
Abstract
Neonatal jaundice is common, and usually harmless, because of physiological jaundice or breast-feeding. In some neonates unconjugated bilirubin concentration, coupled with other risk factors, is sufficient to allow free bilirubin to cross the blood-brain barrier and cause kernicterus. Another subgroup of infants is jaundiced because of elevated conjugated bilirubin; a marker for a number of pathological conditions. Bilirubin measurement must identify those infants at risk. Transcutaneous bilirubin measurement is increasingly used in healthy infants, especially before early discharge or at home, to assess the need for laboratory bilirubin measurement. Transcutaneous measurements are not covered by laboratory quality assessment schemes. Guidelines on management of neonatal jaundice utilize age in hours and other risk factors to define bilirubin action thresholds, which may be as low as 100 μmol/L for sick premature infants, whereas early discharged babies may only present after bilirubin concentrations are extremely high. Hence, there is a requirement for accurate total bilirubin measurement from <100 to >500 μmol/L, with sufficient precision to assess the rate of bilirubin change with time. Babies presenting with late jaundice always require conjugated bilirubin measurement. It is of concern that many total and direct bilirubin automated kit methods suffer from haemolysis interference, while use of in-house methods or modification of commercial methods has virtually disappeared. External quality assessment has a vital role in providing data on different methods' performance, including accuracy, precision and susceptibility to interference. Laboratories should consider whether their adult bilirubin methods are suitable for neonates.
Introduction
An understanding of the normal processes of bilirubin production and disposal is key to a structured approach to the laboratory investigation of neonatal jaundice. 1
Bilirubin production
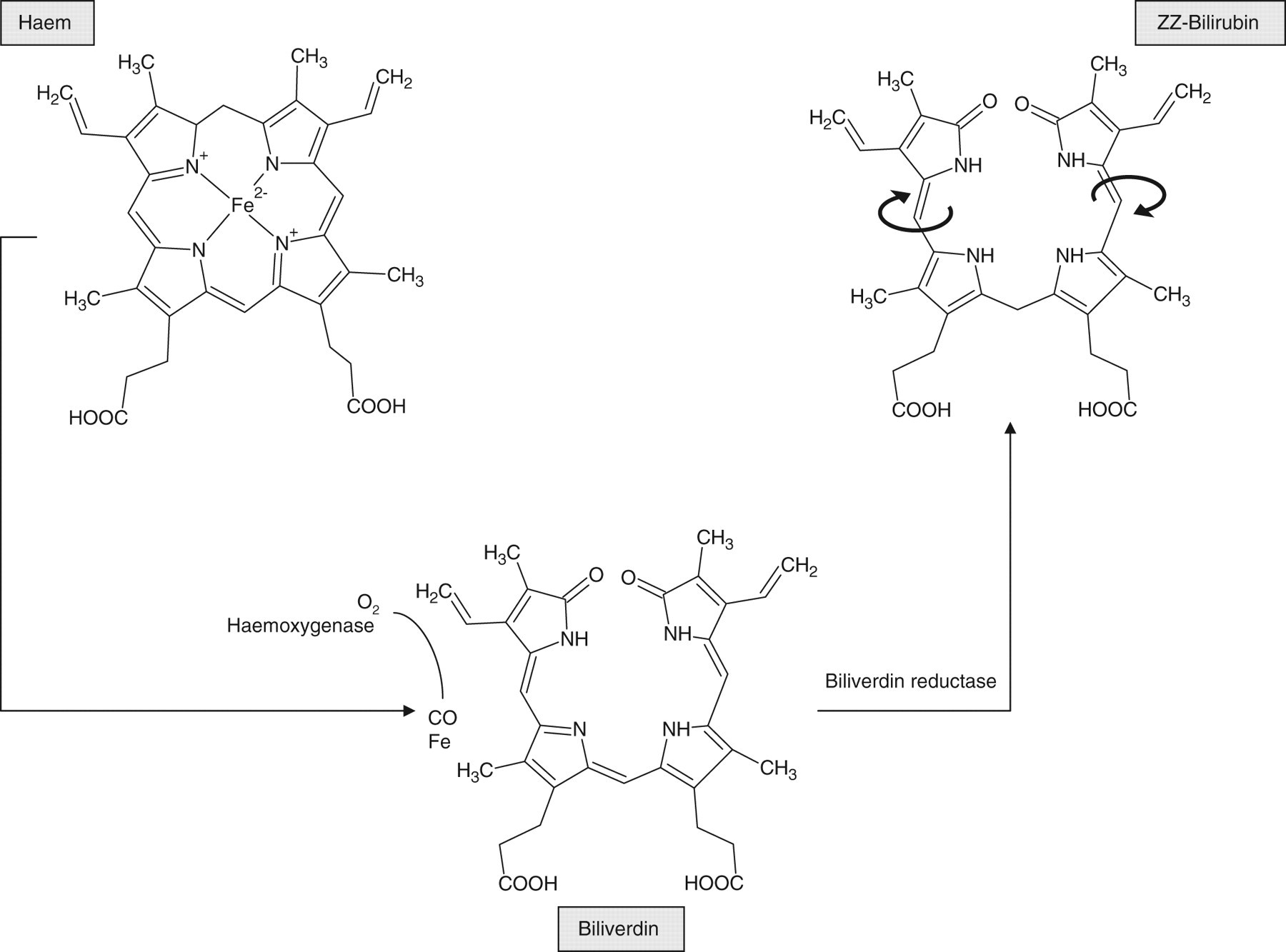
Bilirubin is formed as a breakdown product of haem. 2 In phagocytic cells of the reticuloendothelial system, the action of haem oxygenase opens up the tetrapyrrole ring of haem to produce biliverdin and carbon monoxide. Biliverdin is then reduced to bilirubin by biliverdin reductase (Figure 1).
