
Abstract
We describe a patient being investigated for anaemia where the lipaemia index on a Beckman Coulter DxC800 analyser was markedly elevated and out of keeping with the visual appearance of the serum. Subsequent investigation revealed a monoclonal IgM kappa immunoglobulin with type I cryoglobulin behaviour. The patient was then diagnosed with a non-Hodgkin B-cell lymphoma. We later identified a second patient with a similar anomalous index with an IgM lambda paraprotein, and a known marginal zone splenic lymphoma but were unable to confirm cryoglobulin behaviour prior to treatment. A review of 50 consecutive IgM paraproteins revealed no other anomalous lipaemia indices. We postulate that it is the properties of the paraprotein that determine its cryoglobulin behaviour that also render it susceptible to precipitation in the index diluent, not the fact of it being an IgM paraprotein
Introduction
A feature of most modern biochemical analysers is that they devote one channel to a simple dilution of serum in an aqueous medium that is then monitored at a variety of wavelengths to provide semi-quantitative estimates of haemolysis, lipaemia and icterus.
Monoclonal immunoglobulins (paraproteins) have been described as causing interference in many direct assays (defined as those not requiring prior protein removal by precipitation or other means), most commonly phosphate but also with a wide range of other analytes. 1–6 The paraproteins are usually of the IgM class but interference can also occur with IgG, and IgA classes and with an increase in polyclonal IgG concentration. Mostly the interference is caused by precipitation of the paraprotein giving rise to an increased turbidity of the sample and a positive interference in photometric assays, although the mechanism can be more complicated than this and may give rise to a negative interference, such as that observed in HDL-cholesterol assays. 2
We now describe a case of an IgM paraproteinaemia that was unmasked due to the observation of a high lipaemia index that was inappropriate for the clear appearance of the serum.
Case report
Blood from a 69-yr-old lady, being investigated for suspected anaemia, was received for a full blood count, and Na, K, creatinine and ferritin analysis. Along with analyses for Na, K and creatinine, indices for haemolysis, lipaemia and icterus were also routinely measured (DxC analyser, Beckman Coulter UK Ltd, High Wycombe, UK). These indices are produced by diluting 14
Following a discussion of these findings with the GP, the patient was referred to a consultant haematologist. A 5–6-month history of drenching sweats occurring both at night and during the day, coupled with a slight loss of weight, was elicited. Blood was taken with precautions appropriate for cryoglobulin studies and a bone marrow examination was performed. The bone marrow revealed an excess of plasma cells, with 60% being positive for a kappa light chain, <1% for a lambda light chain and surface markers showing a preponderance of CD19-positive cells, indicative of a B-cell non-Hodgkins lymphoma (NHL).
Serum kept at 37°C remained totally clear, whereas that placed at 4°C rapidly became cloudy. Centrifugation at 4°C caused complete separation into two layers, the supernatant resembling the clear serum while the infranatant was a colourless and clear liquid (Figure 1). The 4°C supernatant was separated from the infranatant, which was then washed three times with cold saline. After the final washing, saline was added to the infranatant to restore the volume to that of the original whole serum sample and then the solution warmed to 37°C. Electrophoresis showed a paraprotein band in the 37°C sample (concentration 14 g/L), which was absent in the 4°C supernatant, and present in isolation in the reconstituted infranatant (Figure 2). Immunofixation confirmed that the bands were of IgM kappa class and that indeed there was no other protein besides the monoclonal IgM in the infranatant (not shown), thus confirming this to be a type 1 cryoglobulin.
