
Abstract
Background
In gastrectomized subjects, oral glucose tolerance test often shows marked hyperglycaemia (oxyhyperglycaemia) after glucose loading. Because serum glycated albumin (GA) has been shown to better reflect postprandial and maximum plasma glucose levels, we investigated whether or not the clinical significance of serum GA and glycated haemoglobin (HbA1C) in non-diabetic gastrectomized subjects differs.
Methods
During health examinations, 62 non-diabetic subjects with a history of gastrectomy and 87 non-diabetic control subjects were selected in the present study. Body mass index (BMI) in the gastrectomy group was significantly lower than in the control group.
Results
Fasting plasma glucose levels were significantly lower in the gastrectomized subjects than in the control subjects. Although both HbA1C and serum GA were significantly higher in the gastrectomized subjects, there was a significant difference in GA/HbA1C ratio between the gastrectomized subjects and the control subjects. BMI-adjusted serum GA, based on our previous finding of inverse influence of BMI on serum GA, was also significantly higher in the gastrectomized subjects than in the controls.
Conclusions
Serum GA is higher relative to HbA1C in gastrectomized subjects. This suggests that serum GA may be a better marker than HbA1C for glycaemic excursion in these subjects.
Introduction
Glycation of various proteins is known to increase in diabetic patients compared with non-diabetic individuals, and is thought to be involved in the onset and progression of some chronic diabetic complications. 1 Among the glycated proteins, glycated haemoglobin (HbA1C) is commonly used clinically as an indicator of glycaemic control. 2,3 The Diabetes Control and Complications Trial recommends that HbA1C be maintained at <7.0% in order to prevent the onset and progression of diabetic complications. 4 The lifespan of erythrocytes is about 120 d, and thus HbA1C reflects glucose control over the preceding 1–2 months. However, measurement of HbA1C values is affected by shortened lifespan of erythrocytes (e.g. haemolytic anaemia, renal anaemia and liver cirrhosis) and variant haemoglobin, which can lead to erroneous values for glucose control. 5,6
Serum glycated albumin (GA) has also been used as a parameter of glucose control. The half-life of serum albumin (about 2 weeks) is shorter than that of erthyrocytes; thus, serum GA reflects glucose control over a shorter term. Moreover, serum GA is not affected by haemoglobin abnormalities, 7 thereby has been recently evaluated as a useful marker for glycaemic control in diabetic patients on dialysis. 8,9 By contrast, in patients who have disorders of albumin metabolism (e.g. nephrotic syndrome, liver cirrhosis and thyroid dysfunction), serum GA is affected and does not accurately reflect glycaemic control. 10 In addition, it has been shown that serum GA is a better indicator for plasma glucose excursions than HbA1C. 11 In that study, HbA1C levels were well correlated with mean plasma glucose levels among daily profile of plasma glucose, while serum GA levels showed stronger correlation with postprandial and maximal plasma glucose levels.
In gastrectomized subjects, oral glucose tolerance test (OGTT) often shows marked hyperglycaemia (oxyhyperglycaemia) 30–60 min after glucose loading, sometimes followed by hypoglycaemia. 12 Thus, plasma glucose levels are thought to show wide variations in gastrectomized subjects. In these subjects, elevated HbA1C levels have been reported previously, 13 but serum GA has not been studied. In this study, we investigated whether or not the significance of measuring serum GA and HbA1C differs in non-diabetic gastrectomized subjects.
Methods
Subjects and controls
During health examinations at Kinki Central Hospital between August 2006 and February 2008, subjects with a history of gastrectomy were identified, and those with a fasting plasma glucose (FPG) of <126 mg/dL were selected as the study group. As controls, age- and gender-matched subjects undergoing health examinations at Kinki Central Hospital between June 2007 and August 2007, and without any history of diabetes or evidence of a diabetic pattern on OGTT, were selected. Exclusion criteria in both groups were liver disease (e.g. chronic hepatitis, liver cirrhosis), renal disease, thyroid disease, administration of glucocorticoid and anaemia or treatment for anaemia. There were 62 gastrectomized subjects (43 men and 19 women) and 87 control subjects (56 men and 31 women) (Table 1). Among the 62 gastrectomized subjects, 44 received gastrectomy because of gastric tumourous lesions and 18 because of gastric ulcers. The duration after gastrectomy was 18.2 ±13.3 y. All the study subjects were apparently healthy and their nutritional states were good. They had no abnormalities in blood tests, chest X-ray examination and abdominal echography. In the gastrectomized subjects, body mass index (BMI) and serum albumin levels were significantly lower (P < 0.001) than in the control subjects (Table 1).
