
Abstract
Background
Assessment of renal function in patients undergoing coronary artery bypass grafting (CABG) is important. Cystatin C has been proposed as an improved indicator of renal function. The aim of this study was to assess cystatin C as an early marker of changes in glomerular filtration rate (GFR) after CABG.
Methods
Blood samples were collected from 61 CABG patients at different time points. Using 51Cr-ethylenediaminetetraacetic acid (51Cr-EDTA) clearance as a ‘gold standard’, we compared the correlations and non-parametric receiver operator characteristic curves of serum cystatin C, serum creatinine and 24 h creatinine clearance (Ccr).
Results
The inverse of cystatin C correlated better with 51Cr-EDTA than those of serum creatinine and Ccr (r = 0.8578, 0.6771 and 0.6929, respectively). Cystatin C exhibited significantly superior diagnostic accuracy for detecting GFR <80 mL/min/1.73 m2 compared with serum creatinine (P = 0.013) and Ccr (P = 0.025); for detecting GFR <60 mL/min/1.73 m2, cystatin C had similar diagnostic accuracy to Ccr (P = 0.812) but was superior to creatinine (P = 0.033). At the best cut-off value, cystatin C had sensitivity 89% and specificity 93% for detecting GFR <80 mL/min/1.73 m2, sensitivity 86% and specificity 96% for detecting GFR <60 mL/min/1.73 m2.
Conclusions
Cystatin C is a better marker for detecting small temporary changes of GFR in CABG patients. This may allow better identification of patients with renal impairment.
Introduction
Early assessment of renal function in patients undergoing coronary artery bypass grafting (CABG) is important. There are a number of ways of assessing glomerular filtration rate (GFR), considered the best overall index of renal function. Inulin clearance or clearances of other exogenous radiolabelled compounds, such as 51Cr-ethylenediaminetetraacetic acid (51Cr-EDTA), are regarded as the ‘gold standard’ for evaluating GFR. Unfortunately, cost and technical difficulties preclude their routine use in clinical practice. 1,2 Determination of 24 h creatinine clearance (Ccr) has been used to assess GFR 3,4 but collection of an accurate 24 h urine is laborious and poses additional sources of errors. Serum creatinine has been widely used as a marker of GFR for many years, but it can be affected by other non-renal factors, such as muscle mass, dietary intake, changes in tubular secretion and analytical interference by other substances in serum. 5,6 In particular, serum creatinine has an inability to detect renal function impairment of 50% or less. 3 Attempts to improve clinical measurement of GFR include the use of creatinine-based equations such as the Cockroft–Gault (C&G) and Modification of Diet in Renal Disease (MDRD) Study equations. 7–10 These equations also allow only crude estimation of renal function, but improve GFR estimation compared with serum creatinine alone. 2,8,11 More reliable and specific markers of GFR are required.
The protease inhibitor cystatin C has been suggested as an early indicator of impaired renal function, which may be superior to serum creatinine in terms of diagnostic accuracy for reduced GFR. 2,4,12–16 In addition, it has been reported to be a more sensitive marker of changes in GFR than serum creatinine. 17 Therefore, cystatin C would seem to be a promising candidate as a marker of GFR in patients after CABG. However, its role has not been fully investigated in this context, and the outcomes of the very few available studies 9,18 are diverse. In the current study, we assessed cystatin C as a marker of GFR during the early postoperative period after CABG in 61 patients. Cystatin C, creatinine and Ccr were compared with 51Cr-EDTA clearance. In addition, the C&G and MDRD equations were evaluated in this study.
Materials and methods
Patients
The study was approved by the local ethics committee and performed from July 2007 to October 2008 at the cardiological service of the Third Affiliated Hospital of Suzhou University, Jiangsu Province, China. Patients (n = 61, mean [standard deviation] age 65.1 [11.7] years, range: 34–77; 35 males) underwent a thorough examination, including physical examination, clinical history and renal function. All patients stopped taking drugs that are known to influence the tubular secretion of creatinine or its determination. We excluded patients receiving glucocorticoid or thyroid hormone therapy. Patients with preoperative normal renal function (based on a 51Cr-EDTA value >80 mL/min/1.73 m2) were selected for inclusion in this study.
Laboratory methods
Gender, age, height and weight of every patient were recorded preoperatively and their body surface area (BSA) was calculated using the formula BSA (m2) = height (cm)0.725 × weight (kg)0.425 × 0.007184.