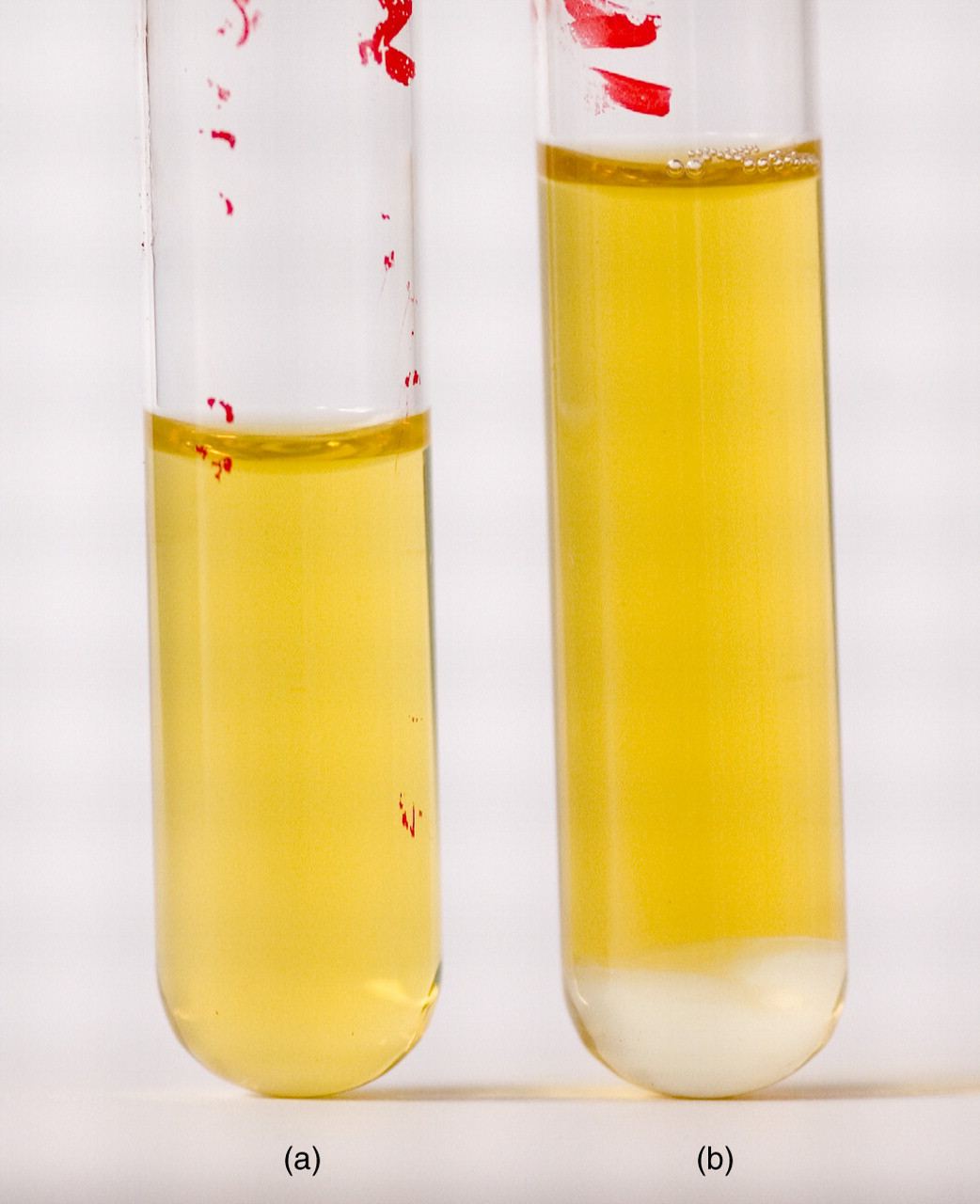
Tubes showing serum kept at 37°C (a) and tube with serum kept at 4°C after centrifugation (b). Tube b shows two distinct fluid layers: the upper (supernatant) indistinguishable from serum, the lower (infranatant) being clear and colourless
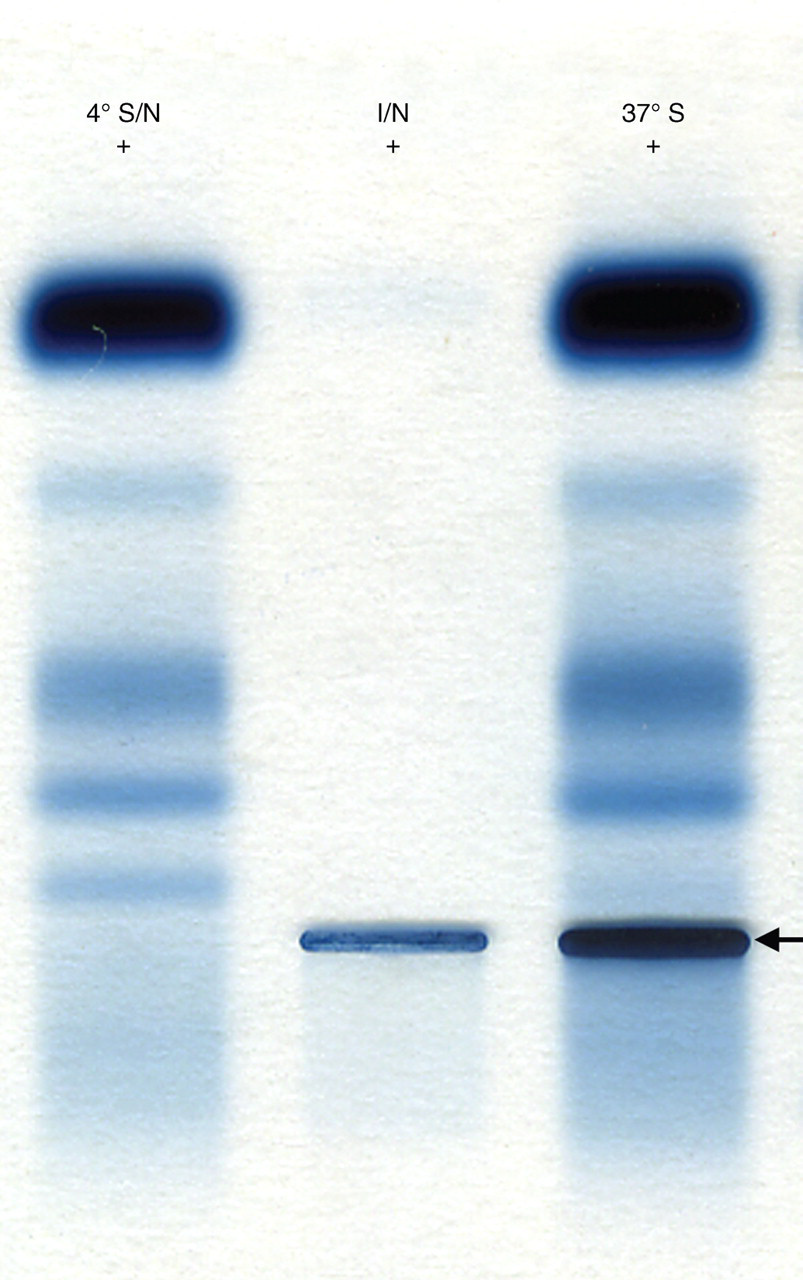
Electrophoresis of supernatant serum after storage at 4°C and centrifugation (Lane 1: ‘4°S/N’): reconstituted infranatant (now at 37°C) after storage of whole serum at 4°C, centrifugation, removal of supernatant and washing of infranatant (Lane 2: ‘I/N’) and whole serum kept at 37°C (Lane 3: ‘37°C’). The IgM kappa paraprotein (arrow) is clearly visible in lanes 2 and 3 but not 1. +Indicates the anode
All three samples, together with a patient serum that yielded a lipaemia index of 0, were diluted in index diluent from the analyser at 37°C in 5 mL plastic tubes in the same sample to total volume ratios as those used in the analyser. The solutions containing the control serum and the 4°C supernatant remained clear, while those containing the sample kept at 37°C and reconstituted infranatant warmed to 37°C immediately became cloudy, thus supporting the hypothesis that it was the paraprotein that had been responsible for the elevated lipaemia index.
The patient was treated with six cycles of chlorambucil and prednisolone. The paraprotein concentration in a sample collected with precautions appropriate to a cryoglobulin was reduced to 3 g/L, the patient's symptoms improved and the lipaemia and icterus indices reduced to zero.
Subsequently, a second patient was identified with indices also inappropriately high for the appearance of the serum (lipaemia index 8, icterus index 6 [corresponding to a bilirubin concentration between 128
A retrospective review of lipaemia indices on 50 consecutive patients presenting with an IgM paraprotein over a 6-month period showed that two had indices of 1 and 48 of zero. These patients were either newly presenting or were being monitored with or without treatment. The range of paraprotein concentrations was from 1 to 94 g/L (median 9 g/L). Ten had concentrations of 15 g/L or over. One patient had a paraprotein that was known to behave as a cryoglobulin (22 g/L) that had an appropriate lipaemia index. We have not so far been able to identify other patients with a type I cryoglobulin and test the serum indices.
Discussion