Metabolism of haem to form bilirubin
During intrauterine life, the developing infant requires a high haemoglobin concentration to extract oxygen effectively from maternal blood and deliver it to fetal tissues. Immediately after birth, with a plentiful supply of oxygen from its own lungs, this requirement drops dramatically. The neonate's reduced red cell lifespan compared with adults means that all newborns have a considerable excess load of haemoglobin 3 to convert into bilirubin and excrete in the immediate postnatal period. Following delivery, a significant proportion of neonates may have additional haemoglobin to dispose of as a result of bruising or other losses. Haem oxygenase-1 is induced by inflammatory mediators, leading to a further increase in haem breakdown in premature infants with co-morbidities, such as respiratory distress syndrome 4 and bronchopulmonary dysplasia. 5 With such an exceptional load on an immature system, it is therefore not surprising that approximately half of all infants become jaundiced in the first week of life. 6
Forms of bilirubin found in plasma
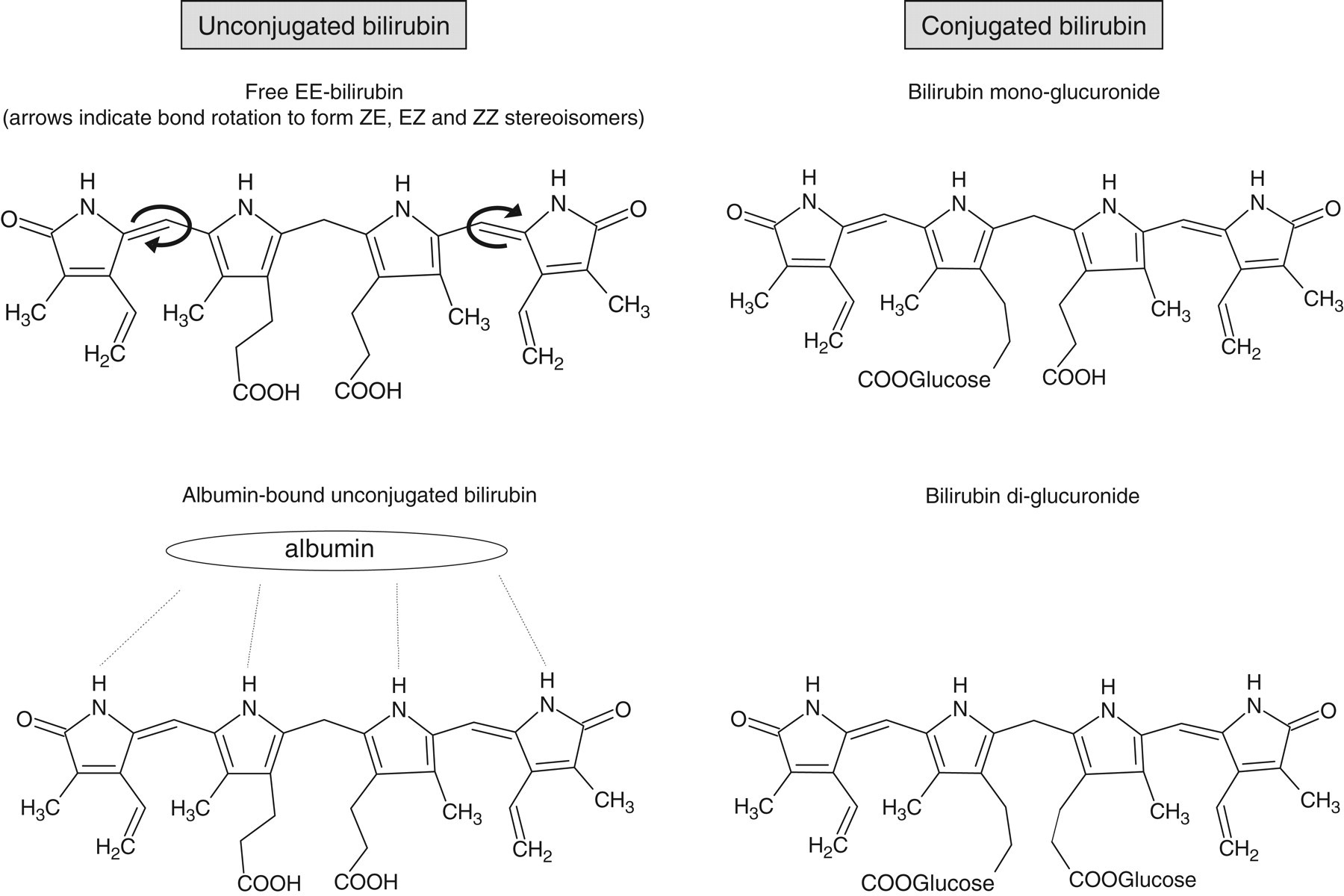
Bilirubin can be considered as an unravelled product of haem, but although it is usually represented in two dimensions on the printed page (Figures 1 and 2), its three-dimensional structure and hence the number of exposed reactive groups is an important factor in its further metabolism. 7 Owing to internal hydrogen bonding, ZZ-bilirubin, the predominant form in neonates, has a three-dimensional structure mirroring the closed ring structure of the parent haem molecule (Figure 1). Rotation around the two double bonds between pyrrole rings result in ZE-bilirubin and EZ-bilirubin (cyclobilirubin) (Figures 1 and 2), which accounts for 14% and <1%, respectively, of circulating bilirubin in healthy one-month old infants. 8 These forms have a more open configuration, have more reactive groups exposed and are hence more soluble than ZZ-bilirubin. Phototherapy promotes the formation of soluble forms of bilirubin.
Structural forms of bilirubin
As a result of the large number of potentially reactive groups, very little bilirubin exists free in the circulation. Most 9,10 rapidly associate with albumin, through a network of reversible hydrogen bonds (Figure 2). Bilirubin can be displaced from albumin by many other compounds, 11 including hydrogen ions, free fatty acids, furosemide, benzoate, benzyl penicillin, phenobarbital and salicylate. Together, free- and albumin-associated bilirubin are referred to as unconjugated bilirubin.
Neonates with conjugated hyperbilirubinaemia develop elevated concentrations of delta bilirubin (δ-bilirubin), characterized by physical and chemical properties as tightly and covalently bound to protein, mainly albumin. The site of protein attachment leaves reactive groups free to bind to azo dyes; thus δ-bilirubin contributes to total and direct bilirubin measurements. Its concentration increases in proportion to the duration of jaundice, and its half-life of 22 days is the same as that of albumin. 12
Hepatic bilirubin clearance
On reaching the liver, albumin-bound bilirubin passes to the space of Disse, between the endothelium and hepatocytes. 13 Bilirubin crosses the hepatocyte membrane through a specific carrier protein, and binds to glutathione-S-transferase B (ligandin). On reaching the microsomes, bilirubin is covalently conjugated to glucuronic acid by bilirubin uridine diphosphate glucuronosyl transferase (UDPGT) forming mono and diglucuronides (β and γ bilirubin), collectively known as conjugated bilirubin (Figure 2). Different mutations in UDPGT result in the inherited unconjugated hyperbilirubinaemias, Gilbert's syndrome and the rarer Crigler-Najjar type I and II syndromes. 14
The water-soluble bilirubin glucuronides are excreted through bile canaliculi and the bile duct system into the duodenum. The process requires an export pump transporter and carrier proteins. The export transporter is defective in Dubin Johnson syndrome. 13 Bilirubin may be reabsorbed from the gut, and this enterohepatic circulation is increased in breast-fed infants. 15
Increased understanding of the biochemical pathways involved has brought out not only identification of the precise defect in the rare inherited hyperbilirubinaemias, but also the realization that certain groups of infants are more likely to suffer from neonatal jaundice than others.
