
Abstract
Background
Human faecal elastase-1 (FE-1) is an established biochemical test for the investigation of pancreatic exocrine insufficiency. Conventional extraction methods for FE-1 analysis can give false-positive results with watery stools. This is a major limitation as patients investigated for pancreatic disease commonly produce such stools. We have developed an improved FE-1 test that overcomes water interference by measuring the enzyme in dried faeces.
Methods
A novel collection device for FE-1 analysis that involves drying and weighing the stool sample was developed in our laboratory and compared with a conventional wet method, E1 Quick-Prep (Schebo, Biotech AG, Germany). The concentration of faecal FE-1 was determined using a commercially available enzyme-linked immunosorbent assay method (Schebo).
Results
FE-1 values obtained using the new dry extraction procedure (mean 1777 μg/g dry stool) were higher when compared with the conventional wet analysis (mean 402 μg/g stool). A 1:2 dilution in water, mimicking a loose stool, was found to affect FE-1 results obtained using the conventional wet extraction procedure. The new dry extraction method gave consistent results when water content was varied in the original stool sample.
Conclusion
We have demonstrated that our new device overcomes water interference, allowing results to be obtained from stool samples that would otherwise be unsuitable for FE-1 analysis.
Introduction
Diagnosis of exocrine pancreatic insufficiency can be difficult and challenging. This reflects the methodological limitations of direct and indirect pancreatic function tests. Although direct tests confer sensitivity and specificity, they are generally invasive, making them unsuitable for routine application. Simple, less-invasive and indirect methods have limited sensitivity in mild and moderate exocrine pancreatic disease and are interfered with by drugs, diarrhoea, pH and gastrointestinal operations, which lower their specificity. In an attempt to identify a simple, yet sensitive and specific biochemical test for exocrine pancreatic function, an enzyme-linked immunosorbent assay (ELISA) method has been developed for the determination of the faecal concentration of faecal elastase-1 (FE-1) and has been commercially available since the early 1990s. 1
Studies have focused on the FE-1 test in detail and revealed that it correlates well with other direct and indirect tests of exocrine pancreatic function. 2–11 The test performs well in the diagnosis of severe pancreatic insufficiency, but not so in the diagnosis of mild and moderate disease. However, when compared with other faecal tests such as chymotrypsin, it performs much better in terms of sensitivity in mild and moderate pancreatic insufficiency. 3,5,10,12 Furthermore, a number of studies in children showed excellent sensitivity and specificity rates (90–100% and 95%, respectively). 13–16 Determination of the faecal concentration of FE-1 is currently the first-line biochemical investigation offered for exocrine pancreatic impairment, its use being supported by the British Society of Gastroenterology (BSG) Guidelines. 17
A central limitation of the FE-1 test in the study of chronic pancreatic disease is the inherent variability due to water content. 18–20 Due to a dilution effect, the FE-1 concentration in watery stool samples may be lowered and give a false-positive result, leading to further unnecessary investigations, inappropriate use of resources and patient management. Very high water content can also lead to the sample being unsuitable for analysis, therefore delaying biochemical diagnosis and initiation of appropriate treatment.
We have offered a service for faecal determination of FE-1 in the UK for over 5 y. Approximately, 18% of the samples we receive have a high water content, of these 50% are so wet that they cannot be analyzed and the other 50% are sent out with the comment ‘interpret results with caution, suggest repeat on a formed stool’. To improve our service we have attempted to overcome the problems of varying water content in stool samples by measuring FE-1 in dried faecal samples. Here, we describe our new dry faecal extraction procedure. We have used this new method to establish reference intervals in a study of 300 patient samples, and using stool samples from patients with exocrine pancreatic impairment, compared with its performance in the conventional extraction procedure.
Patient samples and methods
Reference study
Anonymized stool samples (300) sent for routine microbiology analysis were obtained over a one-month period in November 2006. A 5 mL portion of each stool was placed in a test tube and capped. Samples were stored for a maximum of one month at −80°C prior to analysis. Watery samples were excluded from the study.
Recovery study
Stool samples with a normal consistency from a healthy volunteer, a patient diagnosed with mild pancreatic exocrine insufficiency and severe pancreatic exocrine insufficiency were diluted with water 1:1, 1:2, 1:4 and 1:8 and mixed in a blender to create homogenous watery stool samples.
