
Abstract
The diffuse endocrine system (DES) includes a wide range of secretory cells that may be the source of tumours. Gastroenteropancreatic endocrine (GEP) tumours arising within the DES secrete a variety of peptides and amines that are found in the circulation and are responsible for the syndromes associated with these tumours. In this review, the most common tumours of the GEP tract are outlined and the circulating products of these tumours identified. Where differential diagnosis is difficult these points are addressed. The peptides most commonly secreted by GEP neuroendocrine tumours are identified and described and their biological activities are discussed. Current methods available for measurement of these peptides are described. Attention is drawn towards molecular specificity where appropriate, as many pancreatic and gut peptides fall within families which show considerable homology, such as the tachykinin family or the glucagon family. Other peptides such as gastrin circulate in multiple molecular forms. This homology and diversity may cause difficulty in the interpretation of peptide measurements in the clinical situation if assays are not specific.
The diffuse endocrine system
Many hormones and bioactive peptides originate in what is called the diffuse endocrine system (DES) rather than, or in addition to, originating in discrete endocrine organs. The DES is a collective name for the endocrine cells scattered throughout the gastrointestinal mucosa, cells of endodermal origin including the pancreas, thyroid, urogenital tract, respiratory tract and, in addition, myocytes in the heart atria. All cells throughout the body which have the potential to produce peptides and bioactive amines that may act in an autocrine, paracrine, endocrine or neurocrine fashion are candidates for inclusion in the DES. It is believed that endocrine tumours of the gastrointestinal (GI) tract and pancreas arise from these cells. The products of these cells in tumour pathology and diagnosis are the focus of this review.
A minimum of 15 different cell types have been identified 1,2 which produce at least 33 peptides and biogenic amines. 3,4 In the mid-1960s, Pearce 5 postulated that these cells arise from a common embryological tissue originating from the neural crest. This theory found evidence from the common ability of such cells to take up amine precursor molecules and to undertake decarboxylation of these substances, which resulted in the production of peptide hormones and biogenic amines (Amine Precursor Uptake Decarboxylation) and was known as the APUD theory. With increasing evidence that endocrine cells of the DES arise from stem cells of the pancreas and GI tract, the APUD theory has lost its credibility. However, the ability of these cells to take up amine-precursor molecules and to undertake decarboxylation remains to be valid.
Neuroendocrine tumours
Classification (WHO) of neuroendocrine tumours of the gastroenteropancreatic system
There has been considerable debate regarding the nomenclature of neuroendocrine tumours (NETs) over the past decades. Although these tumours were first described in 1888 by Lubarsch, 6 when he observed two patients with ‘little carcinomata’ in the distal ileum, the term carcinoid (karizinoide) was not introduced until 1907. 7,8 Later, when Masson 9 discovered similar tumours throughout the GI tract and in other sites, the term carcinoid was used to encompass these also, regardless of their site of origin. In 1963, Williams and Sandler, 10 influenced by the concept of the APUD theory, classified carcinoids into fore, mid and hind gut groups disregarding the very mixed cell types included in foregut. This terminology has remained in common usage. In 1960, the World Health Organisation (WHO) published a classification for carcinoids of the DES, which included tumours of the pancreas, medullary thyroid tumours, small cell lung tumours and Merkel-cell tumours. It also subdivided into the carcinoid group as enterochromaffin cell carcinoids, gastrin cell carcinoids and other carcinoids. 11 This did not clarify the situation and caused confusion between pathologists and clinicians. A second WHO classification was published in 2000 that replaced the terms carcinoid and neuroendocrine with endocrine. 12 In this classification endocrine tumours are identified according to their site of origin and then classified further according to growth pattern; benign, uncertain (benign and low grade), low-grade malignant and highly malignant.
Clinical features associated with NETs
Pancreatic
Why the pancreas is such a relatively rich source of endocrine tumours has remained unanswered. Pancreatic endocrine tumours may be sporadic or part of the multiple endocrine neoplasia type I (MEN1) autosomal dominant disease. Pancreatic tumours that are associated with MEN1 tend to be smaller than sporadic tumours, are frequently quite indolent, may be multi-focal and may secrete several hormones and peptides from one tumour or from several different tumours. As tumours may be very small they may be difficult to visualize. Sporadic pancreatic endocrine tumours are more commonly malignant and may be aggressive.
Pancreatic endocrine tumours are named for the hormone or peptide that they produce, giving rise to a syndrome, or alternatively for the peptide which is found in high concentrations in the circulation or in the tumour. They fall into three groups. First, those that present with small tumours producing very active peptides. These include insulinomas, gastrinomas and tumours secreting vasoactive intestinal peptide (VVIPomas). Secondly, those that present with less overt syndromes and show clinical symptoms only when the tumour is more advanced, for example glucagonoma. And thirdly, those which present with problems associated with tumour bulk and are diagnosed as endocrine often only because the patient continues to survive beyond the time expected with exocrine pancreatic cancer, for example somatostatinoma and tumours secreting pancreatic polypeptide (PPomas).
Pancreatic NETs may produce one or more peptide and the products may be in numerous molecular forms of incompletely processed peptides and alternatively processed products. With the exception of insulinomas, the majority of these tumours are malignant or have the potential to become malignant. They are almost invariably slow growing with a low proliferative index. 13,14 However, most of those that are malignant have metastasized within the abdominal cavity by the time of diagnosis.
