
Abstract
Background
Managing workload within the laboratory has become a key role for clinical biochemists. National benchmarking data highlighted a 31% increase in C-reactive protein (CRP) requests between 2003–2004 and 2004–2005 for the University Hospital of North Staffordshire (UHNS). The aim of this study was to examine CRP requesting patterns within the acute admissions units.
Methods
Current requesting patterns within the Accident and Emergency Department (A&E) and Medical Admissions Unit (MAU) were audited. Following discussion with clinical colleagues, the laboratory implemented agreed disease-related protocols and consultant only requesting. The impact these demand management strategies had on requesting within these units was then assessed.
Results
The initial data (January–June 2005) showed that the average number of requests for CRP was 918 per month from A&E and 545 per month for MAU. Implementation of demand-management strategies resulted in an overall reduction of 85% in the numbers of requests, saving the Trust approximately £10,000 per annum. Further to the initial protocols, an IT-based logic rule was also developed to reduce CRP requests made within a 24 h time window of an initial request and educate users.
Conclusion
This study has demonstrated that strategies to control demand at the requesting stage have been able to reduce the number of requests from acute admission units. This study forms the basis for ongoing work on inappropriate requesting and illustrates that the introduction of agreed protocols in acute settings can be used as a demand-management tool.
Introduction
Devising strategies to manage laboratory workload have become a key role for clinical biochemists. Laboratory workload continues to rise by approximately 10% per annum, and a recent review stated that 25–40% of all laboratory requests are unnecessary. 1 While the laboratory seeks to educate service users regarding testing intervals, current guidelines and testing strategies, requesting remains to be frequently duplicated or not required at all. Patient care requires coordination of a range of services and the clinician and laboratory must ensure that the tests requested will positively impact on patient management. 2 Smellie 3 detailed a range of strategies to help the laboratory tackle inappropriate requesting. Initiatives including improving the design of laboratory request cards, setting criteria to monitor the frequency of requesting and altering the profile of tests available have offered laboratories some success depending on the setting. While a detailed analysis of the effect of these strategies is not the focus of this study, it is clear that laboratories can have a significant impact on requesting patterns and demand control.
The challenges facing the laboratory when attempting to manage workload is potentially assisted by an increasingly wide range of tools. For example, more sophisticated information technology (IT) and bidirectional links render it possible for the hospital clinician to review primary care-initiated results. Order communications approaches can highlight previous results or question the need for repeat testing within certain time intervals. There are also options for rule-based criteria to be set-up within laboratory computer systems to allow the staff to decide on the clinical utility of repeat testing. However, the specification of the available laboratory computer systems varies greatly and not all Trusts have access to all facilities.
C-reactive protein (CRP) represents a current typical example of the impact of unmanaged demand. National Pathology Benchmarking figures highlighted a 31% increase in CRP requests for the University Hospital of North Staffordshire, between 2003–2004 and 2004–2005 (68,454–90,015) compared with a national average increase of 16% (98,228–114,084). 4 The hospital covers a population of 500,000 and in our experience, much of the requesting is derived from units comprising non-specialist requestors. Accordingly, in this study, we set out to assess the frequency of requesting from the acute admissions units, implement demand-management protocols and determine the impact of these strategies.
Methods
An initial investigation into the clinical utility of CRP requests was undertaken by the Clinical Biochemistry Laboratory at the University Hospital of North Staffordshire in 2005. A questionnaire was circulated to consultants of all disciplines within the Trust to evaluate when CRP was clinically indicated and how often they felt it should be requested in the conditions they deemed analysis necessary. The results of the questionnaire and audit of requests of CRP indicated that CRP was being requested where it was not clinically necessary (e.g. when the diagnosis had been made and the CRP would not be acted upon) and/or too frequently in cases where it was needed, leading to increased laboratory workload and associated costs. Further examination of the requests showed that a significant proportion of these inappropriate requests came from the acute admissions units.
Following the results of the initial audit, a two-phase approach was utilized for each of the two admission units. In early December 2005, the clinical biochemists discussed the problem with the Accident and Emergency Department (A&E) Management Team resulting in a memorandum being issued from the lead consultant in Emergency Medicine to all A&E staff highlighting the need for appropriate usage. As a result, all requests for CRP from A&E had to be authorized by a consultant.
In the Medical Admissions Unit (MAU), a separate two-phase process was instigated. Initially, the clinical biochemists again met with the senior consultants overseeing MAU in June 2005 at which it was agreed that junior staff would be encouraged to limit CRP testing to only appropriate cases. This was followed-up by a more formal process of development of a protocol for Clinical Biochemistry testing in MAU based on presenting signs and symptoms. This protocol was developed in conjunction with a senior MAU consultant, a consultant nurse and the deputy business manager for Medical Division. Those signs and symptoms where a CRP request was deemed appropriate are shown in Table 1. This protocol was implemented in April 2006.
