
Abstract
Introduction
Macroprolactin (MPRL) is an important source of interference that may lead to misdiagnosis and mismanagement of hyperprolactinaemic patients. Prolactin assays exhibit considerable variation in the detection of MPRL. In this study, we examine the requirement for polyethylene glycol (PEG) precipitation in the analysis of hyperprolactinaemia detected by the Advia Centaur as it has a relatively low reactivity with MPRL.
Methods
Four hundreds and sixty-four hyperprolactinaemic samples were collected from the laboratory information system for Saint James University Hospital over a three-year period. These samples were screened for MPRL using PEG precipitation protocol. Monomeric prolactin concentration post-PEG precipitation was compared with a reference range determined by PEG precipitation in normal subjects.
Results
MPRL was the cause of hyperprolactinaemia in 4% of patients (16/409) over the three-year period studied. Nine subjects with MPRL also had elevated monomeric prolactin.
Conclusions
PEG screening is still needed for assays with low MPRL reactivity such as the Advia Centaur and this should be performed with a locally derived reference range for monomeric prolactin.
Introduction
Macroprolactin (MPRL) is a high molecular mass prolactin complex of prolactin bound to an immunoglobulin molecule. This large complex has delayed clearance leading to increased circulating concentrations. 1 The MPRL complex is detected variably by immunoassay systems presumably due to the physical protection by the immunoglobulin of the epitope on the prolactin which is recognized by the diagnostic antibody. 2 This results in considerable variation in the detection of MPRL by different assay systems. However, since MPRL is thought to be physiologically inactive, a failure by some systems to detect it may not be harmful. The opposite is not true; detection of MPRL offers the prospect of cascading a range of potentially inappropriate testing. 3 Since all immunoassays for prolactin detect MPRL to an extent, it is widely recommended that all laboratories perform a screening test for MPRL on all serum samples with elevated prolactin. Polyethylene glycol (PEG) precipitation is considered the best screening test to use. 4 We have used this protocol in our routine laboratory and report on our experience over three years.
Methods
MRPL screening protocol
Samples with prolactin greater than 700 mIU/L were cascaded for MPRL screening; the upper reference limit is 600 mIU/L (manufacturer's data) and the figure of 700 mIU/L was chosen arbitrarily. This involved measuring prolactin before and after PEG precipitation. Recovery of >60% excluded significant MPRL and recoveries of ≤40% were typically consistent with the presence of substantial amounts of high molecular weight forms. 5 Values between 40% and 60% were classified as indeterminate and were referred for gel filtration chromatography (GFC). In the presence of MPRL, a monomeric prolactin concentration was calculated.
Assay methods
All serum samples were stored at −20°C prior to analysis. PEG precipitation was performed using the protocol described by Suliman et al. 3 A volume of 250 μL of sera was mixed with an equal volume of 25% (w/v) of PEG 6000 (BDH, Poole, England) or prolactin free-assay diluent (Siemens Healthcare Diagnostics Ltd, Camberley, Surrey, UK). The PEG 25% stock was stored at 4°C for no more than two weeks. All prolactin measurements were performed on the Advia Centaur according to the manufacturer's protocol (Siemens Healthcare Diagnostics Ltd). This was calibrated against the World Health Organization (WHO) third international standard IS 84/500 and had an inter-assay % coefficient of variation (%CV) of 5%. Paired pre- and post-PEG prolactin were measured in the same batch.
Reference subjects
Serum samples from primary care specimens were collected for the establishment of a reference interval for monomeric prolactin. The criteria for selection were (i) that the prolactin value was within the reference interval, i.e. ≤600 mIU/L; (ii) there were no previous analyses from endocrinology, gynaecology or psychiatry clinics; (iii) the subjects were euthyroid and (iv) the subjects were not taking any medication known to elevate prolactin or were not pregnant (data from request cards). Samples were collected over a period of three months and were anonymized prior to analysis.
Patient data
Patient data on MPRL were collected retrospectively from the laboratory information system for Saint James University Hospital (population served – 400,000 approximately) for the period September 2005 to September 2008 inclusive. Data were collected on all patients with prolactin ≥700 mIU/L and included age, gender and all prolactin results (total prolactin before and after PEG, GFC analysis if performed and calculated monomeric prolactin).
Statistical analysis
The monomeric prolactin 95% reference intervals were calculated using log transformed parametric data with the Analyse-it add-in package (version 2.10) for Microsoft Excel (Analyse-it, Leeds, UK,
Results
Monomeric prolactin reference interval
The reference population initially consisted of 128 subjects but three subjects were excluded: one had a PEG recovery of 31% and two subjects had concentrations >3 standard deviation (SD) from the group mean of 202 mIU/L. The final panel consisted of 111 women and 14 men, and a median age of 45 y (range 19–72). A total of 125 samples were subjected to PEG precipitation. Median prolactin recovery was 98% (range 70–115) (see Figure 1). Total and post-PEG PRL distribution was non-Gaussian; both distributions were normalized by log transformation. Because the proportion of men in the reference population was small (11%), we used the female data to derive a female reference interval. This gave 95% reference intervals of 74–413 mIU/L (Table 1).