Unconjugated hyperbilirubinaemia in the neonate
Physiological and breast milk jaundice
It will be apparent from the description of normal bilirubin formation and excretion, that disposing a bilirubin load in early extrauterine life is a major challenge even for the healthy term neonate.
The natural history of uncomplicated neonatal jaundice in healthy infants is unclear. A retrospective study 6 demonstrated that breast-fed infants were more likely to have bilirubin measured than formula-fed infants, and that bilirubin concentrations of >172 μmol/L were found in four times as many breast-fed compared to formula-fed infants. This selected concentration, an exact 10 mg/dL in mass units, was chosen to be below the concentration judged to be of clinical concern, but corresponding to clearly visible jaundice. Because not all infants were tested, there is a possible ascertainment bias, with breast-fed infants observed more closely for jaundice. The same publication 6 reported a prospective study of 115 white healthy term infants followed to 21 days of age, using transcutaneous bilirubin measurements, and demonstrated no significant overall difference in peak bilirubin, which occurred at three to four days of age in both breast- and formula-fed babies. However, breast-fed infants had a bimodal distribution, with a subgroup of 21% having peak results >224 μmol/L, a level that was not reached by any formula-fed babies. When compared with formula-fed infants, breast-fed infants had a longer duration of jaundice and serum bilirubin concentration did not return to day 1 values by day 21.
In the first few days of life, breast-fed infants tend to have a lower fluid and calorie intake than formula-fed infants. They become relatively dehydrated and cumulatively underfed and may develop breast (non)feeding jaundice akin to starvation jaundice, caused by increased enterohepatic circulation. 15 There has been much debate about the cause of the breast milk jaundice that is visible later, in the third week of life, in at least one third of breast-fed infants. Mature human breast milk, but not colostrum, has been shown to dramatically increase intestinal absorption of oral bilirubin in animal experiments. The factor mediating this has not been identified. 15 Earlier theories that breast milk contained a compound that inhibited glucuronidation of bilirubin or was the source of high concentrations of β-glucuronidase enzyme that re-hydrolyzed bilirubin glucuronides have been disproven. 16,17
In the vast majority of thriving breast-fed infants, breast milk jaundice is a harmless physiological phenomenon. Those few infants whose bilirubin concentrations reach treatment thresholds require therapy to prevent bilirubin encephalopathy, and investigation of possible genetic factors contributing to their jaundice.
Some interesting studies have investigated the genetic background that combines with non-genetic factors to predispose some infants to severe jaundice. Gilbert's syndrome, G6PD deficiency or hereditary spherocytosis alone do not predispose to neonatal jaundice. Combination of these factors with each other and with non-genetic factors, such as Coombs-negative ABO incompatibility result in a significantly increased likelihood of severe jaundice. 18,19 In Taiwanese neonates recently identified mutations in the organic anion transporter (OATP-2) have been implicated in unconjugated bilirubin uptake by hepatocytes, and increase the predisposition to jaundice. When combined with polymorphic mutations in the coding region of the UDPGT 1A1 gene, the infants' risk of severe jaundice was much increased. The subgroup of the same infants who were also breast-fed had a dramatically increased likelihood of peak circulating bilirubin of >340 μmol/L. 20,21
Bilirubin encephalopathy and its treatment
Free bilirubin is the only form in which bilirubin can cross the intact blood-brain barrier. A sick infant with high circulating concentrations of bilirubin-displacing metabolites has a relatively higher concentration of potentially neurotoxic-free bilirubin, while premature infants may have an impaired blood-brain barrier, allowing the passage of albumin-bound bilirubin. In clinical practice, the concentration of total bilirubin in neonates is usually equal to unconjugated bilirubin. Total bilirubin is used as an easily measured proxy for the concentration of free bilirubin, and hence the risk of neurotoxicity or kernicterus.