19
GFR was assessed by 51Cr-EDTA single-injection method (1 μCi/kg) and blood samples were drawn at 0, 90 and 180 min after injection preoperatively and on days 1, 2, 4 and 7 postoperatively
20
from each patient. An aliquot of time 0 sample was centrifuged and stored at −20°C until analysis of serum creatinine and cystatin C. A 24 h urine collection was completed just before the time 0 blood sample for the determination of urine creatinine. Serum and urine creatinine were measured using a kinetic Jaffe method (Roche Diagnostics, Mannheim, Germany) that is modified to reduce the effect of non-creatinine Jaffe-reacting chromogens. The assay was calibrated with a lyophilized human serum calibrator (c.f.a.s., Roche Diagnostics Ltd, Shanghai, China) so that the creatinine concentration (approximately 320 μmol/L) could be traced to an isotope dilution-mass spectrometry standard. Water was used as the zero standard. The between-day coefficients of variation (CV%) were <3% at concentrations 113 and 333 μmol/L. Serum cystatin C was measured by the particle-enhanced immunonephelometric method (Dade Behring, Marburg, Germany). The intra-assay and inter-assay CVs averaged 3.0% and 4.1%, respectively. All of the analyses were performed on an automated biochemistry analyzer (Hitachi 7600-120E, Tokyo, Japan). Ccr adjusted to BSA was calculated according to the following formula:

GFR was estimated using the following equations:
In this study, by using an average of the serum creatinine and cystatin C concentrations obtained at time 0 min after 51Cr-EDTA injection with the concentrations obtained at the time just before a second 51Cr-EDTA injection, an approximate average serum concentration during each 24 h collection period was calculated. These average values were compared against the preoperative values. The reference range at our hospital for 51Cr-EDTA clearance is from 80 to 120 mL/min/1.73 m2, serum creatinine from 44 to 132 μmol/L and serum cystatin C from 0.6 to 1.20 mg/L.
Statistical analysis
Data were analysed using SPSS 13.0 (SPSS Inc, Chicago, IL, USA) program. Numerical data are presented as mean ± standard deviation and categorical data as proportions. These were compared using t-tests or Wilcoxon-tests for non-normal data and Fisher's exact test for categorical data. Associations between quantitative data were determined using Spearman's test. Receiver operating characteristic (ROC) curve analysis was used to evaluate the diagnostic value of all available markers for identifying renal dysfunction, and the areas under the curve (AUC) were calculated as a summary measure of postoperative renal function. P < 0.05 was considered statistically significant.
Results
The baseline preoperative characteristics of 61 patients in this study are summarized in Table 1.
Baseline preoperative characteristics of 61 patients
BMI, body mass index; MI, myocardial infarction; NYHA, New York Heart Association, a heart failure classification system; LV, left ventricular; SD, standard deviation; MDRD, modification of diet in renal disease; Ccr, creatinine clearance; 51Cr-EDTA, 51Cr-ethylenediaminetetraacetic acid
Renal function during the perioperative period
Preoperatively, all investigated markers were in the reference range for all patients. Postoperatively, 51Cr-EDTA clearance reached a minimum value on day 2. Cystatin C concentration demonstrated a significant rise on day 1 (P < 0.0001) and reached a peak value on day 2. Serum creatinine concentration also peaked on day 2, but there was no significant difference compared with the preoperative concentrations (P = 0.1064). Ccr reached a minimum value on day 2. Compared with 51Cr-EDTA clearance, Ccr differed by <20% in 36 patients and >20% in the remaining 25 patients. The deviations were greater when GFR was estimated by the C&G and MDRD equations (the difference was >20% in 39 patients using either equation).
Correlation of cystatin C with 51Cr-EDTA clearance
Because all available markers reached a minimum or peak value on day 2, we performed linear regression analysis using the data of day 2. As shown in Figure 1, the correlation of 1/cystatin C with 51Cr-EDTA clearance (r = 0.8578, P < 0.0001) was higher than those of Ccr and 1/serum creatinine (both P < 0.05). The correlation between Ccr and 51Cr-EDTA clearance was relatively weak (r = 0.6929, P < 0.0001) and only slightly higher than that between 1/serum creatinine and 51Cr-EDTA (r = 0.6771, P < 0.0001). Estimates of GFR using MDRD (r = 0.5344) and C&G (r = 0.6109), respectively, were weakly correlated with 51Cr-EDTA clearance.
