
Abstract
Increased high-density lipoprotein (HDL)-cholesterol (hyperalphalipoproteinaemia; HALP) is commonly genetic, but may have secondary causes. An association between multiple lipomatosis and HALP has been reported; however, the mechanism for this is unclear. We report the case of a 69-year-old Cook Island woman with extreme HALP who presented with a large paraspinal lipoma. Magnetic resonance imaging showed no other lipomas. She had the metabolic syndrome, a family history suggestive of lipomas and was on lipid-lowering and antihypertensive therapy. Her plasma HDL-cholesterol concentration was 4.9 mmol/L (>95th percentile for age and sex) and was not explained by typical secondary causes. HDL2 and HDL3 subfractions were increased, with HDL2 predominance. The excised lipoma histology demonstrated benign tissue and normal karyotype. Postoperative lipid profiles showed no change in HDL-cholesterol concentrations. In summary, we report a case of extreme HALP that persisted after excision of a solitary paraspinal lipoma.
Introduction
Plasma high-density lipoprotein (HDL)-cholesterol concentrations show an inverse relationship to atherosclerotic cardiovascular disease. 1,2 There has been renewed interest in the protective effects of HDL-cholesterol on both atherosclerosis and coronary heart disease. 1,2 This relates, in part, to the ability of HDL to promote cellular cholesterol efflux and mediate the transport of cholesterol from peripheral tissues to the liver (i.e. reverse cholesterol transport), and also to intrinsic anti-atherosclerotic properties.
Increased HDL-cholesterol (hyperalphalipoproteinaemia; HALP) may be inherited or acquired. 3,4 Primary causes include familial syndromes, which in some cases may be associated with resistance to atherosclerosis and possible longevity. 3,4 Secondary causes are commonly due to environmental factors and medications, i.e. chronic high alcohol intake, oral oestrogen replacement therapy, extensive aerobic exercise, and treatment with fibrates, niacin or statins. 5
An association between multiple lipomatosis and HALP has been reported. 6,7 Although the mechanism for this relationship is unclear, increased lipoprotein lipase (LPL) enzyme activity in lipomatous tissue has been implicated in some cases of HALP. 6–8
We report a case of extreme HALP in a patient with a solitary paraspinal lipoma.
Clinical case
A 69-year-old Cook Island woman presented with a three-month history of an enlarging non-tender right paraspinal mass. The patient reported no history of trauma or other masses, had no systemic or constitutional symptoms, and denied any dyspnoea or cardiovascular symptoms. She was a smoker with a 15 pack-year history, consumed 20 g of alcohol per day and exercised moderately. Her medications included low-dose statin, angiotensin-converting enzyme inhibitor, thiazide diuretic and a β-blocker. A family history of similar lumps in one of her children, brother and distant maternal relatives was obtained. However, their nature was not ascertained.
On physical examination she appeared well, with a body mass index of 27 kg/m2 (weight 75 kg, height 1.66 m), waist circumference of 100 cm, pulse rate of 70 beats/min and blood pressure of 130/80 mmHg. A firm, non-mobile, non-tender 18 cm (height) × 7 cm (width) mass was present in the right lower paraspinal region. No other masses were found. A systemic examination was otherwise unremarkable.
Magnetic resonance (MR) imaging of the thoraco-lumbar spine showed a well-defined 17 × 4 × 7.5 cm intramuscular paraspinal lipoma with no evidence of sarcomatous change. Computerized tomography (CT) imaging of the chest and upper abdomen showed several small nodules in the upper lung lobes of indeterminate significance. No mediastinal mass was detected.