Kernicterus describes the yellow staining of subcortical nuclei found at postmortem in the brains of infants who died following severe hyperbilirubinaemia. Studies in animal models elucidated the toxic role of free bilirubin on the mitochondria of astrocytes and neurones. They also identified that the association constant of bilirubin with albumin varied with albumin concentration, and described the existence of a family of transporters, OATP, that remove bilirubin from the central nervous system. This helped in explaining the variability of susceptibility of neonates to bilirubin encephalopathy at similar circulating bilirubin concentrations. 22 When first identified in the 1950s, 30–50% of untreated babies with haemolysis owing to maternal Rhesus incompatibility developed severe unconjugated hyperbilirubinaemia and kernicterus. These infants were often asphyxiated, sick and delivered premature to avoid stillbirth. The risk of kernicterus appeared to increase dramatically with bilirubin concentration. Exchange transfusion was the first successful treatment for these infants, with a bilirubin intervention level of 342 μmol/L based on the methodology available at that time. 23
Relaxation of intervention levels
After introduction of screening of maternal Rhesus status with routine administration of anti-D, antenatal exchange transfusion if necessary and the development of early phototherapy for less-severely jaundiced infants, there was an impression that kernicterus had virtually disappeared. However, there was believed to be a spectrum of bilirubin toxicity. Early discharge made it more difficult to define the natural history of jaundice in well term infants to establish whether they had a higher bilirubin tolerance. On both sides of the Atlantic in the early 1990s, there was a re-evaluation of whether aggressive treatment of non-haemolyzing and less-severely jaundiced neonates was either necessary or justified. 23,24 It was recognized that the haemolyzing infants of the early studies had co-morbidities that placed them at increased risk, notably the presence of compounds that displace bilirubin from albumin, e.g. in acidotic, ketotic babies or those with renal failure. Premature sick infants were also more likely to have an impaired blood-brain barrier. A review of kernicterus in premature infant autopsies carried out from 1984 to 1993 found a low prevalence of 4%, although plasma bilirubin concentrations were often higher than those previously thought to place the premature infant at risk. This compared with a rate of 25% in the same institution prior to 1982. 25
In the UK, most neonatal units developed treatment protocols that used bilirubin measurement along with other risk factors, such as degree of prematurity, albumin concentration and day of life. Centile charts of bilirubin measurement plotted against age in hours were developed – the 'hour-specific nomogram'. 23 These charts were designed for use prior to early discharge to assess which infants were likely to develop significant hyperbilirubinaemia over the next few days. Just over half of the UK neonatologists surveyed felt that their treatment thresholds could safely be raised. 23 However, not all North American experts agreed. 26
Bilirubin as a cytoprotective agent
Studies on cultured rat hepatocytes, although at non-physiological high concentrations, demonstrated a cytoprotective effect of bilirubin, mediated by 'sacrificial oxidation'. This occurred with all forms of bilirubin, but was particularly marked for albumin-bound bilirubin that protected plasma and mitochondrial membranes from damage by removal of reactive oxygen species. Specifically in neurons, there was evidence of a protective effect at lower concentrations of free bilirubin, and a toxic effect at higher free bilirubin concentrations. The authors 27 suggested that there was a balance between the protective effects of albumin-bound bilirubin at low to moderate concentrations, and the damaging effects of free bilirubin at higher concentrations. Hepatocytes were more resistant to bilirubin toxicity than neurones and astrocytes. The specific areas of the brain that exhibit kernicterus are postulated to contain the most sensitive cells. The differences in cell susceptibility are attributed to differences in effective bilirubin removal mechanisms, by protein binding, metabolism and export transporters.
The re-emergence of kernicterus
Relaxation of criteria for treatment of jaundice coincided with earlier postnatal discharge, so that by the mid-1990s jaundice was the most common cause of re-admission of term infants in North America, 28 and case reports of kernicterus in 22 early discharged full or near-term infants caused great concern. Twenty-one of these cases were breast-fed, five were G6PD-deficient and many had other predisposing factors, such as ABO incompatibility or bruising. Sixty-one infants reported to the Pilot Kernicterus Registry had a median bilirubin concentration of 600 μmol/L at re-admission. Review of their records showed that the use of a predischarge bilirubin measurement, interpreted against an hour-specific nomogram, could have identified their increased risk. 29 In one centre in the UK, the incidence of hyperbilirubinaemia >340 μmol/L more than doubled from 2.4/1000 in 1991 to 5.5/1000 in 2001. 30
The American Academy of Pediatrics updated their clinical practice guideline on management of hyperbilirubinaemia in 2004. They recommended a universal risk assessment for severe hyperbilirubinaemia before discharge, based on one or more early bilirubin measurements assessed using an hour-specific nomogram.
31
An interactive version of this nomogram can be accessed on
A prospective study, supported by the British Paediatric Surveillance Unit, began in June 2003 with the remit of determining the incidence of severe (>510 μmol/L) unconjugated hyperbilirubinaemia. It was to document associated clinical and demographic variables and short-term outcome. 33 Their results reported after two years described the UK incidence of severe hyperbilirubinaemia as 7.1/100,000. 34 The majority of cases presented after the infant had been discharged, and over 80% were breast-fed. The mean presenting bilirubin was 580 μmol/L at 4.3 days of age. Risk factors included haemolysis, dehydration, infection and bruising. More than half were of non-white ethnic origin. Out of the 108 infants, 14 were identified having evidence of bilirubin encephalopathy, and three died. The two in whom a postmortem was carried out had kernicterus identified. The UK study thus confirmed the findings from North America and Europe. 34
Conjugated hyperbilirubinaemia in the neonate
In contrast to physiological unconjugated hyperbilirubinaemia, which requires careful monitoring but is common and usually benign, the presence of significant conjugated bilirubin always indicates pathology. As with many other homeostatic mechanisms, the bilirubin conjugation pathway has been untested until birth, and is immediately subjected to maximum load.
It is vital to identify the presence of conjugated bilirubin as early as possible. Conjugated hyperbilirubinaemia may result from infective, endocrine or genetic disorders, a selection of which are listed in Table 1. Many of the inherited causes of conjugated jaundice are considered very rare; however, there may be greatly increased incidence of particular recessive disorders, owing to consanguinity within extended families in specific geographical areas. The incidence of idiopathic neonatal hepatitis has steadily fallen as additional pathologies are identified. Early identification of conjugated hyperbilirubinaemia enables staged investigation, diagnosis and prompt commencement of medical (e.g. for septicaemia or galactosaemia) or surgical treatment, and thus reduces mortality and morbidity.
Causes of conjugated jaundice
The most important surgically treatable condition presenting in this way is extrahepatic biliary atresia, a rapidly developing condition in which the bile ducts are progressively obliterated, with an incidence of between 1 in 10,000 and 1 in 20,000. Bile drainage may be restored by early surgical removal of all damaged biliary extrahepatic tissue, followed by suturing a jejunal loop directly onto the raw hepatic surface exposed, allowing bile to drain from multiple tiny ducts directly into the bowel. The long-term outcome of this Kasai portoenterostomy procedure is determined by the age at which the operation is carried out. In one series, 73% of infants operated on before 60 days survived to 10 years, compared with 11% operated after 90 days of age, yet in the UK the majority of infants were not referred before six weeks of age. 35,36 This specialist surgery is only carried out in two to three units in the UK. If the Kasai procedure is not successful, a liver transplant is the only remaining option.
A great deal of work has been carried out to raise awareness of the importance of investigating prolonged jaundice. In the early stages before irreversible damage has occurred, infants with biliary atresia may appear well, and families may be inappropriately reassured that the cause is breast milk jaundice. Measurement of conjugated bilirubin is key to identification of such infants. The British Society for Paediatric Gastroenterology have produced a recent guideline for the staged investigation of prolonged jaundice, defined as beyond 14 days in term infants and 21 days in preterm infants. 37 They recommend analysis of total and split (direct or conjugated) bilirubin, and assessment of stool colour, and make no mention of urine bilirubin measurement. Laboratory measurement of conjugated bilirubin should be available within a local laboratory network.