Background characteristics of study subjects
Data are means ± SD or numbers
This study was performed in accordance with the principles of the Declaration of Helsinki as revised in 2000. The Institutional Review Board approved the study protocols, and all subjects provided written informed consent.
Laboratory measurements
Fasting blood was collected from subjects between 09:00 and 11:00, and was centrifuged immediately for measurement. Plasma glucose concentrations were determined by the hexokinase glucose-6-phosphate dehydrogenase method. HbA1C was measured by high-performance liquid chromatography using ADAMS-A1C HA-8160 (Arkray Inc, Kyoto, Japan). 14 Inter-assay coefficient variations as determined in representative blood samples (5.3% and 10.4% HbA1C) were 0.85% and 0.67%, respectively. Serum GA was determined with a Hitachi 7600 autoanalyser (Hitachi Instruments Service Co, Tokyo, Japan) by an enzymatic method using albumin-specific proteinase, ketoamine oxidase and albumin assay reagent (Lucica GA-L; Asahi Kasei Pharma Co, Tokyo, Japan). 15,16 Inter-assay coefficient variations as determined in representative serum samples (13.3% and 34.9% GA) were 1.38% and 1.32%, respectively.
Serum GA and GA/HbA1C ratio were adjusted for BMI using previously reported correlations between BMI and serum GA and those between BMI and GA/HbA1C ratio in non-diabetic subjects. 17
Statistical analyses
All data are shown as means ± SD. For statistical analyses, unpaired Student's t-test was used to compare two groups. To analyse the correlation between HbA1C and serum GA, univariate regression analysis was performed with the StatView computer program (Version 5.0 for Windows, Abacus Concepts, Berkeley, CA, USA). P values of <0.05 were considered to be statistically significant.
Results
FPG levels were significantly lower in the gastrectomized subjects than in the control subjects (97 ± 7 versus 99 ± 9 mg/dL; P = 0.0328). By contrast, both HbA1C (5.4 ± 0.4% versus 5.3 ± 0.3%; P = 0.0167) and serum GA (15.5 ± 1.9% versus 14.3 ± 1.1%; P < 0.0001) were significantly higher in the gastrectomized subjects (Figure 1). In the all studied subjects, serum GA and HbA1C showed a significant correlation (R = 0.571, P < 0.0001; Figure 2). In the gastrectomized subjects, the regression line was shifted upwards from that in the control subjects (y = 3.35x − 2.61 for the gastrectomized subjects, y = 1.56x + 6.05 for the control subjects; Figure 2). GA/HbA1C ratio was significantly higher in the gastrectomized subjects than in the control subjects (2.87 ± 0.27 versus 2.72 ± 0.20; P = 0.0001) (Figure 2). We previously reported that BMI inversely regulates serum GA. 17,18 Thus, serum GA and GA/HbA1C ratio were adjusted for BMI. Comparison of the adjusted values showed that in the gastrectomized subjects serum GA (15.4 ± 1.8% versus 14.5 ± 1.1%; P = 0.0001) and GA/HbA1C ratio (2.82 ± 0.23 versus 2.75 ± 0.18; P = 0.0499) were significantly higher than in the controls (Figure 3).