Comparison study
Stool samples (60) from patients admitted to hospital for the differential diagnosis of malabsorption syndromes or with previously established causes of malabsorption were used. Ages ranged from two months to 87 y with a mean age of 43 y; 37 of the subjects were male and 23 female.
All the stool samples were analysed using the conventional Schebo E1 Quick-Prep wet extraction procedure and the new dry method.
Conventional stool extraction method
Wet stool samples were prepared using a conventional wet method, E1 Quick-Prep (Schebo, Biotech AG, Germany). Briefly, the dosing tip of the device was used to collect samples from three different locations of the stool. Once all the notches on the tip were filled, the tip was placed in extraction buffer and extracted for 10 min. A 1:70 dilution in Schebo washing buffer was then prepared according to the manufacturer's instructions.
Dry stool extraction method
A new device was created for the capture and drying of stool samples for FE-1 analysis. This new faecal collection device comprises of a monofilament nylon mesh (Sericol UK Limited) supported on a plastic parcel tape. Accurate strips of the collection device were produced by a hand-held SP1 32 × 25 mm photo-cutter (Polaroid, Hertfordshire, UK). A pea-size portion of stool was layered onto the device using a wooden tongue depressor (Universal Hospital Supplies, Enfield, UK) and left to dry overnight at room temperature in a fume hood. To determine the amount of stool present, the collection device was weighed using a Reflex HP220c Balance (Avery Weigh-Tronix, West Midlands, UK). The weight of dry stool was calculated by subtracting the weight of the collection device from the weight of the device plus the dry stool.
The device was placed in a 10 mL glass tube with Schebo washing buffer (final concentration 2 mg dried faeces/mL of buffer) and the stool extracted by vortex-mixing for 2 min. The stool extract was then mixed for a further 10 min on a roller mixer. The vortex and roller mixing steps were repeated.
To remove particulate matter, the stool extract was centrifuged at 4230 rpm (Rotanta 460, Hettich-Zentrifugen, Hettich AG, Germany) for 5 min and the supernatant transferred to a labelled tube. For FE-1 analysis, a 1:250 dilution in Schebo washing buffer was prepared.
Measurement of faecal elastase-1 concentration of extracts
FE-1 concentration for both wet and dry extractions was determined immunologically using a commercially available ELISA (Schebo, Pancreatic Elastase 1) according to the manufacturer's instructions. Optical densities were measured using a Dynex MRX II plate reader with Revelation Version 4.06 software (Dynex Technologies, West Sussex, UK). In wet conventional analysis (Schebo E1 Quick-Prep), FE-1 results were expressed in μg/g stool. For the new dry extraction method, results were expressed in μg/g dry stool.
Statistics and calculations
Data were analysed using MINITAB Statistical Software, Version 13 (Minitab Inc., USA).
Results
Extraction device
The weight of the device was found to be highly consistent with a between-batch coefficient of variation of 0.35% (mean weight 212 mg, n = 20). The device remained flat during the drying process. Once dried, the stool tended to form flakes and there is a risk that most of the sample will be lost. The mesh on the device was found to minimize this flaking. The device was not affected by prolonged contact with the washing buffer used in the extraction procedure.
Stability studies
The stability of FE-1 in dried stool was studied using a homogenized sample with normal FE-1 concentration. The results are presented graphically in Figure 1. The enzyme was found to be very stable in dried faeces over 24 d of study.