Surgical excision of benign tumours is curative. Excision of the primary lesion for malignant tumours and/or debulking, followed by chemotherapy, 15 hepatic artery embolization where appropriate and somatostatin analogue therapy with or without the addition of interferon α and/or end-organ targeted therapy usually contains systemic effects and malignant progression for a considerable period of time. This may extend to decades in many patients. 16
Insulinoma
Insulinoma was the first pancreatic endocrine tumour to be described 17,18 and is the most common (1–2 per 1,000,000 per year). Insulinoma presents with palpitations, sweating, pallor, anxiety or personality changes and classically with hypoglycaemic attack, especially in the early morning or after a prolonged fast. The main differential diagnosis is insulin or sulphonylurea abuse, which is uncommon. Other causes of hypoglycaemia may include Addison's disease, hypopituitarism or alcohol-induced hypoglycaemia. Insulinoma remains difficult to diagnose in some patients as insulin secretion from the tumour is irregular and a 1–7 y delay in diagnosis is recorded. 19 A small tumour (<1 cm in diameter) or multiple micro-tumours secreting insulin within the reference range may be difficult to visualize radiologically and insulinomas frequently show negative somatostatin receptor scintigraphy. 20,21 Diagnosis may be confirmed during a 72-h fast, under controlled conditions, where serial blood samples are taken for blood glucose. Insulinoma is slightly more common in women than in men and tumours are usually solitary (85%). Because the majority are benign, cure may be achieved by surgery. Approximately 50% of malignant insulinomas are multi-hormone secreting. Only 2–4% of insulinomas are within the MEN1 syndrome.
Gastrinoma
Gastrinoma, first described by Zollinger and Ellison, 22 is the second most frequent pancreatic endocrine tumour and is a little less common than insulinoma. The slight majority are malignant and about half of these are aggressive. 23 More than 50% of gastrinomas arise in the pancreas, the duodenal wall being the second most common site. 24 Gastrinoma associated with MEN1 is more commonly located in the duodenum and these tumours tend to be small and less aggressive. Gastrinoma secretes gastrin that stimulates excessive gastric acid production resulting in ulceration that may occur in the stomach, duodenum and jejunum (the Zollinger-Ellison syndrome). A significant number of patients with recurrent peptic ulcer in the absence of Helicobacter pylori infection have gastrinoma. Unfortunately, a significant number of these patients remain undiagnosed for some time and are treated with high-dose proton pump inhibitors to control acid secretion, which masks the syndrome and permits the tumour to progress. The classical symptom is peptic ulcer. However, gastrinoma frequently (about 50% of cases) presents with diarrhoea and many patients will also have malabsorption. Occasionally gastrinomas arise that predominantly secrete C-terminally extended gastrins and do not exhibit the Zollinger-Ellison syndrome associated with gastric hyperchlorhydria.
VIPoma
VIPoma is rare (about 0.2 per 1,000,000 per year). However, it is one of the tumours that produces a profound syndrome and as a result is frequently diagnosed at an early stage even in the face of such rarity. VIPoma was originally described by Verner and Morrison in 1958 25 and produces a syndrome of watery diarrhoea, hypokalaemia and achlorhydria (WDHA). The majority of these tumours arise in the pancreas in adults, but about 10–15% occur in the ganglionic chain, most commonly in the adrenal medulla. The cardinal feature of VIPoma is profuse watery diarrhoea which may be intermittent at first, but rapidly becomes unrelenting and may reach a volume of 20 L/d. The majority of patients also complain of abdominal pain and weight loss. Hypokalaemic acidosis occurs as a result of bicarbonate and potassium loss across the bowel mucosa. Hypercalcaemia may occur due to the direct action of VIP on bone. Although gastric achlorhydria occurs only in about 50% of patients, hypochlorhydria is usually present. Flushing occurs in approximately 20% of VIPoma patients, which may cause some confusion with classical midgut carcinoid syndrome (MGC). 26 VIP-producing tumours also occur in childhood as ganglioneuroma and neuroblastoma. These tumours present at an early age most frequently between 2 and 4 y. 27
Glucagonoma
Glucagonoma is also rare (0.1 per 1,000,000 per year) and because the syndrome is not as overt as those described above, patients often present at a later stage with extensive metastatic disease. Glucagonoma syndrome is characterized by necrolytic migratory erythema that most often occurs around the thighs and perineal area, although the rash can be widespread. Because of this classical rash, glucagonoma is the only pancreatic endocrine tumour that may be diagnosed by clinical examination. The raised glucagon concentrations that occur in these patients produces a catabolic state resulting in weight loss accompanied by diabetes. In addition, these patients are prone to deep venous thrombosis that may be a significant cause of death. Many suffer from depression. 28,29
Somatostatinoma
Somatostatinoma is also rare (0.1 per 1,000,000 per year). About 60–70% of somatostatinomas occur in the pancreas and of these almost all present with extensive metastatic disease. Outside the pancreas, somatostatinomas also occur in the duodenum and in the hindgut. Duodenal tumours tend to be small and are frequently associated with MEN1. Circulating concentrations of somatostatin are high with pancreatic tumours, and the widespread inhibitory property of somatostatin leads to mild diabetes, diarrhoea-steatorrhoea and gallstones. 30 Duodenal tumours are further discussed later in the text.
PPoma
PPoma may be the most common pancreatic endocrine tumour but is non-functioning and is diagnosed as a result of tumour bulk rather than from other symptoms. It may remain undiagnosed in the majority of cases. PPoma has no associated syndrome. It is not uncommon for patients with PPoma to be referred from terminal care units when exocrine pancreatic carcinoma had been wrongly diagnosed. If tumour bulk can be managed then these patients may survive for some years even with very extensive hepatic disease. Many PPomas may produce additional peptides that have not been identified to date. Proteomics may shed light on this in the future. In addition to the tumours that appear to secrete only pancreatic polypeptide (PP), the majority of all pancreatic endocrine tumours and about one-third of those arising in the GI tract also produce PP and secrete significant concentrations into the circulation. 31
Rare pancreatic endocrine tumours
Other extremely rare pancreatic endocrine tumours include glucagon-like peptide 1 (GLP1)oma, glucagon-like peptide 2 (GLP2)oma, neurotensinoma, calcitoninoma, ACTHoma, cholecystokinin (CCK)oma and more. All of these may present as defined tumours or the above peptides may be co-secreted in addition to the existing tumour syndromes. In our experience, about 30% of gastrinomas secrete at least one other peptide in addition to PP. These multihormone-producing tumours are indicative of more progressive disease. Four to five percent produce ACTH and these have a poor prognosis. 32
Endocrine tumours of the gut
Endocrine tumours of the gut comprise about two-thirds of tumours of the gastroenteropancreatic endocrine (GEP) tract. They most commonly occur in the midgut; one-third of this group arise in the appendix. Appendiceal tumours cause appendicitis and are removed at surgery. They recur very infrequently, cure being obtained by surgery, except for those presenting with tumours greater than 2 cm in diameter and those located at the rim of the appendix. 33,34 The few that recur give the classical symptoms of midgut tumours.