A lipid profile taken at that time showed very high plasma HDL-cholesterol and apolipoprotein (apo) A-I (the primary apoprotein of HDL) concentrations of 4.9 mmol/L and 3.34 g/L, respectively (both >95th perecentile for age and sex). Lipoprotein electrophoresis confirmed a prominent increase in the α-lipoprotein band. HDL2 and HDL3 subfractions were increased, with the cardioprotective HDL2 subfraction predominant. Serum liver function tests revealed an isolated mild increase in gamma glutamyltransferase of 98 U/L (<50), possibly related to her alcohol intake and fatty liver. A carcinoembryonic antigen (CEA) was 20 μg/L (<3 for non-smokers) and antimitochondrial antibodies were negative. The elevation in her CEA may be related to the pulmonary nodules. Follow-up CT imaging of the chest (four months later) revealed no change in the appearance of the nodules and her CEA concentration remained stable.
Lipomatous tissue (Figure 1) and normal adipose tissue (taken ∼5 cm distant to the lipomatous tissue) were surgically removed and samples were stored at −80°C for LPL analyses. Histology and cytogenetic studies confirmed a benign intramuscular lipoma with normal female karyotype. The patient made an uneventful recovery. Fasting lipid profiles were taken immediately preoperatively, and at days 1, 15 and 90 postoperatively, with no significant temporal changes in HDL-cholesterol concentrations observed (Table 1).
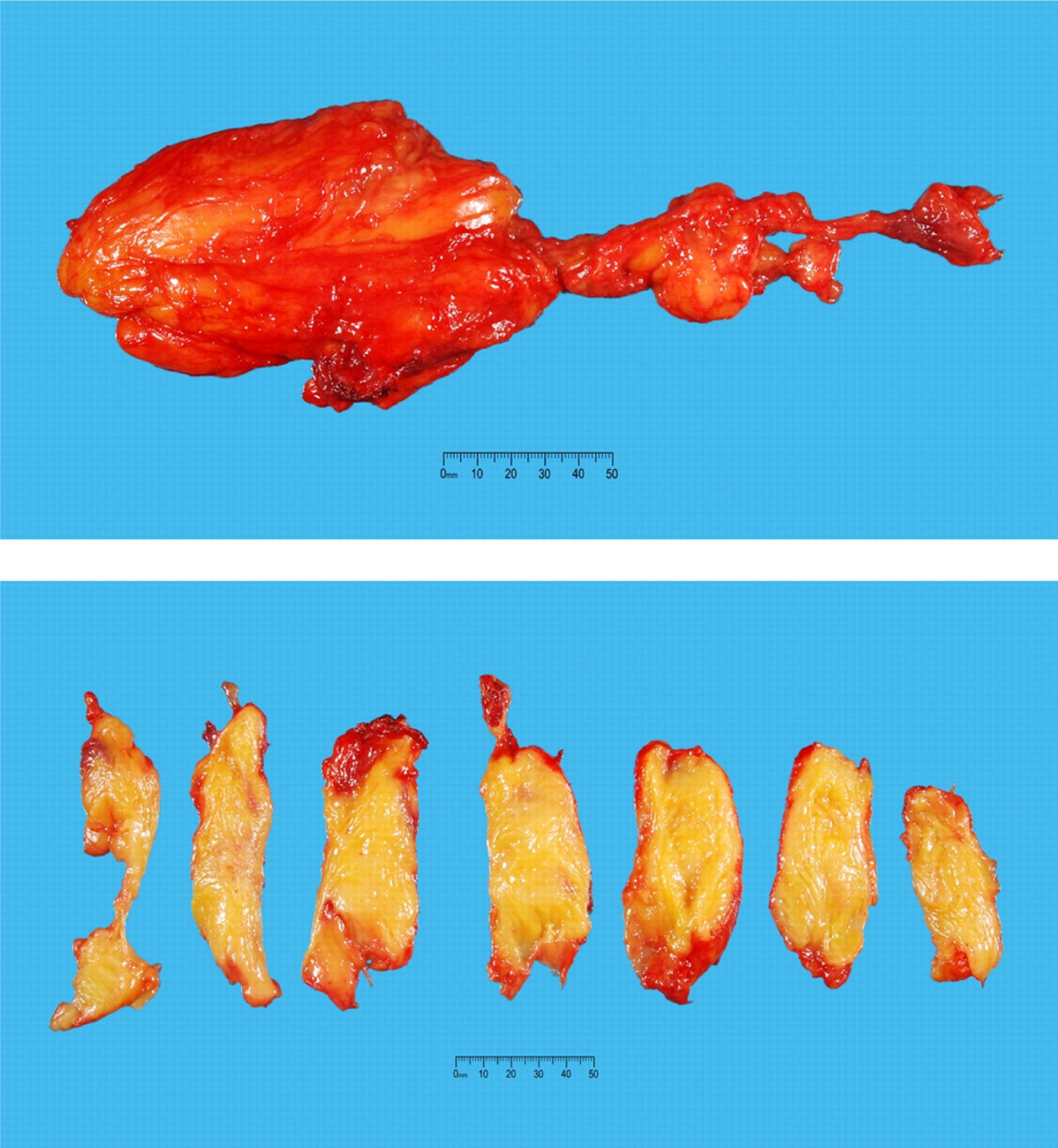
Macroscopic photographs of the solitary paraspinal lipoma
Biochemical investigations before and after surgical removal of the paraspinal lipoma
D = days from −12 to 90 days postoperatively. Sample taken at D0 = day of surgery was preoperatively. TC, total cholesterol; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; TG, triglyceride; ApoA-I, apolipoprotein A-I; ApoA-II, apolipoprotein A-II; ApoB, apolipoprotein B; Lp(a), lipoprotein (a); GGT, gamma glutamyltransferase; CEA, carcinoembryonic antigen; HbA1c, haemoglobin A1c
Molecular studies for cholesterol ester transfer protein (CETP), hepatic lipase (LIPC) and lecithin: cholesterol acyl transferase protein (LCAT) genes were performed.