Once conjugated hyperbilirubinaemia has been identified, the guideline recommends laboratory investigations that should be carried out in the next 24 hours, along with an ultrasound scan to determine whether a gall bladder is present. The list specifies plasma urea and electrolytes (including creatinine and bicarbonate), liver function tests, cholesterol and triglyceride, full blood count, including reticulocytes, blood group and Coombs test, clotting studies, blood and urine cultures and serology for hepatitis A, B and C plus IgM to rubella, toxoplasma, herpes and cytomegalovirus. To investigate endocrine and metabolic causes, the specification includes plasma free thyroxine, thyroid-stimulating hormone, cortisol, α1antitrypsin, urine organic and amino acids, a red cell galactosaemia enzyme screening test and a ward urine test for reducing substances. Their recommendation for plasma immunoreactive trypsin may be less necessary as a result of the UK rollout of newborn screening for cystic fibrosis, but a sweat test may still be required. Second stage investigations, including liver biopsy, are carried out on an individualized basis, depending on clinical assessment and the results of the first-line tests.
Several strategies have been considered to reduce the age of identification of conjugated hyperbilirubinaemia. These include a proposal to drop the age of the well baby check from six to four weeks, 35 or additional analyses on the newborn screening sample, such as unconjugated and conjugated bilirubin by dry-slide technology 38 or conjugated bile acids using a tandem mass spectrometry. 39 At the present time, the recognition of prolonged jaundice by staff in the community remains the first indication of the development of conjugated jaundice. For each infant institution of specific treatment to avoid life-threatening episodes can only occur once a diagnosis has been confirmed, and an important first step is the demonstration of conjugated hyperbilirubinaemia.
First-line assessment of jaundice
Transcutaneous monitors
Circulating bilirubin in infants with physiological jaundice peaks at three to four days of age, when almost all babies are at home. In this low-risk population, sample collection, transport and access to laboratory results can seem to be an invasive and cumbersome process. There is thus a role for point-of-care testing (POCT). Portable transcutaneous bilirubin monitors use reflectance densitometry to quantitate yellow skin colour and are widely used in the initial assessment of potentially jaundiced infants. Thirty-two separate studies in infants from different population groups concluded that transcutaneous readings are correlated with plasma bilirubin. 40 The equation relating the two is population and bilirubin method dependent. For meters such as the Minolta Airshields JM102, the regression equation must be established by each centre for its own population and bilirubin methodology. For more recently marketed meters, such as the Minolta Airshields JM103 and the SpectRx BiliCheck, additional wavelength measurements and algorithms make a conversion and display calculated bilirubin in μmol/L.
For all meters the scatter has been demonstrated to be wide. In a study of 303 full-term babies using the Minolta Airshields JM102 compared with a laboratory diazo method (Roche Cobas Integra, Roche Diagnostics GmbH, Mannheim, Germany), bilirubin results spanned <50 to >400 μmol/L, with almost four-fifths between 100 and 250 μmol/L. From the regression line between the two methods, the 95% confidence limits (CI) of a transcutaneous measurement was estimated as ± 88 μmol/L. 41 A new generation of transcutaneous instrument uses more sophisticated wavelength filtering and algorithms to correct for skin colour and convert the raw reading to μmol/L of bilirubin. Despite this, their agreement with routine laboratory measurements shows equally wide CIs as the first generation meters. 42–44 For example, a three way comparison of laboratory total bilirubin (Roche Hitachi 911 Diazo method, Roche Diagnostics GmbH, Mannheim, Germany), Minolta Airshields JM102, and the new generation SpectRx BiliCheck was carried out on a population of 64 preterm and term neonates with laboratory bilirubin ranging from 50 to 350 μmol/L. This showed 95% CIs estimated from a difference plot of the transcutaneous method versus laboratory bilirubin of ±66.7 μmol/L for the Minolta Airshields JM102 and ±66.4 μmol/L for the SpectRx BiliCheck. 42 Thus, plasma bilirubin cannot be accurately predicted from a transcutaneous reading.
It is reported that the variability may be related to site of sampling, skin colour, degree of prematurity and rate of change of plasma bilirubin. Transcutaneous measurements cannot be used to monitor infants undergoing phototherapy, and their major role is to replace simple visual assessment to non-invasively screen out infants who do not require a plasma bilirubin measurement. When this was carried out on the first or second day of life, prior to discharge, it was shown not to reduce the number of laboratory bilirubin requests, but did reduce the number of babies re-admitted because of hyperbilirubinaemia. 45 There is some speculation in the literature as to whether the degree of penetration of bilirubin into cutaneous tissues might be a better measure of the risk of penetration into brain compared with plasma bilirubin, but there are no data to support this. 41
Precision studies for transcutaneous monitors used cuvettes containing bilirubin solutions, or a small number of repeat measurements on an infant over a short time-period. 40 The reported studies have generally been carried out as part of a research protocol on a limited number of subjects. It is possible that the CIs of the correlation with plasma bilirubin could be even wider in routine practice. Because of the nature of the measurements, direct by on the baby's forehead or sternum, internal quality control (IQC) is limited to electronic checks, and there is no external quality assurance (EQA) available.
The number of publications on transcutaneous measurements in the last 10 years dwarfs the literature on laboratory methods, reflecting the desire to use this technique. Although there is no doubt that sick, premature and significantly jaundiced infants continue to require blood sampling and bilirubin measurement, there is a massively larger population of infants without perceived risk factors, who require assessment of whether or not they have jaundice significant enough to need intervention. It is these infants, who initially need a one-off rapid result, either prior to discharge or when at home, who are the market for transcutaneous monitors. A numerical value is recorded, rather than a subjective visual assessment. This may be particularly helpful in repeat measurements on the same infant. As with all POCTs, it is essential that all staff carrying out these measurements are adequately trained, and that there is an ongoing programme of audit and revalidation. This may be an area where there is little involvement or communication with the local laboratory. At the very least laboratory staff should be aware of the existence and extent of transcutaneous measurements in their area.
Blood gas and electrolyte point-of-care testing analysers
POCT has become available for whole blood bilirubin by the addition of a bilirubin channel to the gas and electrolyte analysers widely available in neonatal units. Capillary samples are measured using spectrophotometry with multiple wavelength readings and algorithms to correct for haemoglobin, fetal haemoglobin and lipaemia. Comparisons with wet 46,47 and dry slide 48 Diazo laboratory methods for neonates have shown an insignificant bias over a wide range of bilirubin concentrations, albeit with a wide scatter.