Endocrine tumours of the stomach
Endocrine tumours of the stomach or gastric carcinoids are more common than originally thought, and may comprise as many as 25% of all endocrine tumours of the GI tract. They fall into three groups. Type I is associated with chronic atrophic gastritis. 35 There is an increased incidence in patients with pernicious anaemia. They are often multi-focal and small and tend not to metastasize. Type II is associated with MEN1 and gastrinoma. Type I and II tumours are mostly comprised of enterochromaffin-like (ECL) cells. In types I and II, circulating concentrations of gastrin are significantly raised. Type III are sporadic gastric carcinoids. 36 They tend to be solitary and may be aggressive. They do not secrete gastrin and circulating gastrin is not raised.
Endocrine tumours of the duodenum
Endocrine tumours of the duodenum may be small, are usually solitary and are frequently associated with MEN1. 37 They may be benign or, if malignant, very slow growing. They occasionally present with obstruction. They most commonly secrete gastrin or marginally elevated concentrations of somatostatin. Only about half of MEN1 tumours secrete chromogranin A (CgA) or the breakdown products of CgA. As duodenal tumours are small they may be difficult to visualize using radiological methods. MEN1 duodenal tumours are therefore difficult to diagnose.
Endocrine tumours of the midgut
Endocrine tumours of the midgut (jejunum, ileum, proximal colon) are the largest single group of endocrine tumours of the DES. They comprise 25% of the total. Necropsy studies indicated that these tumours are frequently seen incidentally at postmortem and may in fact be quite common but probably irrelevant. 38 In the largest studies, of those that were diagnosed in vivo, one-third are diagnosed as an incidental finding. 39,40 When symptoms do occur, the most common is abdominal pain, which may predate diagnosis by several years. Approximately 50% of patients present with intestinal obstruction. Tumours are removed at surgery and although no local spread may be observed in a significant number, these apparently cured patients should be followed up annually as disease frequently recurs. The remaining 15–18% of tumours present with metastatic disease and typical carcinoid symptoms, specifically flushing (94%) and diarrhoea (78%). Carcinoid syndrome is reported in only about 10% of patients, when in addition to flushing and diarrhoea there may be wheezing, bronchoconstriction, oedema, cyanosis and right-sided heart valvular fibrosis (carcinoid heart disease). Carcinoid disease and in particular carcinoid syndrome is accompanied by excessive serotonin production and secretion. In carcinoid disease, substance P (SP) is thought to contribute to the vasodilation and flush, whereas neurokinin A (NKA) may be associated with diarrhoea and increased gut motility.
Endocrine tumours of the distal colon and rectum
Endocrine tumours of the distal colon and rectum produce few symptoms and are difficult to diagnose. Although they may be present for years before presentation, metastases are relatively rare (4–18%). 41 The majority of tumours are solitary and <1 cm in diameter. Those presenting with tumours of size >1 cm are more likely to have metastases. Some rectal carcinoid tumours produce serotonin, but this is uncommon. More often glicentin, PP and peptide YY (PYY) are produced and may show a small rise in the peripheral circulation. CgA is raised in about 70–80% of cases. 31
Among the rare sites for endocrine tumorogenesis, tumours may arise in Meckel's diverticulum, the most common developmental abnormality of the GI tract, which contains ectopic tissue from stomach and pancreas. About one-quarter will have metastasized at presentation and some three-quarters progress to metastatic disease eventually. They most frequently secrete CgA and gastrin. 42 Endocrine tumours have also been identified in the oesophagus, 43 pancreas, biliary tract or gall bladder, 44 liver, 45 thymus and ovaries. 43 These tumours are all extremely rare. CgA is the best general marker for these tumours. Tumours of the oesophagus may secrete VIP.
Endocrine tumours of the respiratory tract
Although outside the GEP tract, endocrine tumours of the respiratory tract are as common as tumours of the midgut and require a mention. They most commonly present early, with symptoms of obstruction of the airways, are usually solitary and frequently small. They are managed by surgical resection, which may result in cure much more frequently than is the case with MGC. Occasionally they do present at GI and GEP NET clinics with secondary disease and carcinoid syndrome. The symptoms include flushing, diarrhoea, haemodynamic imbalance, wheeze, lacrimation and carcinoid heart disease. Advanced respiratory tract carcinoid disease is associated with carcinoid crises. 46,47 These tumours do not usually secrete serotonin or tachykinins but a similar syndrome may be a result of histamine production. 48 About one-third secrete calcitonin gene-related peptide (CGRP), some secrete gastrin-releasing peptide (GRP) (10–25%) and 60–70% secrete CgA. 49
Overview of NET secretory products
Cellular products and staining properties of NETs
Because of common histochemical properties of GEP endocrine tumours and the APUD concept, it was concluded that GEP NETs also developed from tissues of neural crest origin. However, more recent research has disproved this. It has been established that GEP tumours show a variety of histological structures, from solid tumours through trabecular, adenoid, undifferentiated and mixed growth tumours. Classification based on reactivity of cells to silver salts facilitates further classification into argentaffin, argyrophil and argyrophobe cells. 50
Neuroendocrine cells are characterized by uniform nuclei and clear granular cytoplasm. Silver staining was a specialized technique for identifying these cells until it was superseded by immunohistochemistry using specific antisera to the relevant cellular products (which are contained in the granules and may be released into the cytoplasm). Endocrine tumour cells share the basic characteristics of neuroendocrine cells. There are several general neuroendocrine markers which are used to identify endocrine tumours, including the granins, 51 neuron-specific enolase, 52 synaptophysin 53 and protein-gene product 9.5 (PGP9.5). 54
Immunohistochemical staining is used to identify the peptides and biogenic amines produced by NET cells and specific to the various tumour types. Care must be taken in choosing suitable antisera for immunostaining, as with immunoassay, indeed more so as immunostaining does not employ competitive methodology. Controls should be included at all stages. The precise specificity of antisera is of major importance. Specificity of antisera will be discussed in more detail in relation to immunoassays later in the article.
