
Abstract
Background
It has been suggested that for the accurate measurement of calcium in urine, samples must be collected into bottles containing acid. Acidification poses risks to both patients and laboratory staff. Here we reappraise whether acidification is a preanalytical necessity.
Methods
Twenty-four-hour urine samples were collected from 133 patients into bottles without acid or preservatives. In a subset of 29 patients, 10 mL aliquots were prepared to test the effect on urine calcium of 0.1, 1.0 and 5.0 mol/L hydrochloric acid (HCl). Calcium was then measured immediately after acidification, after 12 h and seven days storage at 4°C. In a separate study, urine calcium concentrations in paired control (non-acidified) and acidified (with 5 mol/L HCl) samples were compared in 133 patients. When available, we recorded the time from start of urine collection to time of analysis. Calcium was measured using the cresolphthalein complexone colorimetric endpoint assay on the Roche Modular system.
Results
There was no significant difference in the calcium concentration in the 29 cases studied between the varying acid concentrations tested compared with non-acidified urine (P = 0.987). Overall, in 133 patients there was no difference between control and acidified samples (P = 0.888). We found no correlation between basal urine pH and urine calcium at all time points studied.
Conclusions
Our results suggest that the acidification of urine samples is not a preanalytical necessity for the measurement of urine calcium.
Introduction
Urinalysis is an important part of the clinical laboratory's test repertoire. Unlike other sample types, urine has problems that require special preanalytical considerations. For example, it is important to ensure that patients complete a 24-h collection and a urine creatinine concentration may be used to check this. 1 Analytes such as uric acid require collection of urine in alkali, 2 whereas catecholamines require collection into bottles containing acid to prevent oxidation at neutral pH. 3 Other analytes like phosphate and calcium are affected by food intake and therefore show great variability throughout the day; therefore 24-h collections are recommended. 1 Calcium and magnesium may precipitate by complexing with anions such as phosphate during collection and require either collection in an acid medium to keep the solutes in solution or acidification after collection to re-dissolve precipitated solutes. 1,4
The 24-h urine calcium concentration is used to evaluate calcium and phosphate metabolism and excretion, and to monitor calcium or phosphate replacement. 5 It is therefore a useful test in the management of patients with osteoporosis, renal stone disease and familial benign hypocalciuric hypercalcaemia. 1,6
For the accurate analyses of calcium, it has been suggested that urine must be collected in a bottle containing acid.
1,4
The collection of urine in a container with acid is not without its problems. There have been reports of patients burning their skin, corroding their furniture after accidently pouring out the acid and there have been patients, who have mistakenly poured out the acid assuming that it was either residue or condensate. Given these problems, we undertook a study to assess whether the acidification of urine for the measurement of calcium specifically is a preanalytical necessity. We sought to answer the following questions:
(A) Is there a concentration-dependent effect of the hydrochloric acid (HCl) used on measured urine calcium? (B) Is there a difference in urine calcium after acidification within the laboratory compared with non-acidified urine? (C) Is the analyte stable when stored for 12 h or seven days at 4°C (these times are relevant for clinical laboratory practice as they reflect delay in processing and short-term storage, respectively)? (D) Does the basal urine pH affect urine calcium concentration?
Methods
We had local ethical approval for this study as work carried out as part of assay development and service provision. We collected 24-h urine samples from 133 patients who attended our metabolic bone clinic or ward, into bottles with no acid or preservatives. In an initial subset of 29 patients, after thoroughly mixing the bottle(s), four 10 mL aliquots were prepared: one with no acid; another three with 100 μL 0.1, 1.0 and 5.0 mol/L HCl, respectively. To test whether there were any time-dependent effects on the concentration of the measured urine calcium, analyses were undertaken immediately after acidification, after 12 h and seven days storage at 4°C. In all cases, there were no visible precipitates observed at the bottom of the collection bottles or in the test tube. We also measured the pH in urines of 29 patients in order to assess whether there was any correlation with the urine calcium concentration over the three time points studied. The pH was measured with a Hanna pH meter (Hanna Instruments, Woonsocket, RI, USA).
In a separate study consisting of 133 patients, which included the above 29 patients, we compared the urine calcium in paired samples that were acidified with 5 mol/L HCl and their non-acidified controls. In this particular study, we recorded the time from the start of urine collection as recorded on the bottle to the time of analysis as ascertained from the automated analyser. In all cases, the bottle(s) were thoroughly mixed prior to taking aliquots.