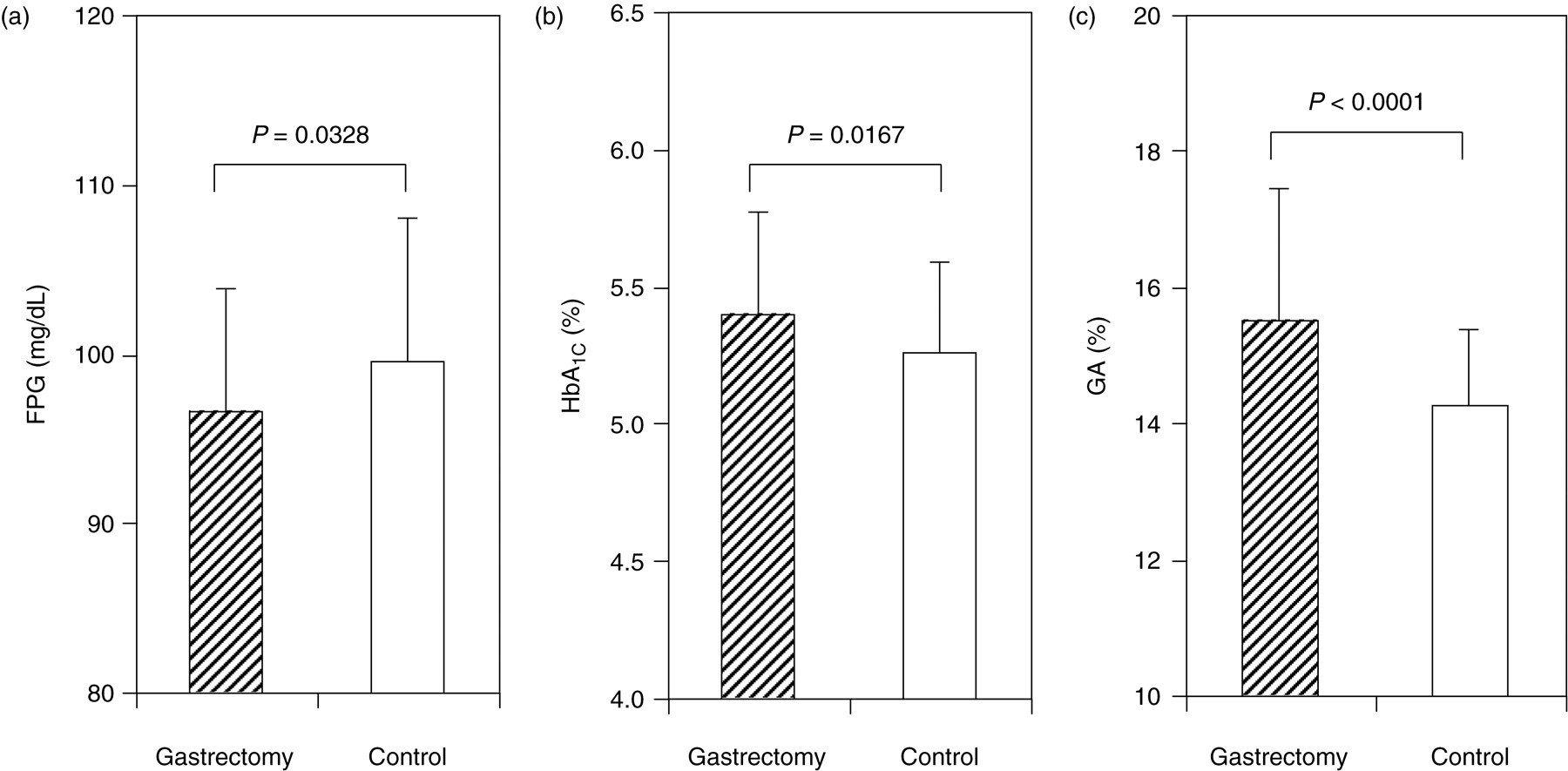
Comparison of FPG (a), HbA1C (b) and serum GA (c) between gastrectomized subjects (hatched column) and control subjects (open column). FPG, fasting plasma glucose; HbA1C, glycated haemoglobin; GA, glycated albumin
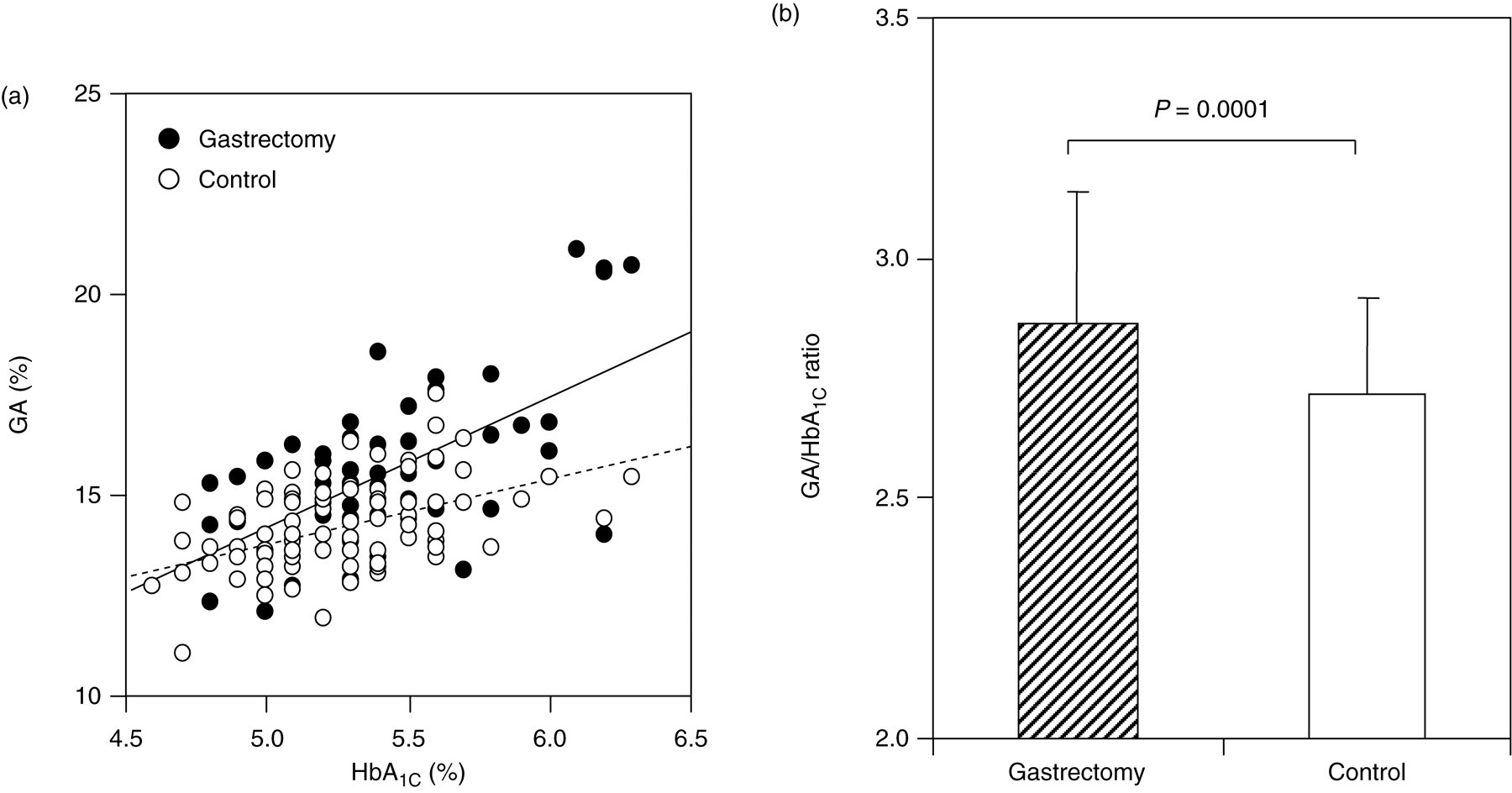
(a) Correlation between HbA1C and serum GA in gastrectomized subjects (closed circles) and control subjects (open circles). (b) Comparison of GA/HbA1C ratio between gastrectomized subjects (hatched column) and control subjects (open column). HbA1C, glycated haemoglobin; GA, glycated albumin
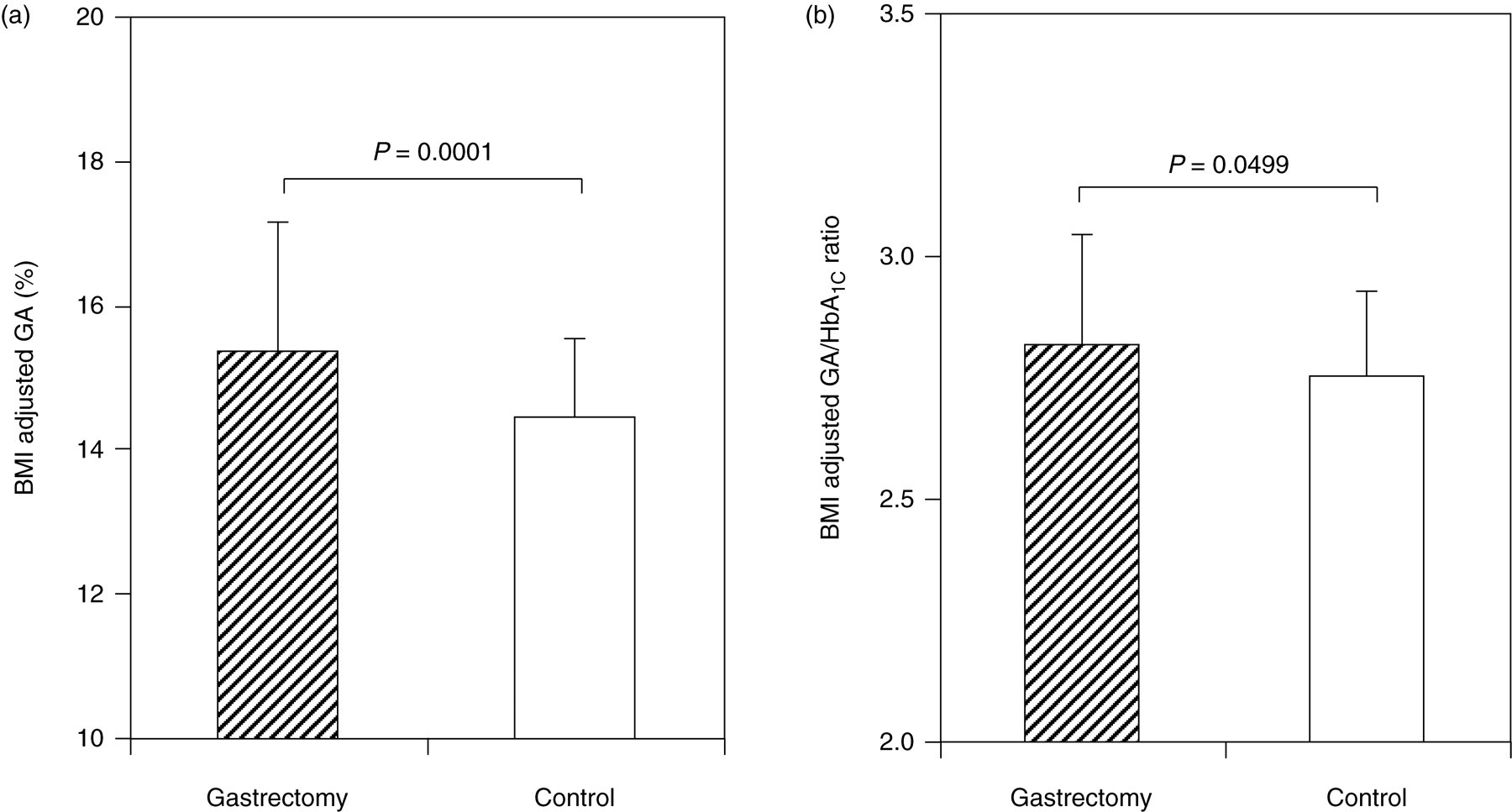
BMI-adjusted serum GA and GA/HbA1C ratio in gastrectomized subjects (hatched column) and subjects (open column). HbA1C, glycated haemoglobin; GA, glycated albumin
Discussion
Our analysis showed that in the gastrectomized subjects, as compared with the control subjects, HbA1C and serum GA were significantly higher in spite of lower levels of FPG. GA/HbA1C ratio was also significantly higher in the gastrectomized subjects, indicating that serum GA was higher relative to HbA1C in the gastrectomized subjects. These results suggest to reflect postprandial hyperglycaemia (the so-called oxyhyperglycaemia) and wide ranges of glycaemic excursion occurring in gastrectomized subjects. 