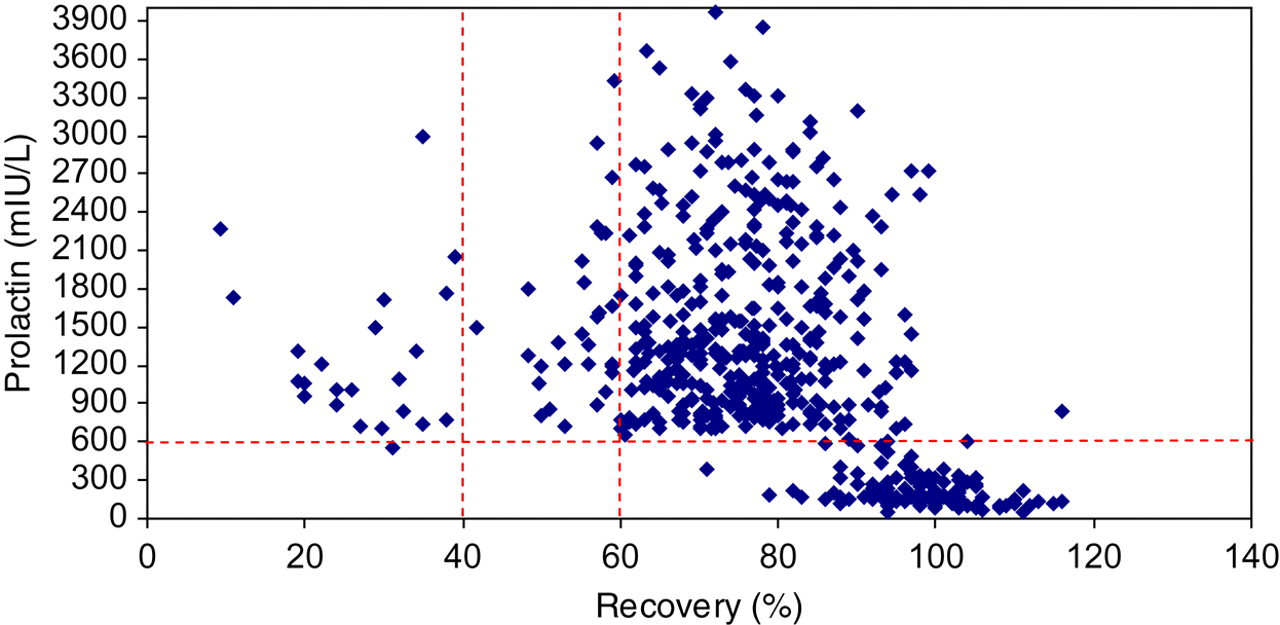
The relationship between prolactin concentration and recovery after the addition of polyethylene glycol (PEG). The top right-hand corner of the graph represents the recovery of 464 hyperprolactinaemic samples (prolactin >700 mIU/L) after PEG precipitation as determined by Advia Centaur. The bottom right-hand corner represents the recovery of 125 samples used to derive the monomeric prolactin reference interval as determined by Advia Centaur
Reference intervals for total prolactin and post-PEG prolactin (mIU/L) for Advia Centaur
PEG, polyethylene glycol
Patient evaluation
Four hundred and sixty-four samples were studied (Figure 1). These were from 409 subjects, 315 women, aged 36 (17–86) y (median, range) and 94 men, aged 45 (17–96) y (median, range). Prolactin values ranged from 700 to 13,330 mIU/L (median 1516 mIU/L). Fifty-five subjects had duplicate samples. The mean difference of the duplicates was 160 mIU/L and SD of the difference 825 mIU/L (range −665 to 985) (no clinical data were available to explain this variation). Only the first sample per person was included in this analysis. Five duplicates out of 55 subjects were positive for MPRL; in all cases the presence of MPRL was consistent within individuals.
Out of 409 subjects, 354 had a recovery >60%. All subjects in this group had a high recovery due to raised monomeric prolactin. Twenty-one (5.3%) subjects had a prolactin recovery of <40%. Table 2 shows the data for 21 subjects with recovery <40%; 5/21 hyperprolactinaemic subjects had raised monomeric prolactin in addition to MPRL. Thirty-four subjects (8.3%) had recovery ranging from 40% to 60%; 22/34 (65%) were referred for GFC analysis (Table 3). Out of 34, 12 had recovery of 57–59%; repeat samples were requested and had recovery >60%.
