
Abstract
Serotonin is frequently analysed by high-performance liquid chromatography (HPLC) with electrochemical detection. However, the accuracy of these methods may be affected by the presence of certain drugs. We describe for the first time the interference of paracetamol in therapeutic dosages in a routine HPLC method for serotonin determination in vivo and in vitro. The retention time coincides with N-methylserotonin used as an internal standard in this method. Erroneous increases of the internal standard will lead, if not recognized and corrected, to falsely low serotonin determinations.
Carcinoid syndrome is clinically characterized by a multitude of symptoms, including cutaneous flush, diarrhoeae, bronchospasm, and others. These clinical signs are mediated via numerous humoral factors like polypeptides, biogenic amines and prostaglandins. In almost all patients with carcinoid syndrome, altered metabolism of tryptophan occurs. While in normal subjects, approximately 1% of dietary tryptophan is metabolized to serotonin, tryptophan metabolism is markedly enhanced to 70% or more in patients with carcinoid syndrome. Serotonin is then degraded to its end-product 5-hydroxyindole acetic acid (5-HIAA). 1 Measurement of 24-h urinary excretion of 5-HIAA is the most useful initial screening test for the carcinoid syndrome. 2 However, the determination of serotonin concentration in platelet-rich plasma or serum may help to support the diagnosis, particularly when urinary 5-HIAA results are equivocal. 3
Serotonin is frequently analysed by HPLC, because immunological assays are not available and mass spectrometric methods are very expensive and laborious. In our laboratory, serum serotonin is measured by a commercially available HPLC method (Chromsystems, Munich, Germany). After deproteinization of the sample, the internal standard N-methylserotonin is added. An aliquot is applied on a reverse-phase column and eluted at a flow-rate of 1 mL/min. The analytes are determined by electrochemical detection, with a potential of 500 mV. The retention times of serotonin and N-methylserotonin are 4.8–5.4 min and 6–7 min, respectively.
We sometimes observed an unknown peak in the serotonin chromatogram that interfered with the internal standard N-methylserotonin, an example is shown in Figure 1a. Evaluating the drug history of these patients, we found that the patients had taken, among other drugs, paracetamol within 12 h before blood collection. Therefore, we hypothesized that administration of paracetamol may have led to the interference with N-methylserotonin.
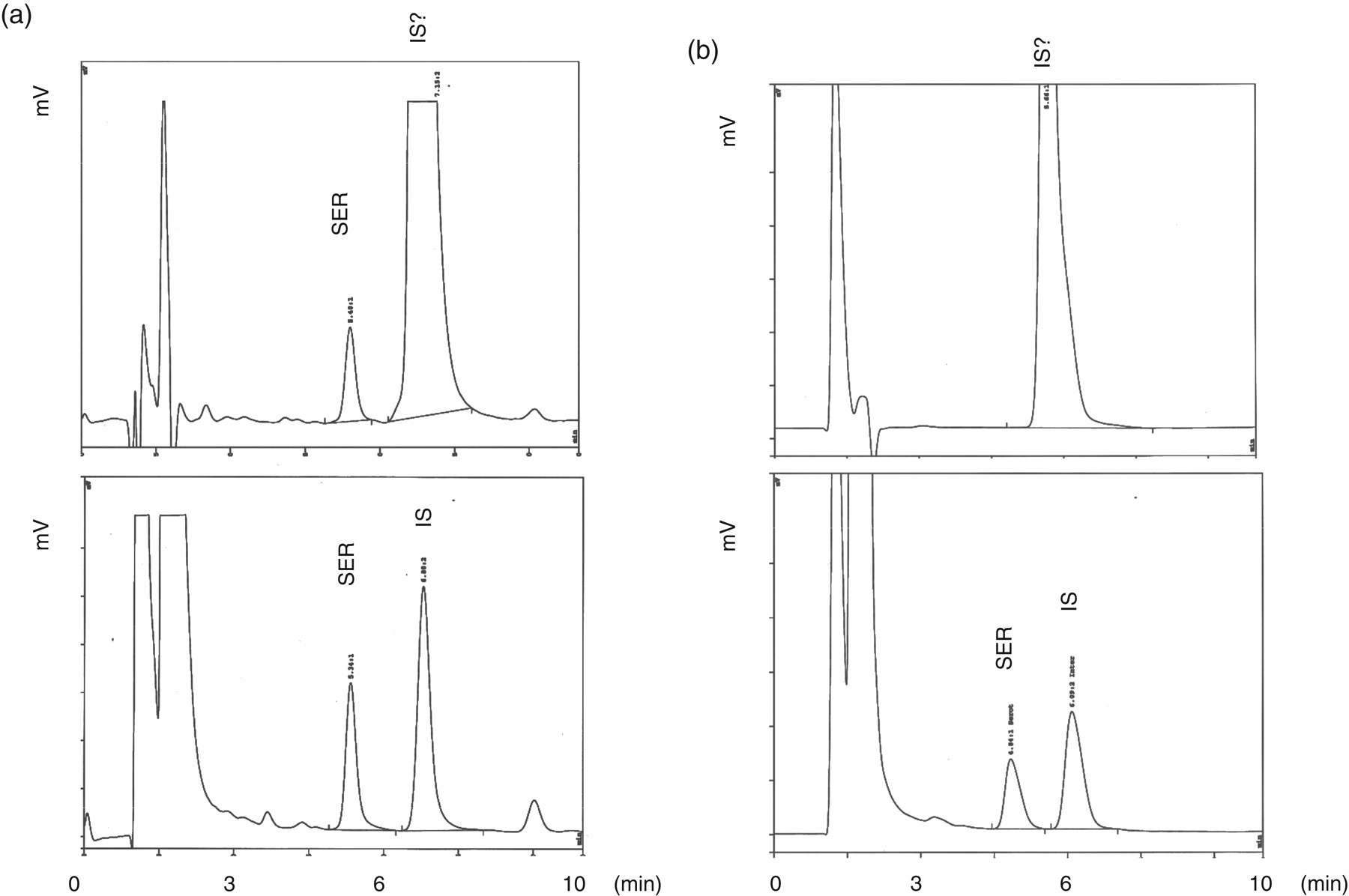
High-performance liquid chromatograms of serotonin analysis. The length of the run is 10 min. Serotonin (SER) has a retention time of 4.8–5.4 min, while the internal standard (IS) has a retention time of 6–7 min. The interference at the retention time of the IS is indicated with ‘IS?’. (a) Above: Serotonin was analysed in a patient treated with paracetamol resulting in a plasma concentration of 18 mg/L. Below: For comparison, the calibrator of the run is depicted with a normal amount of internal standard. (b) Above: Chromatographic separation of an aqueous solution of paracetamol is depicted with a concentration of 10 mg/L. Below: For comparison, the calibrator of the run is depicted with a normal amount of internal standard