Calcium was measured using the cresolphthalein complexone colorimetric endpoint assay on the Roche Modular system (Roche Diagnostics Limited, Burgess Hill, West Sussex, UK). All internal and external quality assurance results were deemed acceptable as per defined criteria during the entire study.
Using the Kolmogorov–Smirnov test, our data were found to be non-normal and we therefore used Kruskal–Wallis test to compare differences in urine calcium across the various acid concentrations tested (0–5.0 mol/L) and Mann-Whitney U test to compare the control (non-acidified) versus acidified samples. All analyses were undertaken using SigmaPlot version 11.0 (Systat Software Inc, Hounslow, London, UK) and figures were prepared using Origin version 6.0 (GE Healthcare UK Ltd, Little Chalfont, Buckinghamshire, UK).
Results
(A) Is there is a concentration-dependent effect of the acid used on urine calcium concentration?
As shown in Figure 1, there was wide variation in the basal urine calcium concentrations in the patients studied with a range of 0.2–4.0 mmol/L; however, there was no difference in the measured calcium concentration across all concentrations of HCl tested compared with the non-acidified (basal) sample (P = 0.987).
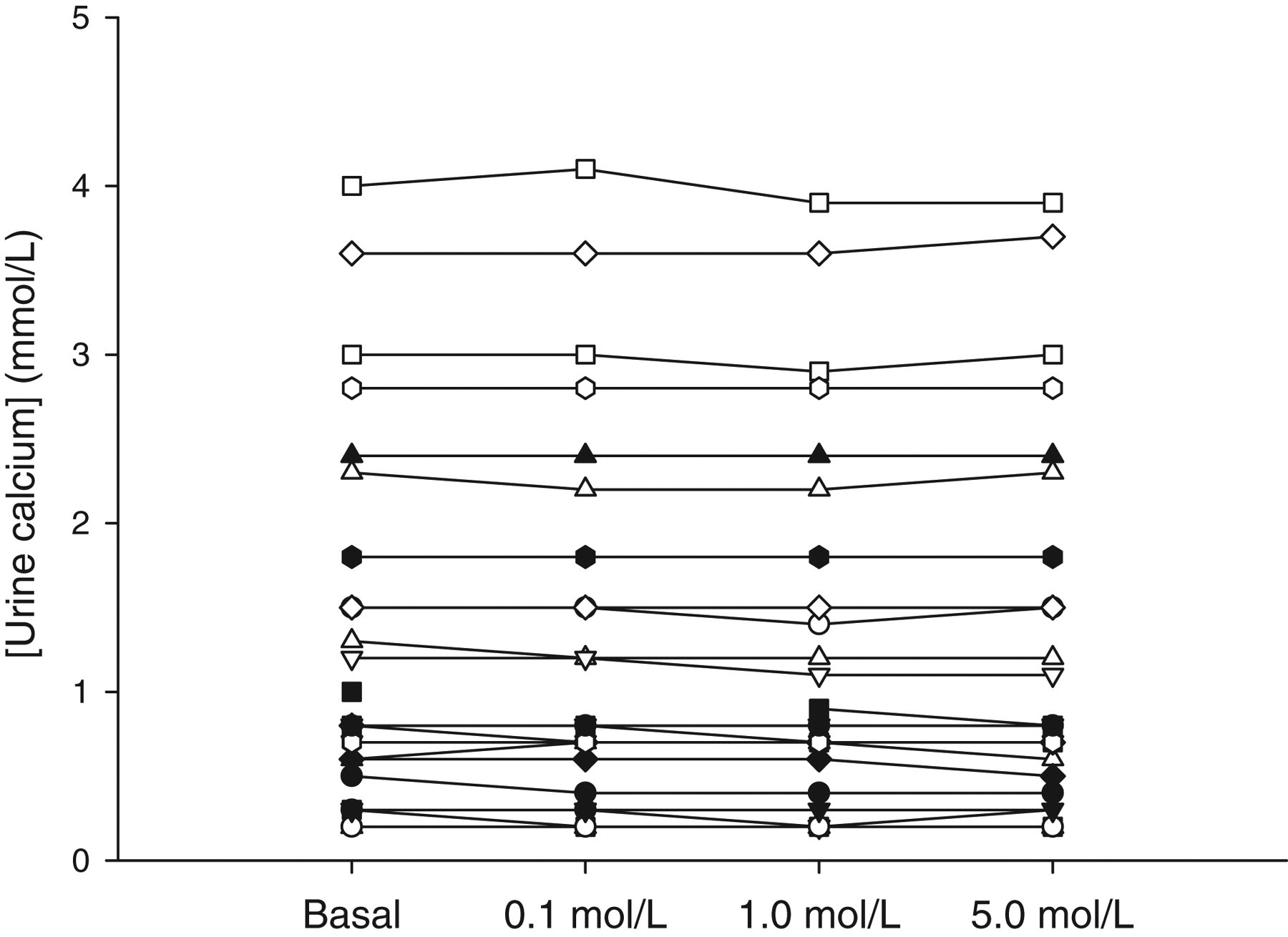
Urine calcium concentration in 29 patients tested with 0.1, 1.0, 5.0 mol/L hydrochloric acid (HCl) compared with basal, untreated urine
(B) Is there a difference in urine calcium after acidification within the laboratory compared with non-acidified urine?
