
Abstract
Lymphoplasmacytic lymphoma (Waldenstrom's macroglobulinaemia) is a low-grade small-cell lymphoma that produces monoclonal IgM. Usually, clinical features are related to growth of the tumour and include weakness and fatigue, an increased bleeding tendency, and neurological and visual disturbances. We present a case of lymphoplasmacytic lymphoma with type I cryoglobulinaemia that presented with clinical symptoms associated with hyperviscosity syndrome. Quantitation of the paraprotein was not possible using conventional serum protein electrophoresis due to the high serum viscosity, and therefore monitoring was carried out using serial serum free light chain measurements.
Introduction
Lymphoplasmacytic lymphoma (Waldenstrom's macroglobulinaemia) 1 is a rare disease with a median age of presentation of 63 y. It consists of a neoplasm of small B lymphocytes, plasmacytoid lymphocytes and plasma cells with infiltrates commonly involving the bone marrow, lymph nodes and spleen. Most patients demonstrate a serum IgM paraprotein with consequent symptoms of hyperviscosity. The paraprotein may also have autoantibody or cryoglobulin activity. 2 In patients with lymphoplasmacytic lymphoma, accurate measurement of serum IgM concentration is vital both at diagnosis and in order to monitor response to therapy. Since immunochemical quantitation of the paraprotein is unreliable, 3 it is recommended that quantitation is carried out by serum protein electrophoresis followed by densitometry. 4