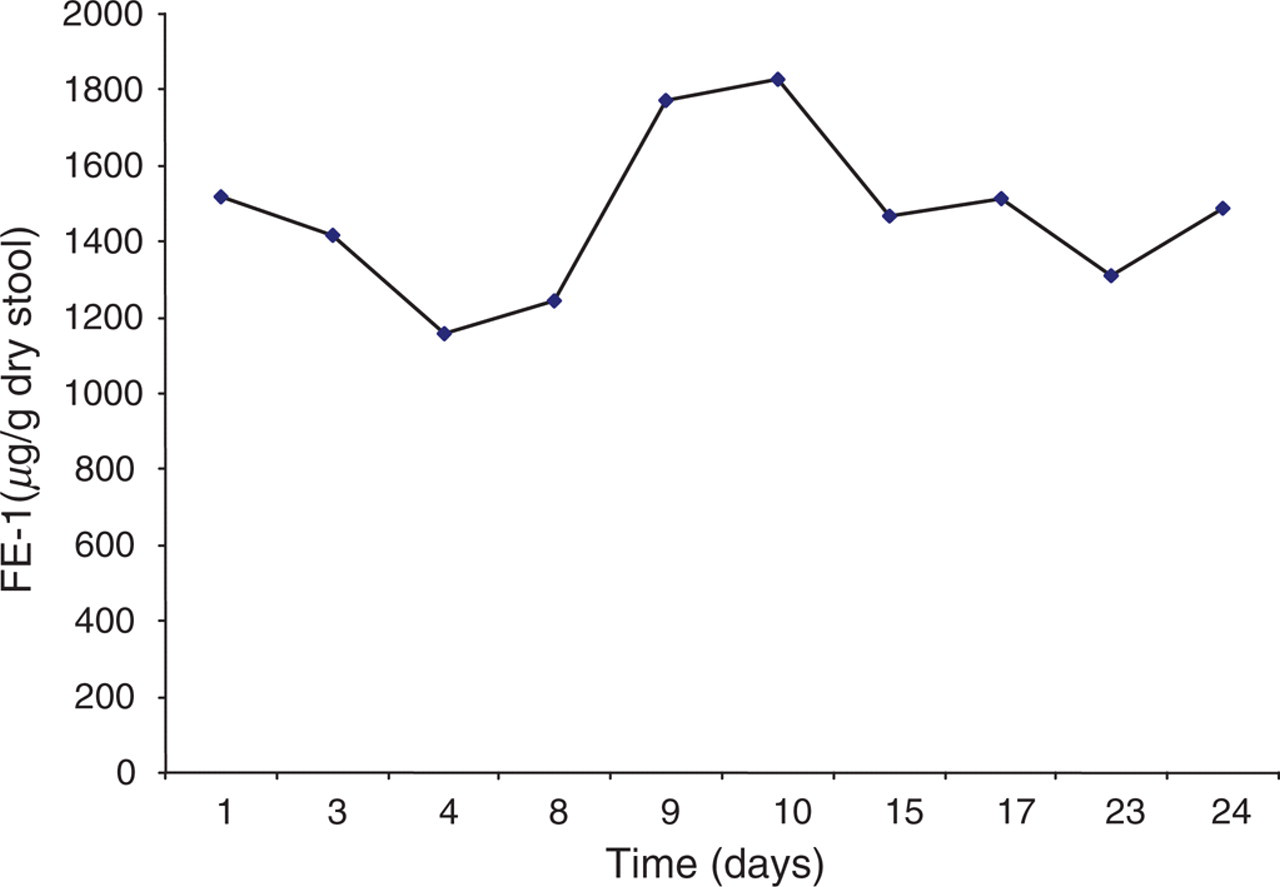
Stability study using a stool sample with a normal faecal elastase-1 concentration measured using the new dry extraction method
Precision studies
The imprecision of the new dry extraction method was established using a stool sample with normal consistency from a healthy volunteer. Results for within-batch and between-batch imprecision compared with the conventional Schebo E1 Quick-Prep wet extraction method are presented in Table 1.
Within-batch and between-batch imprecision data for faecal elastase-1 analysis using conventional Schebo E1 Quick-Prep wet and new dry extraction methods
n = 10. FE-1, human faecal elastase-1; CV, coefficient of variation
Recovery studies
The results for the recovery experiments using stools diluted with water are shown in Figure 2. For the 1:1, 1:2 and 1:4 dilutions, the watery nature of the stools increased and with 1:8 dilution, the sample was watery. Using the conventional Schebo E1 Quick-Prep wet extraction method, a stool sample from a volunteer with a normal FE-1 concentration gave a result consistent with moderate-to-mild exocrine pancreatic insufficiency after a 1:4 dilution with water (slightly loose stool), and severe exocrine pancreatic insufficiency after a 1:8 dilution (watery stool). A sample from a patient with moderate-to-mild exocrine pancreatic insufficiency result became severe after a 1:2 dilution with water. The results obtained using the new dry faecal extraction procedure were not affected by the volume of water added, with all dilutions giving the same result as the undiluted stool.