There was no significant difference in urine calcium concentrations between control (non-acidified) and acidified urine samples as shown in Figure 2 (P = 0.888). The average time from the start of urine collection to the time of analysis was 30.5 h (median = 30 h, standard deviation [SD] = 4.87) and 32.3 h (median = 32 h, SD = 4.73) for the control and acidified urine samples, respectively. The start time of collection was available in approximately 62% of patients.
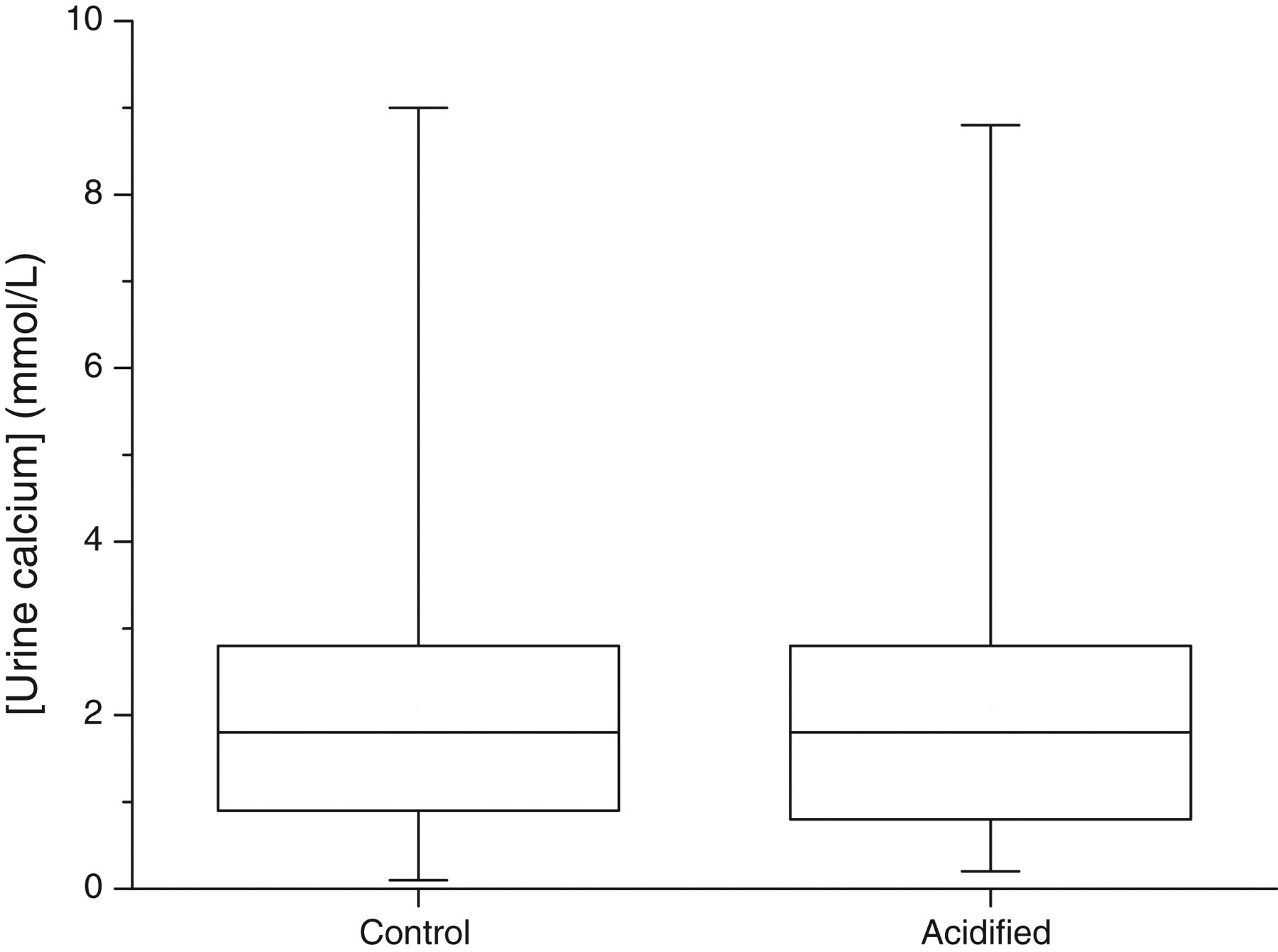
Box–whisker plots comparing urine calcium in paired control and acidified (with 5 mol/L HCl) samples. The horizontal line through each box is the median value, the upper hinge is the 75th percentile and the lower hinge is the 25th percentile. The whiskers represent the full range of the data
(C) Is the analyte stable after 12 h or when stored for 7 days at 4°C?