The interference of paraproteins on standard biochemical measurements has been known about for many years and has been the subject of a recent exhaustive review. 1 In general, the paraprotein precipitates on interaction with the reagent thus causing turbidity and influencing the photometric reading. Dependent upon whether the turbidity occurs at the blanking stage, or after addition of subsequent reagents, interference may be positive or negative. The factors responsible for the precipitation are complex and depend on the pI of the paraprotein, and the pH, ionic strength and chemical composition of the reagent solution. In this case, the diluent was a Tris–HCl buffer with added benzyl alcohol. It is possible that the benzyl alcohol is the agent responsible for precipitation. Without stored serum from the time of the initial studies prior to treatment of the patient we are unable to test this hypothesis and therefore whether the Beckman system is more prone to interference on the indices channel than are other analysers. We believe this to be the first report of a paraprotein that has been detected from determination of the lipaemia index. Appropriate and timely investigations initiated by laboratory personnel following an anomalous lipaemia index led to a diagnosis for this patient with a type 1 cryoglobulinaemia.
Paraproteins that are characterized as type 1 cryoglobulins are almost always indicative of an underlying B-cell malignancy as in this case. 7 The patient had clearly been showing one of the well described ‘B symptoms’ of night sweats, although in this patient they also occurred during the day.
In the second case, in a patient with a known splenic marginal zone lymphoma, after noting the discrepancy between the lipaemia index and the appearance of serum, electrophoresis and immunofixation revealed an IgM paraprotein. While we were not able to identify cryoglobulin properties associated with the paraprotein, it is possible, because of the pathology involved that, prior to treatment, a cryoglobulin was in fact present. This led us to postulate that it is the properties that confer cryoglobulin behaviour that provokes precipitation with the Tris buffer-based diluent at 37°C and not those of an IgM paraprotein
In conclusion, we have reported precipitation of an IgM cryoglobulin in a Tris buffer-based diluent that has resulted in an analytical interference that manifested itself as an anomalous lipaemic index. We believe this to be the first description of this phenomenon.