12 We previously reported that BMI inversely regulates serum GA in diabetic and non-diabetic individuals. 17,18 In the gastrectomized subjects of the present study, BMI was significantly lower than in the control subjects. It raises the possibility that lower BMI is attributable to the higher level of GA/HbA1C ratio. In gastrectomized subjects, both serum GA and the GA/HbA1C ratio showed significant inverse correlation with BMI (R = −0.568, P < 0.0001 for serum GA; R = −0.579, P < 0.0001 for GA/HA1C ratio). For this reason, GA/HbA1C ratio was adjusted for BMI, yet the BMI-adjusted GA/HbA1C ratio was also significantly higher in the gastrectomized subjects than in the control subjects. Therefore, in addition to lower body weight as a factor in the elevated serum GA levels in gastrectomized subjects, oxyhyperglycaemia is also thought to play a role in the higher serum GA relative to HbA1C. Our study is the first to report a relative increase in serum GA versus HbA1C in gastrectomized subjects.
In the present study, serum albumin levels were lower in the gastrectomized subjects than in the control subjects. Serum GA levels were expressed as percent of serum albumin, and are shown not to be influenced by serum albumin levels. 19 Thus, it is unlikely that the elevated serum GA relative to HbA1C is attributable to the decreased serum albumin levels.
HbA1C is affected to a greater degree by FPG rather than postprandial glucose levels, whereas serum GA better reflects postprandial glucose than fasting glucose levels. 10 Yoshiuchi et al. 11 have recently reported that GA/HbA1C ratios in patients with type 1 diabetes were significantly higher than in those with type 2 diabetes. They found a significant correlation between GA/HbA1C ratios and maximum glucose levels in diurnal variations, which suggests that higher GA/HbA1C ratios in type 1 diabetes may be due to the large glucose variations. In our study subjects, we did not measure diurnal glucose variations, but postprandial hyperglycaemia is well recognized in gastrectomized subjects. 12 Therefore, as in type 1 diabetes patients, GA/HbA1C ratios is thought to be elevated in subjects who had gastrectomy, probably caused by postprandial hyperglycaemia.
The mechanism by which serum GA better reflects postprandial hyperglycaemia than does HbA1C is unknown. Erythrocyte survival is reduced in diabetics with poor glucose control, 20,21 and if hyperglycaemia shortens red cell survival, this may decrease HbA1C levels. In addition, with acute changes in glucose levels, erythrocyte uptake of glucose, mediated by GLUT1, may lag, and without an increase in erythrocyte glucose concentrations, the increase in HbA1C may be lower. 22 Moreover, with glucose elevations, differences in glycation rates between haemoglobin and albumin may account for the increases in HbA1C that are lower relative to serum GA. 16,23 Further investigation is necessary to clarify the mechanism.
Postprandial hyperglycaemia has been postulated to be associated with increased prevalence of cardiovascular diseases. 24,25 In subjects with postprandial hyperglycaemia, if serum GA is higher relative to HbA1C, then serum GA may be a better marker for glycaemic control in gastrectomized subjects with diabetes. The Shanghai group has recently reported significantly elevated serum GA in subjects with coronary artery stenosis. 26,27 This suggests the need for further investigation of the correlation of postprandial hyperglycaemia or serum GA with cardiovascular diseases in gastrectomized subjects.
DECLARATIONS