Agreed set of symptoms/clinical conditions where C-reactive protein may be requested from Medical Admissions Unit
In December 2006, an IT-based logic rule that identified repeated requests made within 24 h was also implemented based on the results of the initial questionnaire. The aim of this rule was to improve education and highlight that it is not necessary to repeat the CRP within a 24 h time window (with the exception of paediatrics). As a result, requests made within this frame were rejected and an automated comment to review the previous result was issued.
Statistical analysis
Comparison of pre- and postimplementation requesting frequencies was performed using the Mann-Whitney U test.
Results
The initial data (January–June 2005) showed that the average number of requests for CRP was 918 per month for A&E and 545 per month for MAU (Figure 1).
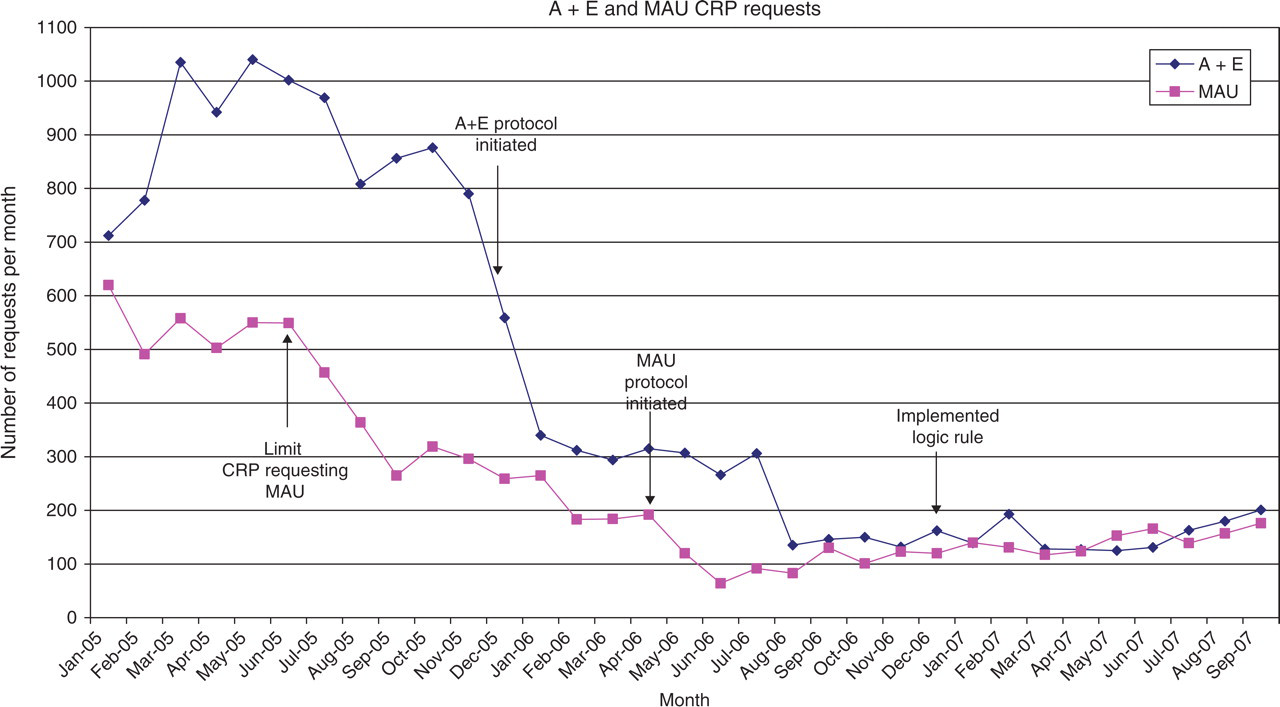
C-reactive protein requests from acute admissions units
Following the implementation of consultant only requesting in A&E, the number of requests decreased to 135 per month (August 2006). The initial discussions with clinicians on MAU lead to an immediate decrease in the numbers of CRP requesting (Figure 1). Comparison of monthly request frequency between the same period (January–June) in 2005 and 2006 demonstrated statistically significant reductions in each unit (both P < 0.005, Mann-Whitney U test). Further reductions were demonstrated with the implementation of the disease-related protocol in April 2006 to approximately 83 requests per month. Re-auditing (August 2006) requesting patterns from the acute admissions units indicated an overall reduction of 85% in the numbers of requests saving the Trust approximately £10,000 per annum at full cost. This cost was derived using a top–down approach, which calculates the full cost of CRP at 65 p. Marginal costs (reagents and consumables) for CRP were calculated at 22 p resulting in a direct laboratory saving of approximately £3500. Comparison of monthly request frequency between January and June in 2006 and 2007 demonstrated statistically significant reductions in A&E (P < 0.005) but not MAU (P = 0.262, Mann-Whitney U test).