Samples from IQC and EQA schemes can be analysed in the same way as patients' samples, and sites using these analysers should have them enrolled in an appropriate EQA scheme.
Alternatives to bilirubin measurement
Carbon monoxide is produced in equimolar concentration to bilirubin when haemoglobin is oxidized (Figure 1), and its measurement in breath has been suggested as an alternative means of early identification of those infants who are at risk of hyperbilirubinaemia because of increased haemolysis. 5,49 As this measurement only identifies bilirubin production and not disposal, its use is likely to be limited to a small cohort of high-risk infants, rather than applied as a widespread screening tool for significant jaundice.
Measurement of serum bilirubin
Two detailed methodological reviews published in the early 1990s considered reference and routine methods for total and fractionated bilirubin. 50,51 Today, reference methods based on high-performance liquid chromatography (HPLC) have limited availability for most clinical laboratories.
Free bilirubin
Attempts to measure free bilirubin have resulted in widely varying results, even in a research setting. Dilution, essential for the analysis, appears to perturb the equilibrium between free and albumin-bound fractions, and to make accurate assessment of free bilirubin virtually impossible. 52,53 Complex equations have been developed to relate free and total bilirubin to brain bilirubin uptake, with terms allowing for potential displacement of bilirubin from albumin by a variety of other compounds, and the integrity of the blood-brain barrier. 54 This model fails to yield expected values for brain uptake when total bilirubin is used. 55 For the foreseeable future, measurement of total bilirubin, and algorithms incorporating other risk factors, will continue to be used for decisions on treatment for jaundiced neonates.
Total bilirubin
The laboratory total bilirubin methods described in earlier reviews–diazo dye binding, spectrophotometry or oxidation by bilirubin oxidase or by potassium ferricyanide 56 –still reflect the practice of laboratories participating in the neonatal bilirubin UK NEQAS in 2008, with over 60% of laboratories using the diazo methods, 26% oxidation methods and 10% dry-slide technology. 57
The main change in provision of bilirubin analysis, at least in the UK, has been the availability of POCT, and a move away from in-house methodology to manufacturer's kits. These changes have been driven by reviews of laboratory workflow and automation, harmonization across laboratory networks and, within Europe, by the regulatory demands of CE (Conformité Européenne) marking, which mean that the manufacturer's performance specification is invalidated by any in-house modification of a commercial kit. The procedure for obtaining a CE mark is too great a task for most laboratories to take on for an in-house method, if commercial kits exist.
Commercial diazo methods now commonly use dichlorophenyl diazonium substrates. These substrates have relatively long-term stability, and can thus be marketed as ready to use solutions, and kept on-board analysers in volumes suitable for use over days or weeks. Details of methodology are to be found in manufacturers' literature. It should be noted that there may be frequent changes of formulation, and that different formulations may be supplied by the same manufacturer.
A major problem in many diazo dye-based bilirubin assays is haemoglobin interference. In a detailed study of the Malloy Evelyn method (where diazo reagent is prepared fresh from sulfanilic acid and sodium nitrite, and bilirubin is solubilized in methanol), Shull 58 demonstrated negative interference because of oxidative destruction of bilirubin before diazotization, linked to conversion of oxyhaemoglobin to haematin with release of hydrogen peroxide. The interference was dependent on the length of the assay preincubation period, before addition of diazo reagent, and could be reduced by addition of ascorbic acid. In these very specific reaction conditions, he found little direct spectral interference of haemoglobin. In contrast, using the same experimental technique, he identified that in a Jendrassik-Grof method (where diazo reagent is made freshly from sulfanilic acid and sodium nitrite, and caffeine is used as the solubilizer), interference is caused by direct spectral interference from oxyhaemoglobin, as well as from oxyhaemoglobin-mediated breakdown of bilirubin during and after diazotization. The net interference could be positive or negative, and correction by ascorbic acid was variable, depending on sample dilution. 59
It should be apparent from the above that haemoglobin interference is exquisitely sensitive to variation in reagents, dilutions and reaction timing. 58,59 There has been a recent concern that the automated bilirubin methods from several major suppliers exhibit unacceptable haemolysis interference for neonatal use. Users of automated kit methods must remain vigilant to product updates and changes in formulation that may affect interference. Although manufacturers provide a statement on haemolysis interference and/or provide references, the user should confirm that this relates to the method and the kit actually in use. The few references in the peer-reviewed literature to this interference 60 may be quoted by manufacturers, but may not correspond exactly to the reaction conditions in the marketed kits. There is no substitute for carrying out in-house interference studies on real patient samples across the full range of bilirubin concentrations found in neonates.
When new analysers are introduced, in-house assessment of total and direct or conjugated bilirubin assays for neonatal use is required, especially with regard to haemoglobin interference. For analysers with open channel capability, it may be possible to use an alternative method if the manufacturer's standard method shows an unacceptable analytical range or interferences. Oxidation methods, such as that described by O'Leary et al. 56 have been demonstrated not to suffer from interference up to a haemoglobin concentration of 5.0 g/L. As for diazo methods, it is recommended that laboratories confirm this in-house.
Dry-slide technology may be based on either diazo dye-binding or spectrophotometry, depending on the intended use of the slides. Very few laboratories use spectrophotometric measurements on a bilirubinometer, although this may potentially be less sensitive to haemoglobin interference than some wet chemistry diazo methods. 61
Conjugated and direct bilirubin
Conjugated bilirubin is the sum of bilirubin mono- and di-glucuronides, plus any other minor conjugates. Direct bilirubin is defined only in the context of diazo dye binding methodology. It describes that part of total bilirubin that reacts with diazo dye rapidly and in the absence of a compound added to solubilize unconjugated bilirubin, usually referred to as an accelerator. It is used as a conveniently measured assessment of conjugated bilirubin, but the relationship between the two will vary depending on the exact reaction conditions. 50
Semi-quantitative assessment of bilirubin excretion is available as a component of multiple reagent strips for urinalysis. This could, in theory, be used in neonates with prolonged jaundice as a first-line screen for conjugated bilirubin. There is a complete absence of any assessment of their use in this situation, however, in adult populations they have been demonstrated to fall far short of 100% sensitivity. 62–64
Laboratory methods for measurement of direct or conjugated bilirubin have not changed greatly over the last 20 years. An enzymatic method using bilirubin oxidase at pH 5.5 in the presence of sodium fluoride and N-acetylcysteine inhibitors to prevent reaction of unconjugated and δ-bilirubin has been described, but appears to be widely used only in Japan. 65,66 This method gave results in neonates that did not agree with either HPLC or diazo results. Mirroring the situation for total bilirubin, in the UK there has been a move away from in-house to commercial methods, standards and IQC materials. The great majority of laboratories participating in the UK NEQAS neonatal bilirubin scheme use diazo-based methods. The remainder use spectrophotometric measurement, usually employing dry-slide technology. 57
Optimization of commercial diazo methods means that the residual proportion of unconjugated bilirubin reacting in the direct reaction has fallen from the 5 to 15% often quoted in textbooks. It is therefore essential for laboratories to quote a reference range and detection limit appropriate to their particular method, 67 based on in-house studies if necessary.