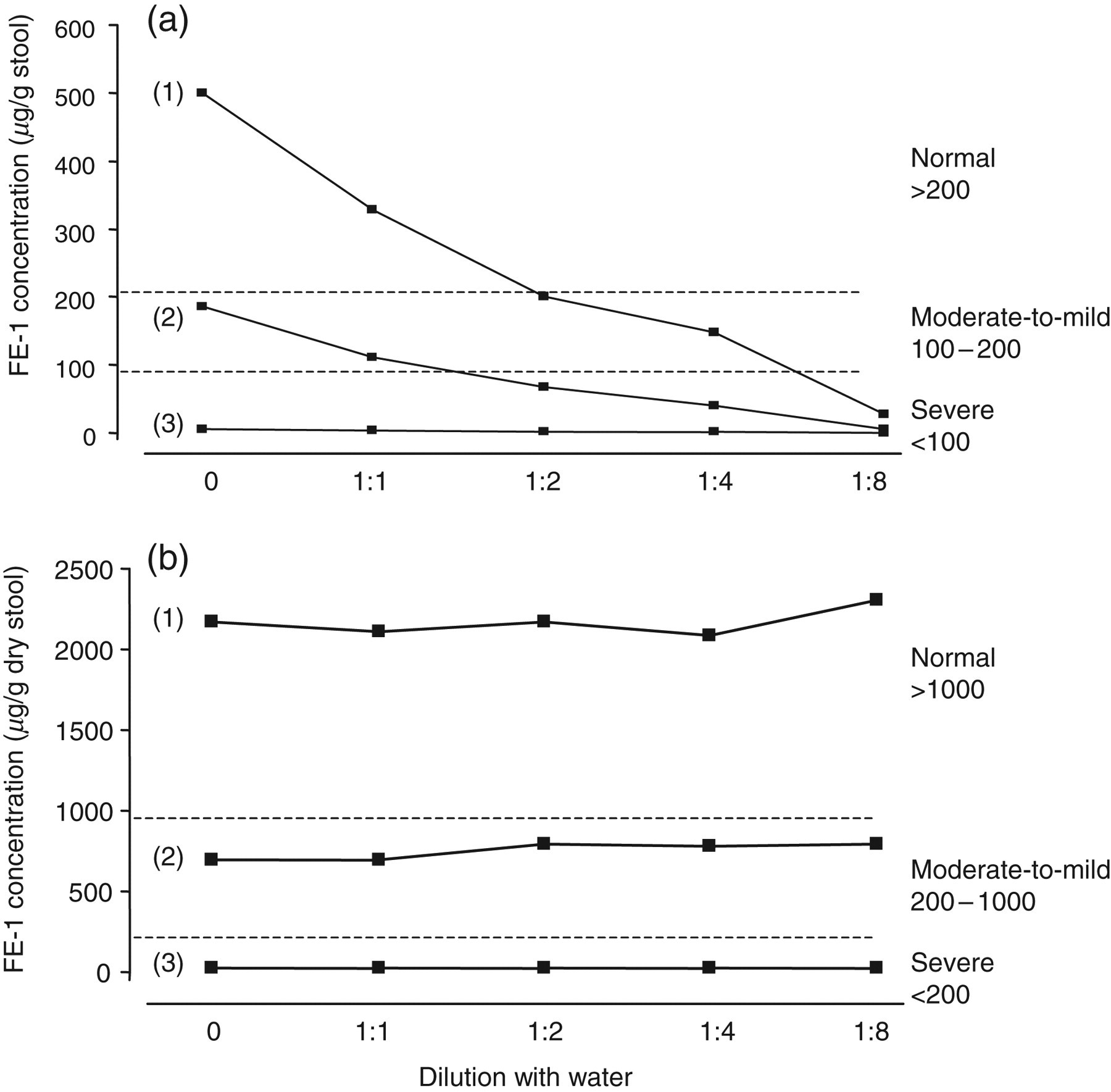
Recovery studies using stool samples with normal pancreatic function and moderate-to-mild and severe exocrine pancreatic insufficiency diluted with water. Faecal elastase-1 (FE-1) concentration measured using (a) conventional Schebo E1 Quick-Prep wet extraction method and (b) new dry extraction method. Reference concentrations for FE-1 for both extraction methods are indicated by the broken lines. (1) Stool sample with normal FE-1 concentration; (2) stool sample with moderate-to-mild exocrine