To account for the seasonal variation of CRP, comparison of requesting patterns for the year before and after the demand-management strategies were implemented, should be undertaken. However, due to IT limitations and where intervention points occur, a review of similar six-month period highlights the impact of the agreed protocols. The combined total of CRP requests from the acute admission units for January–June 2005 equalled 1463, compared with the same time point in 2007 when CRP requests had dropped to 279. As expected, comparison of monthly requests in the first six months of 2005 and 2007 demonstrated statistically significant reductions in each unit (both P < 0.005, Mann-Whitney U test).
Re-auditing CRP requesting patterns from the other wards showed that the overall numbers of requests had not increased. Indeed, examination of the data showed that the number of CRP requests from other wards (excluding the targeted acute admission wards) decreased by 12% from 6218 to 5486 between the same first six months of 2005 and 2007 (P=0.025; Mann-Whitney U test), supporting the view that there had not been a shift of requesting from the acute admissions units to the wards. This decline appeared to start during the first six months of 2006 possibly indicating a wider impact of the policy beyond the acute admission wards in line with staff rotation.
Discussion
Managing laboratory workload has become a major challenge within Clinical Biochemistry. National Pathology benchmarking data highlighted that the University Hospital of North Staffordshire had a higher percentage increase of CRP requests per annum than the national average. Upon further investigation, the high frequency of CRP requesting within acute admission units was assessed and targeted. Through working with clinicians and the IT department, strategies within the acute admission units were devised and implemented. As a result of the demand-management strategies introduced, the saving to the Trust is approximately £10,000 per annum. While this study may have a lack of formal evidence base for the implemented protocols, clinical colleagues have a wealth of experience and this, together with laboratory collaboration, can positively impact on requesting patterns and service provision. Clinical Biochemistry Departments, and clinical biochemists in particular, should balance responding to the needs of the users together with a formal evidence base. However, where this is not available, studies like this can be a useful first step.
Re-auditing to detect any increases or shift of requesting to other units was vital. As part of this study, requesting patterns from other wards was assessed to ensure that there was not a shift of requesting. The department also implemented an IT-based logic rule. While the implementation of the logic rule does not appear to have made a significant impact on reducing the number of requests from the acute admission units, this rule has been applied to all requestors. It is thought that the rule has helped identify existing CRP results to the wards and in turn reduce the number of repeat requests made within a 24 h time window. Discussions with colleagues in other Trusts (using the Association for Clinical Biochemistry Mailbase) suggest from internal audits that this strategy alone can reduce the number of CRP tests by up to 6%. This has not been validated as part of this study due to the impact of the other strategies on requesting patterns, but will form part of the continued investigation of requesting within the rest of the Trust.
Education also remains to be of vital importance in managing demand. Figure 1 highlights a slight increase in requesting from July 2007. This may be due to recruitment of newer members of staff who are not aware of Trust protocols. Following this study, the acute admission units have merged. As a result, increased CRP requesting has been detected. However, an updated condition-based protocol and request card to meet the requirements of this wider group of patients is now being devised.
As Jackson states, 2 tackling the problems of optimizing laboratory requesting does require both clinicians who are open to feedback and laboratory staff who are not afraid to state their case. Clinical Biochemistry must be involved in guideline development and care pathway discussions and this, along with the current emphasis on evidence-based medicine, will help to identify areas of inappropriate requesting that may be targets for future improvement. Our study also illustrates that, while laboratories often concentrate on managing demand for expensive low volume tests, it may be more cost-effective to focus on reducing the high numbers of low-cost tests. Laboratories must also move away from the attitude that it is easier to accept tests that are on automated platforms than spend time devising complex rules and protocols, as this will be the area where managing demand could have the biggest impact and hence cost savings.
This study has demonstrated strategies to control demand at the requesting stage that, with the support of clinical colleagues, have been able to reduce the number of requests from acute admission units. As demonstrated, targeting requesting patterns by agreed protocols require the input and support of clinicians and ongoing education to junior doctors and nurses if these are to form part of the strategy to sustain a reduction in inappropriate testing. As a result, clinical biochemists have a vital role not only in the development and implementation of demand-management strategies and protocols but also in the continued education and assessment of such strategies as part of the wider task of reducing inappropriate testing and improving patient care.