We present here a patient with lymphoplasmacytic lymphoma, in whom the IgM paraprotein could not be quantitated using serum protein electrophoresis, and therefore monitoring was carried out using serial serum free light chain (FLC) analysis. Although the value of serum FLC measurements in Waldenstrom's macroglobulinaemia has previously been recognized as both a prognostic marker and a reflection of tumour burden, 5–7 we are unaware of any reports where they have been measured in patients with cryoglobulinaemia.
Case report
An 82-year-old gentleman with stage 3 CKD and diabetes was referred from his general practitioner (GP) to the haematology day unit to the Victoria Hospital, Kirkcaldy in view of the results of routine investigations. These revealed he was markedly anaemic with a haemoglobin of 8.9 g/dL, had a grossly elevated plasma viscosity of 15 cp and a total serum protein of 102 g/L. Serum protein electrophoresis revealed the presence of an IgM lambda paraprotein, which could not be quantitated since it precipitated out on the gel (Figure 1) even when applied directly post incubation at 37°C (Figure 2). Furthermore, the serum sample appeared clotted after overnight storage at both 4°C and room temperature, and this clotting process was reversed once the sample was warmed to 37°C.
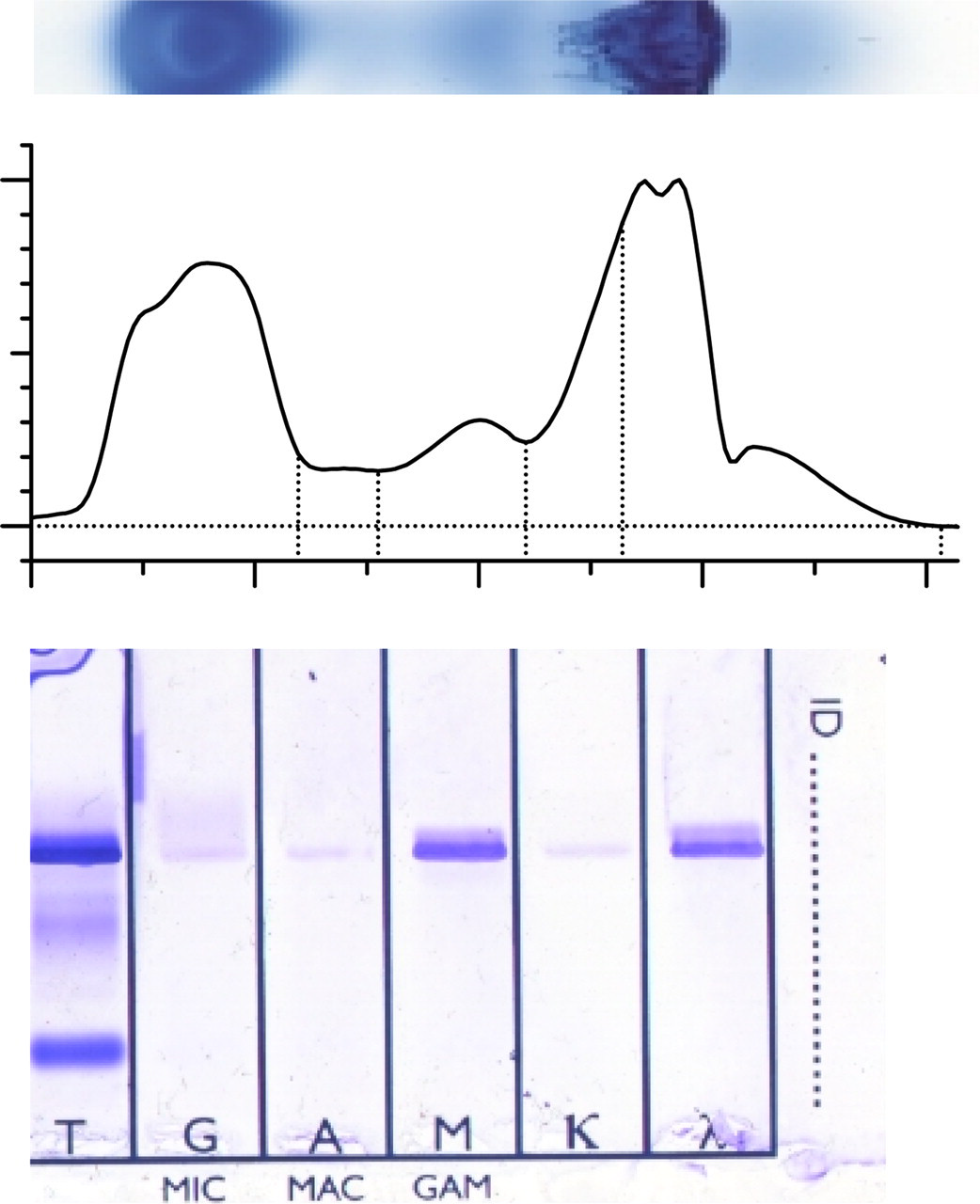
Serum protein electrophoresis and immunofixation on samples at room temperature
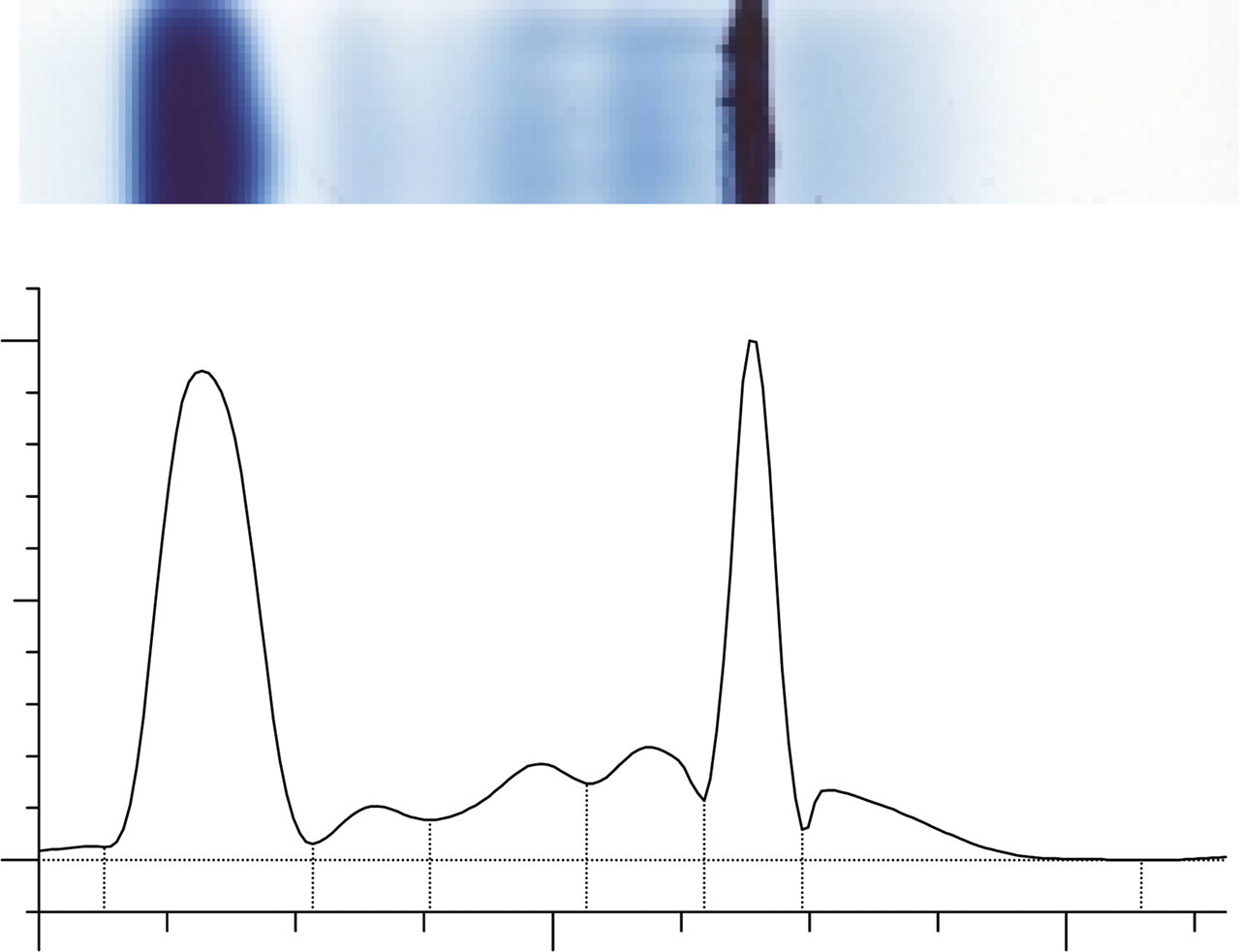
Serum protein electrophoresis on a sample at 37°C
Upon questioning, he displayed clinical symptoms in keeping with hyperviscosity syndrome, including dyspnoea, epistaxis, blurring of vision and sensory neuropathy. Plasma exchange was subsequently carried out to alleviate his symptoms. The diagnosis was expected to be lymphoplasmacytic lymphoma, although an extremely rare case of IgM myeloma could