pancreatic insufficiency; (3) stool sample with severe exocrine pancreatic insufficiency
Comparison of extraction methods
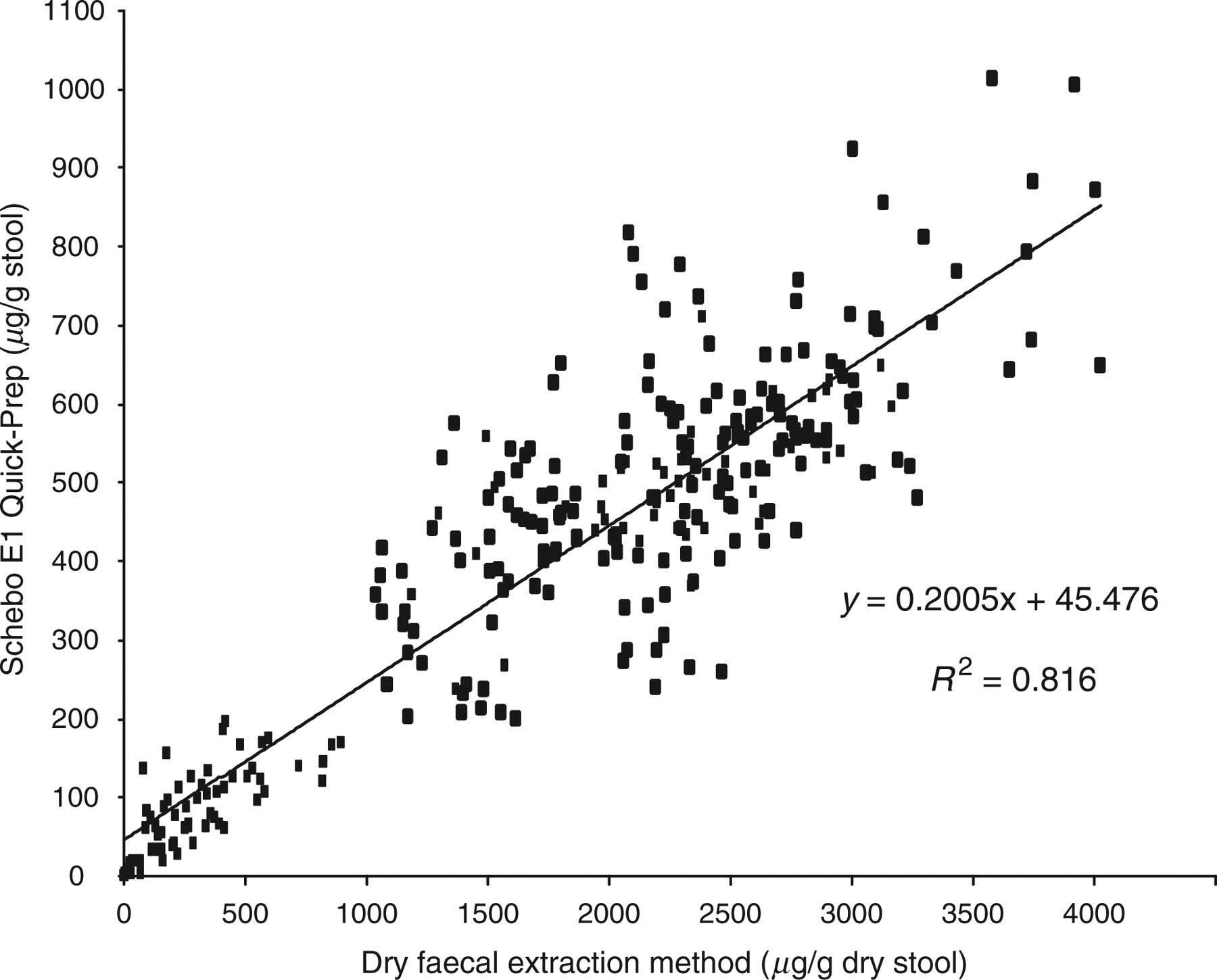
The results of FE-1 analysis of the 300 stool samples using conventional Schebo E1 Quick-Prep wet analysis and the new dry extraction method are shown in Table 2 and compared as shown in Figure 3. The concentration of FE-1 using the new dry method was higher compared with conventional analysis with mean FE-1 concentrations of 1777 μg/g dry stool and 402 μg/g stool, respectively.