Products of NETs in the circulation
The granins are the ubiquitous family of proteins throughout endocrine and neuroendocrine cells. They are acidic proteins which are contained within the secretory granules of these cells 55 and are found in increased quantities in endocrine tumour cells. The granins include CgA, chromogranin B (CgB), chromogranin C, secretoneurin II and an increasing number of newly identified proteins. 56–58 CgA is the most important of the granins and is usually found in much higher concentrations than CgB. However, occasionally when CgA is within the reference range, CgB concentration is reported to be elevated. 59 Human CgA is a large protein of 439 amino acid residues 60 which undergoes post-translational processing to produce a number of active peptides. The actions of several of these peptides, however, remain elusive. In endocrine tumour cells, the production of CgA is increased and its processing altered, which results in large quantities of peptides being released into the blood stream. The products of CgA are not consistent between one tumour and another, resulting in a complex picture. In the chemical diagnosis of endocrine tumours, pancreastatin (residues 248–303 of CgA) was the first product of CgA to be measured, but more recently with improved methods of measurement the whole molecule is most commonly assayed.
In addition to CgA, many endocrine tumours from the DES produce a variety of peptide hormones and bioactive amines. These products are delivered into the blood stream and may be measured in venous blood. These molecules are responsible for the syndromes associated with endocrine tumours. In tumours of pancreatic origin, for example: insulinomas produce pro-insulin and/or insulin, gastrinomas produce gastrin and VIPomas produce VIP. In addition, PP is produced by the majority of pancreatic endocrine tumours. In the GI tract tumours arise in the stomach, where the products include gastrin, GRP and histamine. Tumours of the duodenum are extremely rare, accounting for <4% of all gastrointestinal endocrine tumours. 61 They produce gastrin most commonly but may alternatively produce somatostatin, PP, calcitonin or serotonin. Tumours of the jejunum and ileum, ‘classical midgut carcinoid tumours’ are the most common, increasing in frequency distally from the second part of the duodenum to the transverse colon. These tumours produce serotonin, tachykinins and bradykinin. Endocrine tumours of the appendix account for approximately half of this group. Almost invariably they present early with appendicitis and are cured surgically. Those that are metastatic produce the same markers as tumours of the midgut. Tumours of the hindgut (distal transverse colon, descending colon and rectum) are more rare. They do not secrete serotonin. Some hindgut tumours produce small but significant amounts of glicentin, PP, PYY or somatostatin. It has also been reported that most hind-gut endocrine tumours produce human chorionic gonadotropin alpha (HCGTα). 62
Measurement of secretory products of NETs in the circulation
Historically, peptides have been measured by radioimmunoassay (RIA) that offers specificity and sensitivity for the measurement of these small molecules, which normally circulate in picomolar concentrations. However, some sensitive immunoassays have been developed for a number of peptides and are available commercially. Commercial assays including RIAs are available for many of the peptides and although some show poor analytical sensitivity and specificity, this situation is constantly improving. Some commercial assays quote a rather high reference range when compared with in-house assays, although frequently no international standard is available. A high reference range may be associated with poor sensitivity in the assay of small peptides. All commercial assays are expensive when compared with in-house methods. Insulin, gastrin and calcitonin may be measured using automated methodology. However, particularly in relation to gastrin, these methods may be inadequate for tumour diagnosis because of the limited number of relevant molecules that are detected. The characteristics of some of the commercial assays are shown in Table 1. This table is not an exhaustive list but merely illustrates some of the robust assays that are available.
Some commercial assays available for peptides commonly raised in neuroendocrine tumours
N, No; Y, Yes; GRP, gastrin-releasing peptide; NKA, neurokinin A; VIP, vasoactive intestinal peptide; CGRP, calcitonin gene-related peptide
*UKNEQAS Guildford Peptide Hormone Scheme. Royal Surrey County Hospital, Guildford Surrey GU2 7XX, UK
**UKNEQAS for peptide hormones and related substances. The Royal Infirmary of Edinburgh at Little France, Old Dalkeith Road, Edinburgh EH16 4SA, UK
Stable, reproducible in-house RIAs for the measurement of peptides may be developed. Effort in developing the method is rewarded by the relatively low cost of materials thereafter. One disadvantage is that in-house assays are labour-intensive and where no international standard or external quality assessment scheme is available, then careful validation and standardization must be practised to maintain quality assurance. This again is labour-intensive. Because endocrine tumours are uncommon, it is not practical for individual centres to develop and maintain such assays for a wide range of secretory products. Many laboratories measure insulin and calcitonin and a number of them also measure CgA and gastrin. In the UK at present there are two central laboratories that offer a service for a wide range of tests for the diagnosis and monitoring of NETs. 63
Interpreting the significance of the concentrations of peptides is extremely important as some tumours will secrete relatively low concentrations, which makes interpretation of assay results complex. When circulating concentrations are very significantly raised this may also be for several reasons other than the presence of a NET. All the peptides discussed in this review with the exception of insulin are significantly raised in the circulation of patients with renal failure. 64,65 The chemical diagnosis of NETs in patients with renal failure and on dialysis is therefore difficult. As NETs frequently occur in patients beyond the sixth decade, renal function should be assessed. Furthermore, some of the treatments used in patients with NETs may adversely affect renal function and this must be borne in mind when interpreting results.