Method
LPL activity was measured in the lipomatous tissue and normal adipose tissue by the method of Krauss et al.
9
with modifications. In brief, 30–60 mg aliquots of tissue were homogenized for 10 s in 1 mL of buffer (50 mmol/L NH4OH · HCl, pH 8.5 containing 5 mg heparin/100 mL buffer) in borosilicate glass tubes on ice. Tubes were then incubated for 40 min in a shaking water bath at 37°C, then centrifuged at 2000 ×
Plasma LPL activity was measured using Triolein as a substrate in the presence of heat inactivated serum (apoC-II source). After the addition of substrate, incubations were performed in duplicate for 60, 90 and 120 min at 37°C in a shaking water bath. The oleic acid released was extracted into hexane, dried down under nitrogen and then quantitated by high-performance liquid chromatography (HPLC) with ultraviolet detection, using linolenic acid as an internal standard. HPLC separation was performed using an isocratic mobile phase containing acetonitrile:dH2O, 90:10 containing 0.1% trifluoroacetic acid. Separation was on a Merck Lichrocart 250 × 4 mm, 5 μm RP C-18e column with a Nova-Pak C18 4 μm guard column assembly. The flow rate was 1 mL/min and the injection volume was 120 μL. Oleic acid and linolenic acid were both monitored at 210 nm and the run time was 25 min. The intra-assay coefficient of variation (CV) for the duplicate samples was <5%, and the inter-assay CV for a plasma control was <10%.
Genomic DNA was extracted from blood using a commercially available salting-out procedure (Gentra PUREGENE DNA Purification kit). The CETP, LCAT and LIPC genes were amplified by polymerase chain reaction (PCR) and sequencing reactions performed using BigDye Terminator chemistry. Primers were designed to cover exons and exon–intron boundaries.
Results
LPL activity for lipomatous and normal adipose tissue was 43 and 47 nmol free fatty acid (FFA)/mg protein/h, respectively.
No abnormalities that could account for the HALP were found in the CETP, LCAT or LIPC genes.