Discordant classification of 21 patient with post-PEG recovery <40%
H, hyperprolactinaemia and M, macroprolactinaemia, based on monomeric prolactin reference interval derived by Beltran et al. and this study (mIU/L). PEG, polyethylene glycol
Relationship between post-PEG recovery and presence of raised monomeric prolactin
PEG, polyethylene glycol
Only 4/22 subjects with intermediate PEG precipitation showed evidence of MPRL on GFC. Three of these subjects showed MPRL and one subject had big prolactin (M r 40–60 kDa) as the predominant form of prolactin. However, all four of subjects positive for MPRL also had elevated monomeric prolactin (referral lab reference range >415 mIU/L).
In our laboratory, the prevalence of raised prolactin due to MPRL only was 4% over the three-year period. The majority of the workload for prolactin measurement comes from the general practitioner (37%), psychiatry (25%), and hospital outpatient clinics (23%) (including endocrinology, gynaecology and reproductive units).
Discussion
It is evident that a clinical suspicion alone is not a satisfactory approach to indicate the presence of MPRL in patients with hyperprolactinaemia. MPRL is a heterogeneous molecule due to complexes with IgG, IgA, non-IgG containing MPRL and glycosylated MPRL. 6 The heterogeneity of this molecule, in addition to the various formulations for prolactin assays, and the different antibodies population utilized for different prolactin methods are contributing factors to the variable detection rate of MPRL. The use of PEG precipitation as a screening test is based on its ease of performance and cost-effectiveness even for assays with relatively low cross-reactivity. 7 We have found that 4% of hyperprolactinaemic samples measured by the Advia Centaur were due to MPRL and this is similar to the 5% figure previously reported. 8 This is low in comparison to methods such as Tosoh AIA and Wallac DELFIA, which have rates of 24% and 15% respectively. 5,8,9
Reporting monomeric prolactin alongside the result for MPRL is a way to improve the clinical service and to prevent missing cases where hyperprolactinaemia and MPRL co-exist in a patient serum. 10 Monomeric prolactin is the prolactin concentration determined after PEG precipitation, but because of the partial and non-specific precipitation of monomeric prolactin by PEG, this should be compared with a reference range determined by PEG precipitation in normal subjects. 10 Our study illustrates the importance of reporting monomeric prolactin since nine subjects with MPRL also had an elevated monomeric prolactin. Although the dual occurrence of macro- and monomeric prolactin is rare, it is likely that reporting only the presence of MPRL would have led to incomplete or even inappropriate therapy for these subjects.
The definition of increased monomeric prolactin is difficult since we have shown a different reference range for monomeric prolactin than Beltran et al. 11 who also used the Advia Centaur with the same PEG protocol, calibrated against same standard (IS 84/500). The upper limit of female reference interval derived from this study was considerably higher at 32% more than that reported by Beltran et al. We compared the classification of macroprolactinaemic patients using percentage recovery post-PEG to monomeric reference intervals. This resulted in a significant change in the diagnostic classification depending on which reference interval is used. Leeds reference interval classified five cases as hyperprolactinaemia whereas 10 cases would have been so diagnosed by the reference interval of Beltran et al.
It is likely that the discrepancy is related to the reference populations. 12 In our study, reference samples were selected from serum samples that were sent to the laboratory for prolactin measurements, whereas Beltran et al. used ‘healthy health-care professionals’ to derive their monomeric prolactin ranges. A further possible explanation for this discrepancy may be the high recovery that has been seen in our reference population which may be concentration dependent. The prolactin concentration in the control group did not exceed 600 mIU/L with a mean of 202 mIU/L. Beltran et al. reported a recovery of 88% for Advia Centaur for a concentration of 700 mIU/L.
PEG has a non-specific ability to alter protein solubility due to steric and water exclusion effects and therefore has variable effects as a protein precipitant. 13 This non-specific effect is a major limitation of the technique. We have shown that PEG precipitates immunoglobulins differentially. The 25% w/v PEG protocol precipitates almost all IgG and IgM but only 50% IgA (unpublished data). In view of this, PEG precipitation can be recommended as a screening test for high molecular weigh forms of prolactin since there are both false-positive and -negative cases. False-positive cases have been reported in cases with raised immunoglobulins 14 and false-negative is likely to occur in cases of IgA containing MPRL. 15
In conclusion, we confirm that assessment of MPRL by such methods as PEG precipitation is still needed for prolactin assays with relatively low cross-reactivity with MPRL such as the Advia Centaur. Reporting monomeric prolactin in addition to MPRL status may detect cases where raised monomeric prolactin co-exists with MPRL. This step requires the development of specific reference intervals for monomeric prolactin. Moreover, we suggest that the reference interval for monomeric prolactin is not transferable across laboratories even when the same analytical method is used due to population differences.
DECLARATIONS