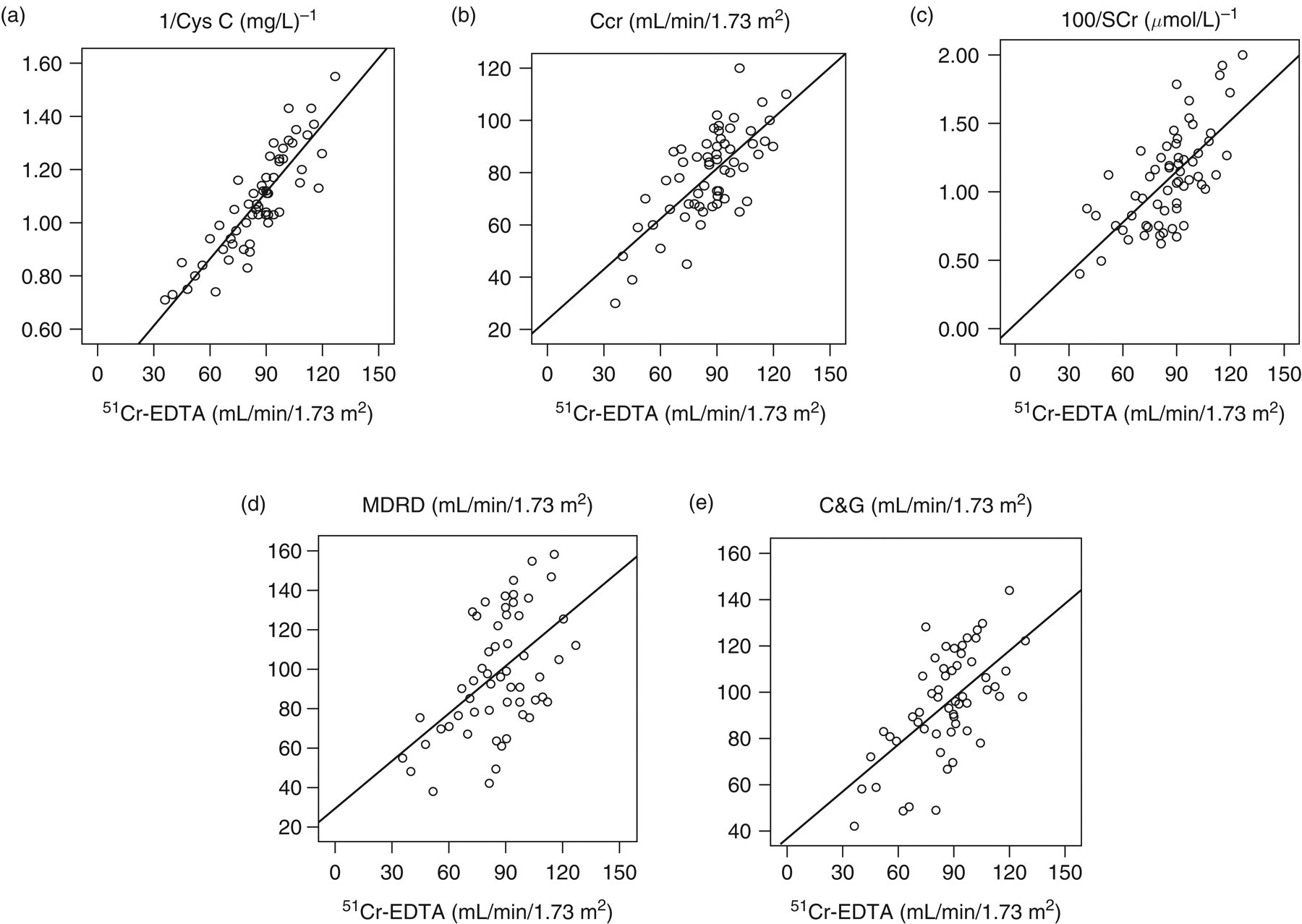
Correlation between GFR markers and 51Cr-EDTA clearance. The inverse of cystatin C (a), Ccr (b), the inverse of serum creatinine (c), MDRD (d) and Cockroft–Gault equation (e) for all the patients included in the study using the data of day 2 postoperation. The correlation coefficient was 0.8578 for 1/cystatin C, 0.6771 for 1/serum creatinine, 0.6929 for Ccr, 0.5344 for MDRD and 0.6109 for Cockroft–Gault equation, respectively. The correlation of 1/cystatin C with 51Cr-EDTA was higher than that of other studied markers (all P < 0.05). GFR, glomerular filtration rate; Ccr, creatinine clearance; 51Cr-EDTA, 51Cr-ethylenediaminetetraacetic acid; MDRD, modification of diet in renal disease
Diagnostic accuracy of cystatin C
In order to determine the diagnostic accuracy of cystatin C compared with other markers, we used the day 2 data to construct ROC plots and calculate their AUCs for detecting 51Cr-EDTA clearance <80 and <60 mL/min/1.73 m2 (Figure 2). For detecting 51Cr-EDTA <80 mL/min/1.73 m2, ROC curve analysis revealed an AUC for 1/cystatin C of 0.936, significantly greater than the AUCs for other investigated markers. For detecting 51Cr-EDTA <60 mL/min/1.73 m2, cystatin C also had a significantly higher diagnostic accuracy than serum creatinine, MDRD and C&G. The difference between the AUCs of cystatin C and Ccr did not reach a statistically significant difference (P = 0.812). To describe the characteristics of the analysed parameters, the best diagnostic sensitivity, specificity, positive predictive value and negative predictive value were calculated for detecting 51Cr-EDTA <80 and <60 mL/min/1.73 m2, respectively (Table 2).