Discussion
Epidemiological data indicate the 95th percentile for HDL-cholesterol in a 69-year-old white women to be ∼2.5 mmol/L. 10 Of 48,845 HDL-cholesterol measurements performed over the last three years in our laboratory, only 0.36% showed concentrations >3.0 mmol/L, with less than 0.12% >3.5 mmol/L. HDL-cholesterol concentrations are affected by genetic as well as environmental factors, diet and drugs. 3 Primary causes for HALP include CETP and hepatic lipase deficiency, scavenger receptor B1 mutations, up-regulation of apoA-I and LCAT overexpression. 3 These disorders are relatively uncommon and may show ethnic or racial variation, e.g. CETP deficiency is present in 61.7% of Japanese with HALP (HDL-cholesterol >2.59 mmol/L). 11
Secondary causes of HALP include vigorous sustained exercise, regular substantial alcohol intake, primary biliary cirrhosis and medications, e.g. oestrogens, phenytoin, fibrates, nicotinic acid and statins. 3 HALP is a common finding in multiple symmetric lipomatosis (MSL), a disease characterized by slowly growing symmetrical fat masses mainly in the upper body that may be familial in nature. 6,7 MSL has been reported to be associated with a metabolic abnormalities, including glucose intolerance, a variety of hyperlipidaemias (increased VLDL and chylomicrons) and hyperuricaemia. 6,7 Asymmetrical lipomatosis has been associated with hyperlipidaemia, considered to be familial combined hyperlipidaemia, with the presence of HALP. 12
HDL-cholesterol concentrations in MSL patients (n = 15) were 1.6-fold greater than control patients, mainly due to a two-fold increase in the HDL2 subfraction. Furthermore, LPL activity of the lipomatous tissue (n = 10) was nine-fold greater than that found in adipose tissue from control patients and was correlated with HDL2 levels. 6 A lesser increase in LPL activity (2.6-fold) was reported in lipomatous tissue (n = 13) when compared with adjacent normal adipose tissue. 13 Of interest, adipose tissue LPL activity also correlates closely with HDL-cholesterol concentrations in normal subjects. 14
It has been proposed that increased adipose LPL activity could account for the combination of abnormal fat accumulation and HALP in MSL. 6,13 However, the LPL activity in our patient's lipoma and adjacent normal adipose tissue was similar. Of interest, the LPL activity in our patient was higher than that previously reported. 6 This finding may, in part, relate to a systemic effect of focal abnormalities of adipose tissue expansion on LPL activity or method-related differences. Other metabolic abnormalities have been observed in MSL patients including hyperuricaemia and insulin resistance. 7 Our patient had no clinical or radiological evidence of multiple lipomas. She had no clinical evidence of peripheral neuropathy, a common finding in MSL, 15 but evident features of the metabolic syndrome, being overweight with central adiposity, fasting hyperglycaemia and hyperuricaemia.
Although lipomatous tumours are common, no association between solitary lipomas and HALP has been demonstrated. Moreover, solitary lipomas and multiple lipomas are cytogenetically distinct. 16 An MSL case with HALP (HDL-cholesterol 3.6 mmol/L) showed unaltered HDL-cholesterol levels after removal of a lipoma mass, possibly related to incomplete surgical excision. 7 Our patient had extreme HALP with no clinical or radiological evidence of MSL. However, MR imaging was restricted to the thoraco-lumber region. Likewise, her HDL-cholesterol concentrations did not alter after surgery, consistent with the presence of normal tissue LPL activity. Moreover, no genetic abnormality in her CETP, LCAT and LIPC genes was demonstrated. Although the aetiology of her HALP remains unexplained, it may be due to a combination of both secondary and as yet unidentified genetic factors. Unfortunately, we could not acquire any blood samples for lipid studies on affected relatives.
In summary, we describe a case of extreme HALP that persisted after excision of a solitary paraspinal lipoma.
DECLARATIONS