As shown in the difference plots in Figure 3, in comparison with the non-acidified (basal) urine calcium concentration, the change in the measured calcium concentration was within 2 SDs of the mean in most of the samples either with no acid treatment (Figure 3a) or after treatment with 0.1 mol/L (Figure 3b), 1.0 mol/L (Figure 3c) and 5.0 mol/L (Figure 3d) HCl at 12 h (filled circles) and seven days (open circles) storage at 4°C. However, eight patients (some with multiple data points) showed differences greater than or less than 2 SDs in the measured urine calcium concentration. With 5 mol/L HCl the differences in the urine concentration was close to or within 2 SDs of the mean (Figure 3d).
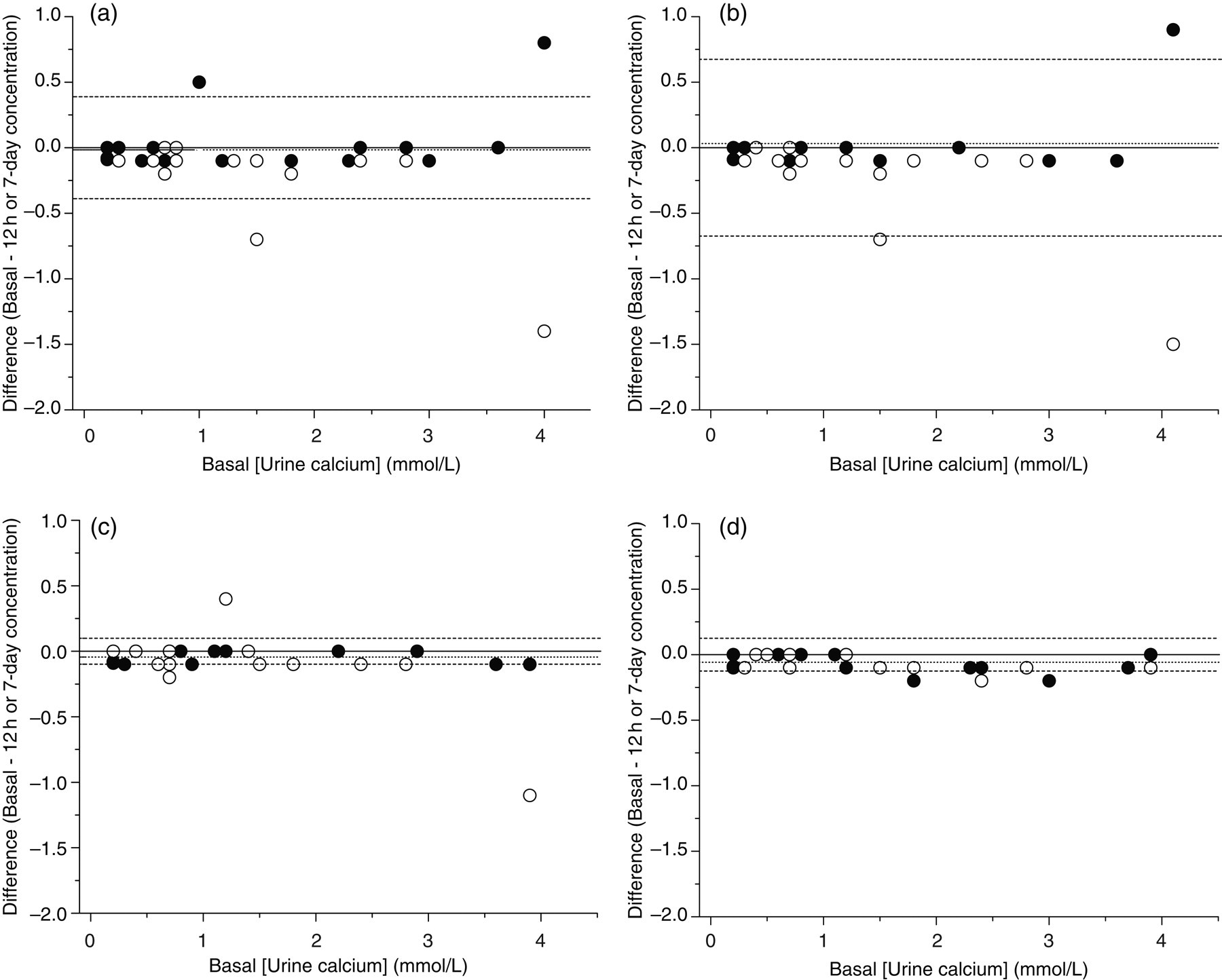
Difference plots of urinary calcium concentrations between basal and 12-h concentrations (filled circles), or seven-day concentrations (open circles) at basal pH (a), and with 0.1 mol/L (b), 1 mol/L (c) and 5 mol/L HCl (d). The solid lines denote zero bias, the dotted lines denote mean difference and the dashed lines are ±2 standard deviations of the difference
(D) Does the basal urine pH affect urine calcium?
The mean basal urine pH in the subset of 29 patients was 6.54 (SD = 0.71) and varied between 4.46 and 7.81. We found no correlation between basal urine pH and urine calcium concentration measured immediately after acidification (r = −0.04), after 12 h (r = 0.01) and after seven days (r = −0.09) storage at 4°C.
Discussion
Although it has been suggested that acidification re-solubilizes calcium, we found no significant differences between calcium concentrations before or after acidification when the urine calcium was measured on the day of sample receipt. It is difficult to assess whether a patient's urine sample is liable to contain precipitated calcium, therefore it has been suggested that to prevent any potential error it would be necessary to acidify all urine samples. 1 However, taken together our data do not support the idea that acidification is a preanalytical prerequisite. As shown in Figure 2, there was no significant difference in the urine calcium concentration between control and acidified samples.