Calibration of bilirubin assays
Total bilirubin
Previous reviews highlight the particular problems of bilirubin calibration. 50,51,68 The spectra of the different bilirubin species are matrix-dependent, as is the absorptivity of bilirubin diazo conjugates. It is important that working standards for routine methods show traceability to reference standards of unconjugated bilirubin in human serum base. 69 SRM 916a, the second batch of bilirubin calibrator prepared by the USA National Institute of Standards and Technology (NIST), defines molar absorptivity of bilirubin in caffeine reagent at 432 and 457 nm, and of alkaline and neutral azo-pigments at 598 and 530 nm. It was shown to give results almost identical to SRM 916 by a panel of North American laboratories using a candidate reference diazo method, 70 based on the Jendrassik-Grof principle, with and without alkalinization. By assessing molar absorptivity in caffeine reagent, which disassociates bilirubin from albumin, they removed the matrix dependency of the molar absorptivity.
Manufacturers of commercial bilirubin methods should establish traceability of their working calibration standards to SRM 916a. However, Apperloo et al. 71 demonstrated that while SRM 916 gave good agreement when analysed by wet and dry chemistry methods, adult human samples showed substantial over and under estimation, respectively, when compared with the reference diazo method. This again emphasized the effect of matrix on measurement of the complex mix of physiological bilirubin species found in circulating plasma.
Direct or conjugated bilirubin
A commercial source of bilirubin mono- or di-glucuronide is not available. Assays are therefore routinely calibrated using either synthetic ditaurobilirubin or unconjugated bilirubin at a pH that enables it to react fully. A North American quality assurance scheme distributed a sample containing >300 μmol/L of unconjugated bilirubin in a human serum base, with no conjugated bilirubin added. The results demonstrated little cross-reaction in direct or conjugated bilirubin assays, with the worst method giving a cross-reactivity of 5%. This represented a large increase in specificity of methods since its previous evaluation, 10 years previously. 72
Quality assurance
A North American EQA scheme recently highlighted method disparities that could be attributed to differences in the matrix of the circulated samples. 72,73 Large method-related differences were found, especially at elevated bilirubin concentrations, when high concentrations of unconjugated bilirubin were added to a bovine serum base. An additional complication in this College of American Pathologists (CAP) survey was an apparent problem with specific method groups, that was most marked for Vitros dry-slide technology. This was the result of methods from the same manufacturer, but with a different chemical basis, being classed together. The same laboratories returned very different results depending on whether an identical sample was distributed as part of a general chemistry or neonatal bilirubin scheme. The Vitros neonatal bilirubin dry slide uses spectrophotometry to measure unconjugated and conjugated bilirubin and calculates the sum, whereas the total bilirubin slide uses a diazo-based reaction.
The authors concluded that occasional issue of an elevated bilirubin sample prepared by spiking human serum with pure unconjugated bilirubin, and establishing its concentration by a reference (diazo-based) method 70 was necessary to estimate the accuracy of routine methods, and to identify problems with specific manufacturers' calibration material. Use of this sample would not introduce additional variables related to sample matrix and non-physiological bilirubin species.
Interpretation of results
Several studies have identified the 95th centile of bilirubin in healthy neonates during the first week of life. A recent estimate is 259–301 μmol/L in a predominantly breast-fed population. However, risk assessment for an individual infant must take into account the hour of life when the bilirubin was sampled, its rate of increase and other factors such as risk factors for haemolysis. 74 Readers should also refer to their local neonatal unit's own guidelines.
Assessment of measured bilirubin against a percentile plot for hour of life, and the rate of change with time imposes new precision requirements on the laboratory method(s). According to the American Academy of Pediatrics guideline, a rate of rise >4.3 μmol/L/hour or 103 μmol/L/day should be a cause for concern, 31 which has clear implications for the precision and accuracy required for laboratory methods to identify a true biological change.
Two illustrative cases
Evolution of jaundice in two patients is shown in Figure 3. In both cases, over the time period shown, analyses were carried out by laboratories using different methodology.