Chromogranins
Chromogranin A
It is commonly agreed that CgA is the most useful general circulating marker for GEP tumours. 66,67 Human CgA is a 439 residue acidic protein that is preceded by an 18-amino acid signal peptide. 68 Both C- and N-terminal regions of the molecule are greatly conserved, whereas the mid-portion of the molecule shows considerable sequence variation between species. The function of CgA is not fully understood, but it is thought to be involved in the packaging and processing of neuropeptide precursors and peptide hormones. It may also play a role in the organization of the secretory granule matrix. In addition, CgA is itself the source of a range of peptides which are a result of post-translational processing to produce precursor molecules and potentially active peptides. The CgA molecule contains a number of mono- and di-basic amino acid sites, which generally indicate the processing targets for proteolytic generation of pro-hormones. Many regional specific antisera have been raised to various sequences within the molecule and these have been used to illustrate that different processing sites predominate in different cell types and in different tumour cells. 69–73 Many endocrine cells express CgA receptors. However, somatostatin and PP cells express few epitope-binding sites for CgA, which indicates that these peptides are not regulated by CgA or its products.
Chromogranin B
CgB is the second most abundant member of the chromogranin family. Like CgA, it is a strongly acidic protein containing approximately 25% acidic amino acid residues. CgB shares two regions of strong homology with CgA, one near the N-terminal region and the second at the C-terminus. CgB promotes sorting of processing intermediates, which are derived from the precursors of peptide hormones. 74 The relative abundance of CgA and B vary not only from one species to another, but also from one tissue to another within species. In pancreatic endocrine tumours and in serotonin-producing tumours of the ileum and appendix, CgA is generally the quantitatively predominant protein. 75 However, it has been shown that in rectal carcinoids where CgA is generally absent, CgB is found. 76 Unlike CgA, CgB does not show increased concentrations in patients with renal failure, in patients with atrophic gastritis, or those receiving acid-suppressing therapy. This has increased the interest to measure CgB in addition to CgA in patients with tumours of the GEP tract. 77
Chromogranin A assay
CgA may be measured using a variety of reliable commercially available assays. In this laboratory, we have assessed two methods, 78 and Stridsberg has made a comparison of two RIAs and one enzyme-linked immunosorbent assay (ELISA) in a small group of patients. 79 Stridsberg's comparison of methods 80 showed a slight preference for the CGA-RIA Euro Diagnostica method that uses an antibody raised to CgA 116–439 over both the DAKO Chromogranin A ELISA and the Cis Bio International CGA-RIA. In the UK the DAKO CgA ELISA, which uses an antibody raised to a 23 kDa C-terminal fragment of CgA, is the method used in the two reference laboratories. All three methods are both specific and sensitive (Table 1). Further to these methods, some CgA assays have been developed where enzymatic digestion generates specific fragments that are then measured by RIA. 81 These assays have the advantage of measuring total CgA regardless of the degree of processing the molecule but are technically laborious and impractical for routine diagnostic use. In addition to the measurement of whole CgA, many RIAs have been developed to different epitopes within the CgA sequence where the aim is to measure certain products of processing the molecule. For tumour diagnosis, however, it is advantageous to measure the intact molecule and thereafter if desired to measure whichever fragments that may give additional information as these may vary greatly between each tumour. 82 For diagnostic purposes, the measurement of intact CgA is the best chemical screening tool for NETs.
CgA and the products of processing of the CgA molecule, including pancreastatin, show only a small rise in the circulation in response to food. 83 CgA is elevated in NETs although it is not invariably raised in benign tumours. This is particularly helpful with respect to assessing malignancy in insulinoma, where it has been reported that only malignant insulinomas produce elevated circulating CgA. 84 All states of gastric hypo- and achlorhydria result in elevated circulating CgA, where the ECL cells are stimulated by elevated gastrin concentrations in the blood stream that results from the lack of negative feedback for gastrin. 85 Raised circulating CgA, in addition to raised gastrin in atrophic gastritis, confounds the diagnosis of gastrinoma in many patients who present with dyspeptic symptoms. Patients treated with long-term histamine type 2 receptor antagonists or proton pump inhibitors also have raised circulating CgA. 86,87 Because of all these, gastric hypochlorhydric and achlorhydric states are common; care must be taken in the interpretation of CgA results. A circulating CgA concentration of more than twice the reference range is usually indicative of NET, whereas concentrations lower than this are inconclusive. It should be remembered that CgA is significantly suppressed by somatostatin analogue treatment in the majority of NET patients. This suppression may bring concentrations of CgA previously elevated to within the reference range. Somatostatin analogue therapy is used in the majority of NET patients.
Pancreastatin
Pancreastatin is a 49-amino acid peptide produced by dibasic cleavage from within the mid-portion of the CgA molecule (CgA 240–288). It was isolated by Tatemoto 88 using a method for detecting C-terminally amidated peptides. Pancreastatin inhibits insulin secretion, somatostatin release, exocrine pancreatic secretion and gastric acid secretion. 89 Before the complete sequence of CgA had been elucidated, pancreastatin was used as an epitope for antibody production. Pancreastatin antisera were used in immunohistochemistry and RIA to assess the presence of CgA in cells and the concentration of CgA in the circulation. Although pancreastatin assay occasionally remains in use as a surrogate marker for CgA, pancreastatin concentrations do not equate to CgA concentrations in the circulation. Some assays measure both processed pancreastatin and that within the CgA molecule, while other assays measure only processed pancreastatin. The pancreastatin molecule is found in significant amounts in the circulation of patients who have NETs with metastatic spread to the liver, 90 and concentrations are proportional to the number of hepatic deposits. Monitoring of liver metastases may remain the main advantage of pancreastatin assay.
Pancreastatin assay
Pancreastatin is measured in an extract of plasma after plasma proteins have been removed by precipitation with alcohol or by Sep-pak®. Several pancreastatin assays are available commercially. One robust commercial RIA is detailed in Table 1, although the sensitivity of this assay is poor.