not be excluded at this stage. A bone marrow aspirate was inconclusive; however, the trephine biopsy both morphologically and with immunohistochemistry confirmed the diagnosis as lymphoplasmacytic lymphoma. Subsequent investigations revealed his urine was positive for Bence Jones Protein and cryoglobulin analysis indicated this was a type I cryoglobulinaemia. The patient was commenced on chemotherapy and since we were unable to monitor his response to treatment using conventional protein electrophoresis, serial serum FLC analysis was used instead. Table 1 shows the patients baseline serum FLC results and those post commencing chemotherapy.
Serum free light chain (FLC) results pre- and postcommencement of chemotherapy. Reference intervals are shown in parentheses
Discussion
Cryoglobulins are serum proteins that reversibly precipitate at temperatures below 37°C. Type I cryoglobulinaemia accounts for 10% of all cryoglobulins, and consists of monoclonal immunoglobulins associated with immunoproliferative disorders that can result in symptoms of hyperviscosity and thrombosis. 8 High concentrations of monoclonal components tend to precipitate at higher temperatures, and in our patient precipitation occurred at room temperature. Due to the high concentration of the M protein, quantitation was not possible using serum protein electrophoresis as the sample precipitated on the gel even when applied at 37°C. Monitoring was therefore carried out by measuring serum FLC that do not cryoprecipitate. This case highlights the benefits of the use of the serum FLC assay in situations where serum protein electrophoresis cannot be used for M protein quantification.
DECLARATIONS