Paracetamol is widely used as an over-the-counter drug because of its analgesic and antipyretic properties. Approximately one-third of the population takes paracetamol at least once monthly 4 .
Testing paracetamol in vitro for interference with serotonin HPLC analysis, we found a marked peak indistinguishable from the internal standard at a concentration of 10 mg/L (Figure 1b). In contrast, no interferences with the other reported drugs were detected (not shown). Pharmacokinetics of paracetamol have been studied in detail. Therapeutic serum concentrations after standard dosage are 10–30 mg/L. However, serum concentrations are reported to reach up to 64 mg/L. 5 Determination of paracetamol levels in our patients with disturbed serotonin analysis on a Dimension RXL (Siemens, Eschborn, Germany) revealed paracetamol concentrations ranging from 14.9 mg/L to 58.5 mg/L. For instance, in the patient whose serotonin analysis is shown in Figure 1a, serum concentration of paracetamol was determined at 18 mg/L. At low concentrations of paracetamol (1 mg/L), the interfering peak caused by paracetamol can be distinguished from the peak of the internal standard since paracetamol elutes approximately 0.3 min earlier. However, when serum paracetamol concentrations exceed 10 mg/L, the corresponding peak overlaps with the internal standard yielding falsely low results, as serotonin concentrations are calculated via the peak height of the internal standard.
Trying to avoid this interference, we found that the described interference could be minimized using a rather new column (less than 300 injections) as well as by lowering the potential. However, these conditions are not easily preserved for economical and logistical reasons under routine conditions. We informed the manufacturer about the interference and Chromsystems (R. Lukacin, personal communication) is going to include a warning in their instructions concerning the paracetamol interference in serotonin measurement.
It is worth noting that paracetamol belongs to those drugs that are recommended to be discontinued prior to laboratory testing for serotonin and 5-HIAA, as they may falsely increase their concentrations. However, the source of this information remains doubtful and reports about biological effects of paracetamol on serotonin concentrations are controversial. Some found decreased concentrations of the metabolic end-product 5-HIAA in paracetamol-treated rats, 6 whereas others found a minimal rise in platelet serotonin concentrations after chronic paracetamol treatment. 7 Interestingly, paracetamol-associated interference in HPLC with electrochemical detection was described earlier for urinary catecholamines, 8 so, the frequent finding of paracetamol interference is not only because of its widespread application but also because it is easily oxidized during electrochemical detection.
To the best of our knowledge, this is the first report on an analytical interference of serotonin HPLC analysis by paracetamol, which appears to be of clinical significance considering the widespread use of paracetamol. Therefore, patients should be instructed to discontinue paracetamol prior to serotonin measurement. Our findings underline the importance of good communication between laboratory and clinical units if high-quality laboratory results are to be maintained.
Footnotes
Acknowledgements
We thank Steffi Hasanovic for her excellent technical assistance.