, sample handling and specimen acceptance or rejection will surely translate into higher quality standards. 63–65 Likewise, significant improvements have been made to the postanalytic phase in data transcription as a result of interfacing analysers and laboratory information systems. Importantly, data transcription is a source of serious errors, particularly if many numbers and results have to be entered into the laboratory computer manually. Further important achievements in the post-analytic phase concern policies and procedures used for reporting critical values as well as initiatives to better understand and improve upon the efficiency of test report delivery to requesting physicians. 66,67 Automatic computerized communication systems have recently been developed to improve the timeliness of notification and avoid potential errors for which accreditation programmes require read-back of the result. After being validated by laboratory physicians on call, critical values are automatically communicated (in real time) to the clinicians, short message services or alert messages appearing on desktop computers. 67,68 These IT systems, which improve the likelihood of reaching the physician on call, are easily adapted to reach patients on their mobile phone or desktop computer, thereby representing an effective means of reducing or indeed eliminating the failure to communicate abnormal outpatient test results to users. Further developments concern the introduction of more effective automated procedures for data validation and reporting as well as the implementation of systems which allows an effective knowledge management to support data interpretation and clinical decision-making at the point of care. 69 At the simplest this can include a direct link into the laboratory handbook giving guidance on interpretation as well as the procedural information required to carry out that investigation on the individual patient. 70 Similar tools should be used to improve the appropriateness of test requesting. The accurate analysis of all testing processes and documented procedures through proactive tools such as FMEA and HAZOP have already proven effective in reducing the risk probability index and, therefore, in improving patient safety in laboratory testing. 58–60 These proactive tools are increasingly, and more readily, accepted by laboratorians and clinicians because they exploit professional competences through a positive approach to problems by focusing on the examination of the entire testing process, thus anticipating major adverse events and pre-emptively implementing changes to prevent them.
International initiatives to reduce errors in laboratory medicine
Recently, the World Alliance for Patient Safety (promoted by the World Health Assembly in 2004 to improve patient safety as a global initiative) included the communication of critical test results among 23 potential patient safety solution topics, thus acknowledging the importance of avoiding errors in laboratory testing.
71
The second goal of the Joint Commission 2008 National Patient Safety Goals for Laboratories is to ‘improve the effectiveness of communication among care-givers’, the first goal being to improve ‘the accuracy of patient identification’, thus underlining the initial and final steps of the testing process.
72
The Working Group on ‘Laboratory errors and patient Safety’ (WG-LEPS) of the International Federation of Clinical Chemistry and Laboratory Medicine (IFCC) has undertaken a project named ‘Model of quality indicators’ based on the identification of valuable and consensually accepted quality indicators in all steps of the testing process. Briefly, 25 quality indicators were selected after discussing and analysing the proposal made by 26 clinical laboratories enrolled in the Working Group: 16 for the pre-analytic, three for the analytic and six for the post-analytic phase. Currently, participant laboratories may introduce the data collected in their own institution on each and all quality indicators in a specifically developed website (
A further proposal is to undertake a project aimed at identifying and promoting the adoption of a sentinel event policy in laboratory medicine. A sentinel event is an unexpected occurrence involving death or serious physical or psychological injury, or the risk thereof, thus signalling the need for immediate investigation and response. The terms ‘sentinel event’ and ‘medical error’ are not synonymous: not all sentinel events occur because of an error and nor do all errors result in sentinel events. Since the assessment of clinical outcomes in relation to laboratory diagnostics is notoriously challenging, a further problem is the identification of those laboratory events arising across the totality of the testing process that are most closely associated with patient harm. This highlights the compelling need for the development and use of reliable and universally agreed performance indicators that would reflect the ‘best practice’ throughout TTP as well as the identification of ‘laboratory sentinel events’ that would be conducive to gaining further knowledge on incidents, and hold providers accountable for patient safety. Available data indicate that potential ‘sentinel events’ might include inappropriate test requests for critical diseases (e.g. myocardial infarction, pulmonary embolism), patient misidentification, the use of inappropriate assays, severe analytical errors, critical tests performed on unsuitable samples (e.g. haemolysed, clotted), the release of laboratory results in spite of poor quality control results, the failure to alert critical values and the wrong report destination. 74 Finally, the lesson we have learnt from the worst laboratory error in Italy (a report transcription error resulting in HIV transmission to three transplanted patients) is the need to avoid manual transcription of data. 75 This tragic event caused by a human error, once again, demonstrated weaknesses in the system and holes in the defensive layers. In particular, it was underlined that this incident occurred because of ‘inadequate awareness of the specificity of the donation process and the non-evaluation of the consequences for the already transplanted patients or on waiting lists and for the personnel involved’ and related procedures. 75 Taking into consideration current international initiatives and recommendations, some priority areas of improvement in patient safety and in error reduction in laboratory medicine might be summarized, as shown in Table 6.
Priority areas of patient safety improvement in laboratory medicine
Conclusions
In the last two decades significant advances have been achieved in the comprehension and reduction of errors in medicine. Finally, those involved are aware that, rather than being caused by ‘bad’ people, errors are indicative of weaknesses of the system, a system that includes almost all the processes and methods we use to organize and carry out virtually everything we do in medicine, including laboratory medicine. The first lesson we have learnt is, therefore, that system theory works and that errors and injuries can be prevented by redesigning systems so as to make it difficult for care-givers to make mistakes. In laboratory medicine, process analysis, the recording/documentation of all procedures and processes according to quality standards, particularly the ISO 15189: 2007 which has been specifically developed for medical laboratories, are key tools for changing and improving upon everyday clinical practice. 76 The accurate analysis and control of all procedures and processes included in the testing process, particularly if effective tools such as FMEA and HAZOP techniques are adopted, may significantly reduce weaknesses and vulnerable steps, thus maximising patient safety. In laboratory medicine we have learnt that TTP is the unique framework for identifying and reducing error, including initial steps such as patient identification and appropriateness in test requesting, and final steps, such as communication and interpretation of test results.
The second lesson is that teamwork is the essence of safety, particularly if we wish to improve the appropriateness of test requesting and the reaction to test results. The availability of expert support systems, which provide information on diagnostic efficiency and interpretation criteria at the point of care, may play a role, but multidisciplinary co-operation and collaboration is mandatory for assuring a patient-centred approach to error reduction. International projects aiming to develop quality indicators for all steps in the testing process, and to establish related quality specifications, may enable clinical laboratories to compare, monitor and improve their performances in the every-day practice, not only in the analytic phase. Finally, the goals selected by international organizations, such as the World Alliance for Patient Safety and the Joint Commission, should lead to the prioritization of improvement programmes addressing well-recognized critical issues, such as patient identification and communication of laboratory results.
DECLARATIONS