Pancreastatin is measured by in-house RIA in the author's laboratory. 91 Antibodies were raised to synthetic pancreastatin or to a C-terminal fragment of pancreastatin which is available commercially (Penninsula Labs Inc., CA, USA; UK distributor – Bachem UK Ltd, England) Pancreastatin 33–49 (Porcine) (Product Code H 5905) coupled to a carrier protein using carbodiimide or glutaraldehyde. It should be remembered that pancreastatin is amidated and it is this molecule that is found in the circulation of GEP tumours. Amidation is crucial as the starting material for appropriate assays. Antibodies raised to the C-terminus of pancreastatin do not cross-react with whole molecule CgA. 83 Radiolabelled pancreastatin is prepared from synthetic tyr-0-pancreastatin (Bachem UK Ltd.; custom preparation Tyr-0 pancreastatin) using chloramine-T as an oxidant and the product is purified using high-performance liquid chromatography (HPLC). Iodinated pancreastatin is not commercially available, but may be purchased as a custom preparation (GE Healthcare UK Ltd, England; custom preparation 125I-radiolabelled pancreastatin) (Table 2).
In-house radioimmunoassays for peptides commonly raised in neuroendocrine tumours
GEH no longer supplies 125I or radio-labelled peptides. All of the materials previously supplied by GEH may now be purchased from Perkin Elmer Life & Analytical Sciences, Chalfont Road, Seer Green, Beaconsfield, Bucks HP9 2FX, UK. All of the relevant products have been tested by this laboratory and are of high quality.
Pancreastatin shows only a small rise postprandially, therefore a fasting specimen is not required. In normal subjects pancreastatin circulates in very low concentrations and is often undetectable when present as <5 ng/L (2.7 pmol/L). Pancreastatin is raised in the circulation of patients with endocrine tumours and especially those who have metastasized to liver. The assay is particularly useful in progressive disease where a rapid rise indicates the approach of terminal stage. 40
Pancreatic polypeptide
Pancreatic polypeptide was discovered by Kemmel in 1968 92 in bird pancreatic extracts as a contaminant of insulin preparations. Human PP was later identified by Chance 93 and subsequently isolated from the pancreas and characterized. 94,95 PP was the first of this family of peptides to be isolated. A decade later, PYY was isolated from intestinal mucosa 96 and Neuropeptide Y (NPY) from brain. 97 All three peptides have considerable homology and are encoded on chromosome 7 as three separate genes that have evolved through gene duplication. Although the physiological roles of NPY and PYY are well-defined, a specific role for PP has remained obscure. Both NPY and PYY activate most NPY receptors, whereas PP is very much less potent. PP is a single chain, 36-amino acid peptide (Figure 1) arising almost exclusively from the PP cells of the pancreas.
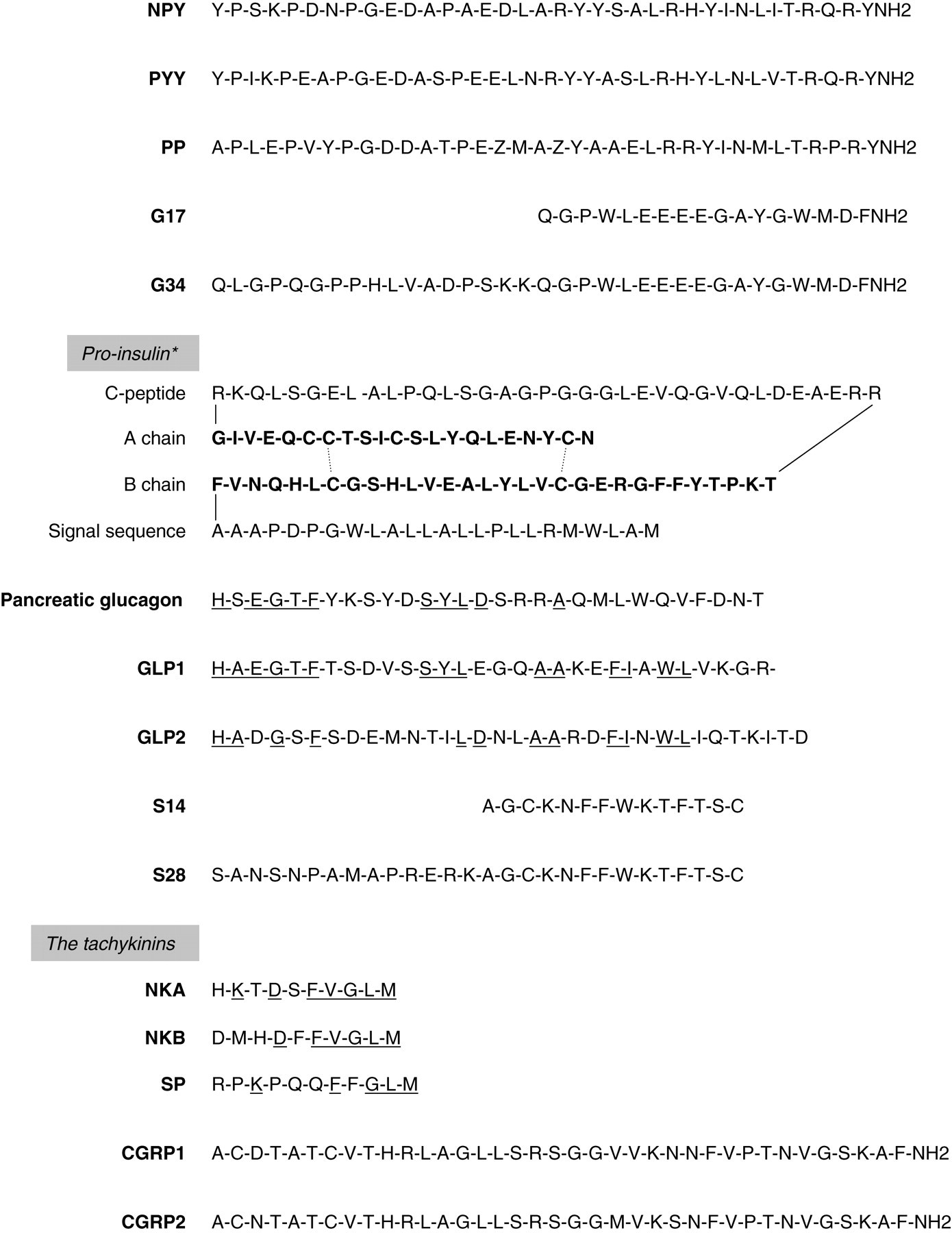
The sequences of various peptides secreted by neuroendocrine tumours illustrating structural similarities and differences. *Pro-insulin is folded to show the insulin sequence in bold, comprising A and B chains. CGRP1, calcitonin gene-related peptide 1; CGRP2, calcitonin gene-related peptide 2; G17, gastrin 17; G34, gastrin 34; GLP1, pro-glucagon 77–107; GLP2, pro-glucagon 126–258; NKA, neurokinin A; NKB, neurokinin B; NPY, neuropeptide Y; pancreatic glucagon, pro-glucagon 1–29; PP, pancreatic polypeptide; PYY, peptide Y, S14, somatostatin 14; S28, somatostatin 28; SP, substance P
Circulating PP shows a rapid response to food, particularly to protein and fat, although there is also a considerable response to oral glucose that is exaggerated in type I diabetes. There is no rise after intravenous nutrients. Intravenous infusions of acetylcholine, CCK, VIP or gastric inhibitory polypeptide (GIP) result in a significant rise in PP. Pathways governing the release of PP have been elucidated by Schwartz. 98 The principal regulation is vagal, cholinergic stimulation and response to stimulation is biphasic. The primary response is rapid and almost totally under vagal control. 99,100 The secondary phase, not totally under vagal control but mediated also by enteropancreatic and neurohumoral pathways, is prolonged and continues for 6 h after eating.
Although the relatively high concentrations that are measured in the circulation and the strong response postprandially lead one to conclude that PP is physiologically important, a major role has remained unclear. Although not as well studied as PYY in relation to appetite and satiety, it has been observed that PP rises in proportion to the calories ingested and when infused into the peripheral circulation appetite is suppressed and circulating ghrenin falls. Early studies using pharmacological doses of PP indicated that it had an inhibitory effect on stimulated pancreatic and biliary secretions. Little or no effect however has been observed on gastric acid, gastric emptying, insulin, glucagon, gastrin or secretin in humans.