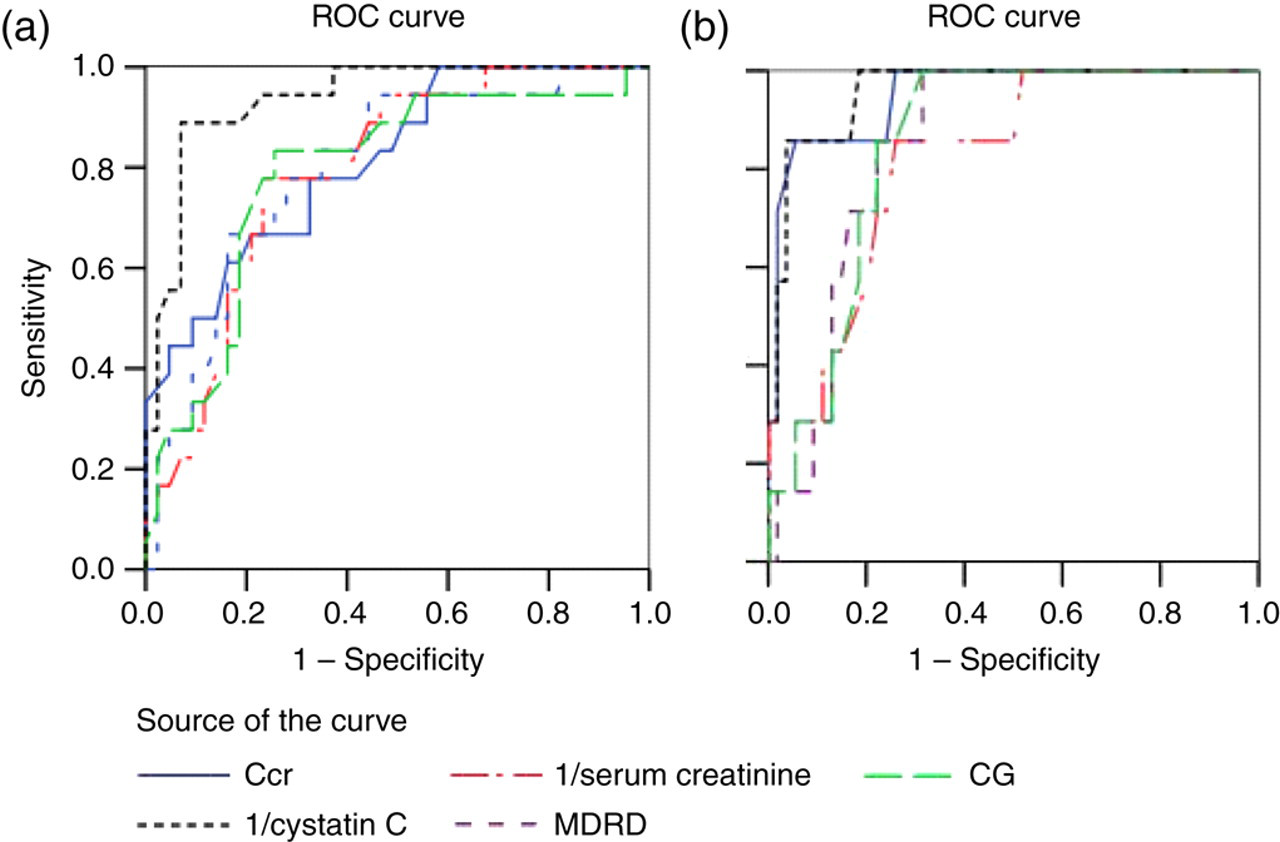
ROC curve analysis of diagnostic accuracy of serum cystatin C, serum creatinine, Ccr, and clearance estimated from the MDRD and Cockroft–Gault equations. The GFR determined with 51Cr-EDTA was used as the reference method. (a): the definition of renal dysfunction was GFR < 80 mL/min/1.73 m2. The AUC for cystatin C (0.936) was statistically significantly different (all P < 0.05) from that of the other markers (0.792 for serum creatinine, 0.812 for Ccr, 0.796 for MDRD and 0.787 for Cockroft–Gault equation, respectively); (b): the definition of renal dysfunction was GFR < 60 mL/min/1.73 m2. The AUC for cystatin C (0.959) was statistically significantly different from the AUCs for serum creatinine (0.820), MDRD (0.837) and Cockroft–Gault (0.851) equations (all P < 0.05), but did not reach statistical significance compared with that for Ccr (0.951) (P = 0.884). ROC, receiver operator characteristic; Ccr, creatinine clearance; MDRD, Modification of Diet in Renal Disease; GFR, glomerular filtration rate; 51Cr-EDTA, 51Cr-ethylenediaminetetraacetic acid; AUC, areas under the curve
The best diagnostic sensitivity, specificity, positive predictive value and negative predictive value calculated for detecting GFR <80 and <60 mL/min/1.73 m2 on day 2
The GFR determined with 51Cr-EDTA was used as the gold standard
PPV, positive predictive; NPV, negative predictive; CI, confidence interval; GFR, glomerular filtration rate; MDRD, modification of diet in renal disease; Ccr, creatinine clearance
Discussion
Postoperative renal impairment is a frequent complication following cardiac surgery and is accompanied by increased morbidity and mortality. 1,21–28 Importantly, even temporal changes in function during the first postoperative week are predictive of long-term mortality. 23,29 In such patients, early knowledge of changes in GFR can help physicians identify patients requiring renal protection. 30–32
All CABG patients included in the current study had preoperative 51Cr-EDTA clearances within the reference range. GFR declined significantly at every time point postoperatively (all P < 0.01 or 0.05), indicating postoperative renal impairment. Serum creatinine was poor at identifying renal dysfunction and tended to overestimate GFR in patients. 