Comparison of faecal elastase-1 results for 300 study samples using conventional Schebo E1 Quick-Prep wet and new dry extraction methods
Faecal elastase-1 results for 300 study samples using conventional Schebo E1 Quick-Prep wet and new dry extraction methods
FE-1, Human faecal elastase-1. Values for Quick-Prep wet extraction are in μg/g stool and for new dry extraction method μg/g dry stool
Reference intervals for new dry extraction method
The reference intervals for the new dry method were derived from comparison with the FE-1 results obtained for the 300 study samples using the conventional Schebo E1 Quick-Prep wet extraction method and are presented in Table 3. The concordance between the two extraction methods for all results was 100%; 45 (15%) were categorized as having severe exocrine pancreatic insufficiency, 28 (9%) with moderate-to-mild exocrine pancreatic insufficiency and 227 (76%) with normal exocrine pancreatic function.
Reference concentrations for faecal elastase-1 (FE-1) using conventional Schebo E1 Quick-Prep wet and new dry extraction methods
Sample comparison
Both the conventional Schebo E1 Quick-Prep wet extraction method and the new dry method were used to analyse 60 stool samples received for routine FE-1 analysis. Of these stool samples, 57 were of a normal consistency and the remaining three samples were watery. In the samples of normal consistency, the concordance between the two extraction methods was 100%; 29 severe exocrine pancreatic insufficiency, 11 moderate-to-mild exocrine pancreatic insufficiency and 20 normal exocrine pancreatic function. For the three watery samples, the two extraction methods gave different results. One sample gave a result consistent with moderate-to-mild exocrine pancreatic insufficiency using the conventional Schebo E1 Quick-Prep wet extraction method (150 μg/g stool), but a normal result with the new dry method (2312 μg/g dry stool). The other two samples yielded results consistent with severe exocrine pancreatic insufficiency using the conventional wet extraction method (both 30 μg/g stool) but moderate-to-mild exocrine pancreatic insufficiency results with the new dry method (410 and 330 μg/g dry stool).
Discussion
The Schebo Pancreatic Elastase 1 kit insert states that in case of pathological FE-1 concentrations <200 μg/g stool in watery stool samples, a second formed stool sample should be requested. 20 We have found that for a large percentage of the routine requests we receive, the stools are wet and this is not surprising as patients investigated for pancreatic disease are likely to produce such stools. The need for a repeat formed stool leads to extra clinic visits and may delay diagnosis. We therefore developed a new method for preparing stools for FE-1 analysis, which removes the water. Using this new method, we have been able to demonstrate that even slightly loose stools (1:2 dilution of water) affects FE-1 concentration using conventional Schebo E1 Quick-Prep wet extraction, and could give misleading results. This is significant as such stools may not be considered watery, as stool samples can be applied to the dosing tip.
An interesting finding of this study was the number of results in the 300 stool samples randomly taken from microbiology requests for routine analysis that gave FE-1 results consistent with severe exocrine pancreatic insufficiency (15%), and moderate-to-mild exocrine pancreatic insufficiency (9%). We have previously reported a similar high number of FE-1 results consistent with moderate-to-mild and severe exocrine pancreatic insufficiency in randomly selected stool samples for faecal occult blood analysis. These findings reflect the difficulty in diagnosing exocrine pancreatic insufficiency and suggest that many patients remain undiagnosed and are undergoing unnecessary investigations.
Despite more operator-involved steps, including weighing, the precision of the dry extraction method was found to be similar to that of the Schebo E1 Quick-Prep. The new dry extraction method does take longer to prepare samples when compared with the conventional method, and in practice we have been limiting its use to loose and wet samples. The disadvantage with this approach is the difference in reference concentrations between the two extraction methods, as there is a risk that users will apply the wrong one. To minimize this risk, we send a covering letter with all results. Since the introduction of this method, we have been able to report results for 141 wet samples (11% of total workload) that previously we would not have done, significantly reducing the need for repeat faecal sampling.
Further work needs to now focus on determining if it is possible to convert the reference ranges for the dry extraction method to those of the conventional method for better comparison, or indeed, if it is practicable to move over to using dry faecal analysis as the primary assay.
Footnotes
Acknowledgement
Thanks to the Microbiology Department at Sandwell Hospital for the 300 anonymized stool samples.