Pancreatic polypeptide assay
Pancreatic polypeptide (PP) is readily measured in the circulation using immunoassay. Commercial PP assays are available and examples are detailed in Table 1. For in-house assay, antibodies may be raised to the total synthetic molecule or to a selected fragment coupled to a carrier protein using one of the well-tested methods for coupling peptides that employ carbodiimide, glutaraldehyde or triazine. 101,102 Careful consideration must be taken for the method of coupling as there are 11 acidic or basic groups which may be used, also four tyrosines. These multiple sites may result in some potentially confusing products of conjugation. Another confounding problem is the potential for cross-reaction between PP, PYY and NPY because of homology in the sequences (Figure 1). Antisera to PP therefore must be carefully selected and assessed for specificity. 103 Radiolabelling of PP is also not without problems, because of the four tyrosine residues where iodine may be incorporated. Careful purification of the labelled product using HPLC is crucial for reproducibility in the resulting assay. Radiolabelled PP is commercially available (Bachem. Radio labelled PP. Product Code H-5018), but the quality may not be suitable for use in RIA with all antisera, alternatively PP radiolabel may be custom prepared (GE Healthcare UK Ltd.; custom preparation 125I-radiolabelled PP) (Table 2).
Because of the significant response to food, it is essential that PP be measured only after an overnight fast (a minimum of 8 h). Circulating PP rises with increasing age and is higher in males than in females. 104 Elevated concentrations of PP are found in the circulation of patients with NETs, both pancreatic (50–0%) and gastrointestinal carcinoids (30–50%). 105 Before methods for the measurement of CgA were available, PP was used as a general marker for endocrine tumours, although it is poorly specific. PP measurement is now useful in the diagnosis and monitoring of endocrine tumours where no other general or specific marker is raised and in PPomas.
Gastrin
Gastrin was discovered by Edkins in 1905 when he observed acid-stimulating properties from the pyloric antrum of the stomach of pig. 106 After many years, and much debate as to whether this secretagogue was histamine, gastrin was finally isolated and purified by Gregory and Tracy some 60 years later. 107,108
The gastrin gene encodes two sequences which transcribe gastrin. 109 Gastrin is produced in numerous molecular forms: pre-pro gastrin, which is the initial gene product, is rapidly converted to progastrin and thereafter to smaller products, in particular the C-terminally glycine-extended gastrins. A further cleavage and amidation produces gastrin-34 (G34) and gastrin-17 (G17) (Figure 1). A previous review in this journal provides a detailed examination of the gastrin family. 110 Gastrin is distributed in the upper GI tract from the gastric antrum to the jejunum, decreasing distally. It is produced by the epithelial G cell. The cells of the antrum preferentially secrete G17, whereas those of the duodenum secrete G34 and G17 in approximately equivalent molar concentrations. 111
Gastrin is released in response to food, particularly protein, and is also released through autonomic pathways. 112 Gastrin is a powerful gastric acid secretagogue and the regulation of gastric acid is controlled through this pathway. The acid-secreting activity of gastrin resides in the five C-terminal residues of amidated gastrins, G17 and G34 113 and is mediated through the CCKB receptor. 114 As C-terminal amidation is critically required, C-terminally extended gastrins, do not possess acid-secreting activity. Gastrin also stimulates gastric mucosal cell proliferation and differentiation, which has led to the hypothesis that hypergastrinaemia is implicated in the aetiology of several gastrointestinal carcinomas including carcinoma of the stomach, 115 carcinoma of the colon 116 and gastric carcinoid. 117,118 This may be through two separate pathways, first the CCKB receptor and second through autocrine regulation not utilizing the CCKB receptor. The release of gastrin is suppressed through a negative feedback mechanism when the pH of the stomach is reduced as a result of acid secretion. In pathologies and pharmacologically induced conditions where gastric acid is diminished or absent, gastrin production and release continues to be stimulated. In the circulation, under normal physiological conditions, the major circulating components are G17 and G34, the latter being the predominant form in the fasting state.