Regarding storage, we chose to study two time points, that is, 12 h and seven days as they reflect delay in processing and short-term storage, respectively, in a typical clinical laboratory setting. In eight cases there were differences greater than or less than 2 SDs in the measured urine calcium concentration at these time points and at different acid concentrations tested when stored at 4°C (Figure 3). In addition, we found that with 5 mol/L HCl the differences in the urine concentration was for the most part within 2 SDs of the mean (Figure 3d). If storage or delay in sample processing is an issue, then it may be necessary to acidify urine samples on receipt in the laboratory for calcium determination with 5 mol/L HCl. However, further work is required to confirm this observation. This was also the basis for the choice of using only 5 mol/L HCl in the larger study with 133 patients.
Previously, we have shown that although acidification or the lack of it affects the accuracy of urine calcium measurement, it did not have a significant clinical impact because the changes were not large enough to exceed the critical threshold, which takes into account the biological and analytical variability. 7 The findings of the present study are also consistent with another report that showed, among other analytes that were studied, that there was no difference in the measured urine calcium concentration after acidification in promptly assayed 24-h urine collections even after heat treatment. 8
Factors such as the urine citrate concentration may have an important role in determining whether urinary calcium precipitates and thus affects the final calcium concentration in urine, 9 but it was beyond the scope of the present study to examine this. Future studies may wish to explore the determinant factors, the nidus for precipitation and therefore the final urine calcium concentration.
In view of the risks to patient and laboratory staff safety posed by the acidification of urine samples and as shown by our data, we suggest that the acidification of urine samples for calcium measurement may not be necessary. However, storage may give inaccurate results in some cases. Furthermore, it is appreciated that for some analytes such as catecholamines and 5-hydroxyindoleacetic acid the need for collection into bottles containing acid is imperative due to their in vitro instability 3 ; however, these are less commonly requested tests.
In conclusion, our results suggest that the acidification of urine samples is not a preanalytical necessity for the measurement of urine calcium.
DECLARATIONS