3 Although recommended as a supplement to serum creatinine in current guidelines, 7–10 the C&G and MDRD equations significantly deviated from reference GFR measurements in this cohort. Our results suggest that the C&G and MDRD equations allow only crude estimation of renal function, 2,15,33–36 despite correcting serum creatinine for age and gender or weight. The MDRD and C&G equations, like serum creatinine, may be misleading when renal function changes rapidly. Ccr estimation is plagued with preanalytical compliance problems and biological variation of creatinine synthesis and elimination. 3 In many cases in our study, Ccr overestimated GFR, as has been reported by others. 3,37 Hence, these markers are clearly not ideal, each has limitations, and none reflects realtime changes in GFR.
Our data demonstrate the potential usefulness of cystatin C as a test for detecting early changes of GFR in patients after CABG. As described in previous studies, 18,38,39 changes of cystatin C concentration paralleled those of GFR. Of all the available markers, cystatin C had the best correlation with GFR. Cystatin C was more accurate and more sensitively reflected the changes in GFR. 17,40 The accuracy of cystatin C was also illustrated by ROC analysis. For detecting GFR <80 and <60 mL/min/1.73 m2, the diagnostic accuracies of cystatin C were superior to creatinine, even when the C&G and MDRD equations were used. The diagnostic accuracy of cystatin C did not differ significantly from Ccr for detecting GFR <60 mL/min/1.73 m2. A possible explanation for this is that both Ccr and cystatin C accurately reflect renal function at low GFRs, whereas in milder renal function impairment Ccr is not accurate enough to assess transient changes. Diagnostic accuracies of different approaches to GFR assessment vary according to the level of GFR. 13 Cystatin C appears to be a better marker for assessing changes in GFR in CABG patients, even when the changes in GFR are relatively small.
A limitation of our observational study is the relatively small sample size, as reflected in the wide confidence intervals for the sensitivity and specificity estimates. The results therefore need to be confirmed in larger studies.
In conclusion, all data presented here show cystatin C to be capable of detecting small temporary changes of GFR in CABG patients. This may allow earlier identification of patients with increased overall risk and those with a chance of contrast damage.
DECLARATIONS