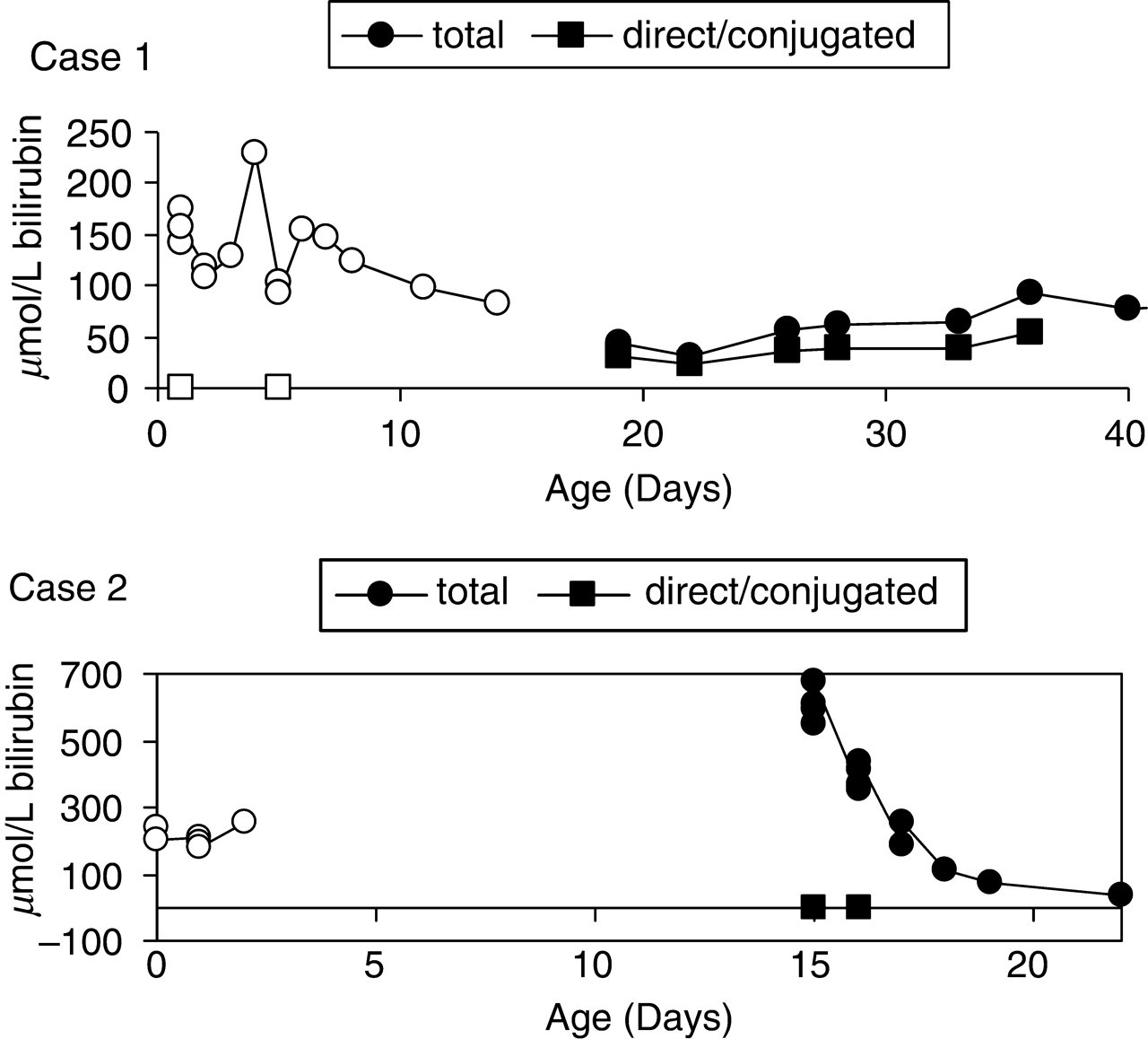
Two Illustrative cases. Changes in bilirubin methodology because of samples referred to different laboratories are indicated. For each patient, results from the first method are shown in open symbols, and the second in closed symbols. The points shown on the X-axis for direct/conjugated bilirubin at days 1 and 5 in case 1 and days 15 and 16 in case 2 were below the detection limit for the method used
Case 1 was a girl born at 30 weeks gestation with intrauterine growth retardation. She initially had physiological neonatal jaundice treated by phototherapy. After her initial jaundice had resolved she had multiple infections and was fed by total parenteral nutrition. Monitoring of total and direct bilirubin from day 19 onwards identified steady development of cholestatic jaundice, at total bilirubin concentrations that were at or below the limit of clinical detection of jaundice. After appropriate investigation, she was diagnosed as having extrahepatic biliary atresia.
Case 2 was an infant of Asian origin born at 39 weeks gestation, who developed jaundice in the first 24 hours of life. He was treated with phototherapy on days 2 and 3, and discharged on day 4. He presented to the Emergency Department of a different hospital on day 19 with severe jaundice owing to unconjugated hyperbilirubinaemia, requiring exchange transfusion and further phototherapy. He was shown to have glucose-6-phosphate dehydrogenase deficiency.
Case 1 demonstrates the laboratory requirement for accurate and precise measurement of total and conjugated bilirubin when the total bilirubin concentration is around 50 μmol/L, whereas Case 2 demonstrates the need to measure a total bilirubin of 700 μmol/L, an accurate low conjugated bilirubin in the same sample, and the ability to measure both total and conjugated bilirubin in samples from an infant with in vivo haemolysis.
Summary
The laboratory must provide a routine and emergency service for the measurement of total and conjugated bilirubin in neonates. Analysis of total bilirubin must cover the concentration range and treatment thresholds encountered in the whole neonatal population. This includes the extreme premature infant on day 1 or day 2 of life, who may require phototherapy at a plasma bilirubin of <100 μmol/L, through to the re-admitted term infant with severe hyperbilirubinaemia of >500 μmol/L. Infants whose hyperbilirubinaemia is the result of in vivo haemolysis require that the assay does not suffer from interference because of haemolysis. Methods must be of acceptable precision, capable of assessing the rate of change of bilirubin concentrations, either with time or in response to phototherapy, rehydration or exchange transfusion.
The assessment of conjugated bilirubin must be able to determine whether this is significantly increased. Thus, the cross-reactivity of the method at all concentrations of unconjugated bilirubin must be known, along with the reference range expected in jaundiced infants without cholestasis.
Participation in an EQA scheme, such as UK NEQAS for Paediatric Bilirubin 57 or the CAP surveys in the USA, 73 can give useful information on the relative accuracy and precision of different methods, and some information on cross-reactivity of unconjugated bilirubin and haemolysis interference. By comparing the submitted data with the EQA scheme's limits of acceptable performance, a decision may be made either to modify methods (a less common option) or to select an alternative method for neonatal bilirubin analysis.
In the common situation where the infant has had bilirubin measured in a number of different health-care settings, there must be an ability to interpret changes with time, that is not distorted by changes in the methodology used. There is a strong argument for harmonization of assays provided from locations from where the same infant may have successive samples referred (e.g. maternity unit, primary care, local or regional paediatric unit). With the development of regional laboratory networks, this may be more likely to occur, however, either the standard bilirubin methodology chosen for adult samples must be suitable for neonatal analysis, or a separate neonatal bilirubin method must be selected. Much smaller numbers of direct or conjugated bilirubin analyses are requested, and it may be sufficient to have these available from one laboratory in a local network, provided appropriate handling and transport links are in place.
However, bilirubin assays are provided, it is essential that the laboratory has an ongoing dialogue with the teams caring for jaundiced infants to ensure that there is a shared understanding of the performance of the near patient and laboratory methods used, and any differences between them, and the concentration levels or time-related changes in concentration that are the basis of treatment thresholds.