Gastrin assay
Gastrin measurement using immunoassay is straightforward and many reliable commercial kits are available. Examples are detailed in Table 1. However, antibodies raised to the C-terminal of amidated gastrin are the most useful for the routine diagnosis of tumours. Antibodies which measure C-terminally extended gastrins produce results that are difficult to interpret. Antibodies which measure only G17 may fail to detect about 25% of tumours, 119 as G17 is not invariably raised in gastrinoma.
For in-house assay, antibodies to amidated gastrins may be raised to gastrin 2–17 coupled to a carrier protein using glutaraldehyde. 102 All the established methods may be used to generate gastrin antisera. Careful selection of antisera is important to ensure binding to all of the acid secretagogue gastrin molecules, all C-terminally amidated gastrins. The C-terminal residues of gastrin are common to CCK and cross-reaction with CCK should be avoided, although CCK circulates in extremely low concentrations compared with gastrin. Gastrin may be readily radiolabelled. Leu-15 gastrin radiolabelled using an adaptation of the Hunter and Greenwood method, 120 and purified using reverse-phase HPLC will produce a stable product less readily damaged by oxidation than that produced by the labelling of native gastrin. Gastrin is labelled at the tyrosine residue 12 of G17, which does not usually interfere with C-terminal antibodies. Radiolabelled gastrin is available commercially (Bachem; radiolabelled Gastrin-17, Product Code H-5342); however this product may not be suitable for sensitive RIA and a custom preparation may offer a better option (GE Healthcare UK Ltd.; custom preparation 125I-radiolabelled gastrin) (Table 2).
In addition to the two central laboratories in the UK that use in-house assays for gastrin, a further 20 laboratories use commercially available assays for the measurement of gastrin and take part in the UK national quality assessment scheme (UK NEQAS).
Because of a significant rise postprandially, circulating concentrations of gastrin should be measured after an overnight fast. Circulating gastrin is raised in gastrinoma. In 10–20% of patients, this elevation will be in the order of 5–20% above the reference range although in the majority of gastrinoma patients circulating gastrin shows a 10–100-fold rise. 119,121 However, several compounding factors make gastrin estimations difficult to interpret. First, Helicobacter pylori infection is associated with increased concentrations of gastrin and this is particularly relevant if the patient has not been fasted, as the gastrin response to food is greatly exaggerated in these subjects. 122–124 Secondly, all gastric hypo- and achlorhydric states result in raised circulating gastrin concentrations. 125 Long-standing autoimmune atrophic gastritis may result in a 100–1000-fold elevation. 126 As the vast majority of patients who present with a grossly elevated gastrin have autoimmune atrophic gastritis, parietal cell antibodies may be measured to exclude this diagnosis. Thirdly, treatment with proton pump inhibitor drugs or histamine type-2 receptor antagonists results in significant elevation of gastrin (owing to loss of negative feedback), up to two-fold, the reference range. 123,127,128 In patients who have been on long-term treatment with these drugs, gastrin does not return to baseline for many months after withdrawal of therapy. 129 Withdrawal of treatment for 3 d will show a significant reduction in circulating gastrin concentrations. However, in patients with gastrinoma even this short period without acid-suppressing treatment may be life-threatening and patients should be carefully observed during this vulnerable period. Fourth, although a rare diagnosis, patients with phaeochromocytoma may show an elevation of 2–4 fold in gastrin. 130 To confirm the diagnosis of gastrinoma, acid-secretion studies may be performed. This may be 24-h pH monitoring or 1 h basal acid secretion after withdrawal of acid-suppressing therapy. Two further tests may be carried out to aid diagnosis, a secretin stimulation test, where a bolus of intravenous secretin is administered after two baseline blood specimens have been taken. Serial blood specimens for gastrin measurement are collected during a 60-min period. 131 This is followed, often directly, by a test mixed meal, with the collection of further serial blood specimens for gastrin estimation. In normal subjects there is no gastrin response to intravenous secretin and a rise after a mixed meal between 50% and 200%. In 50–70% of gastrinoma patients, secretin stimulates release of gastrin (two-fold) where the release of gastrin after the test meal is minimal.
Insulin, pro-insulin and C-peptide
The discovery of insulin 132 in 1921, and its subsequent purification from porcine pancreas to a quality that could be used in the treatment of diabetes, was rewarded with a Nobel Prize in recognition of the key role of insulin in diabetes mellitus and its potential for control of that disease. This discovery remains the most significant in the chemistry and pathophysiology of peptides to date. Insulin is a heterodimeric peptide synthesized in the beta cells of the islets of Langerhans from a single chain precursor, pro-insulin. The removal of a 24-amino acid signal sequence releases pro-insulin from pre-pro-insulin. Further processing results in the cleavage of connecting peptide (C-peptide) to produce insulin. Insulin is composed of two amino acid chains, A and B (formed by the removal of C-peptide), and held in association by disulphide bonds (Figure 1). Equimolar concentrations of insulin and C-peptide are secreted from the beta cell. However, as C-peptide has a longer half-life than insulin due to its hepatic extraction, higher concentrations of C-peptide are measured in plasma.
Insulin is the most potent anabolic peptide. It is essential for the maintenance of glucose homeostasis throughout the body and is the basic requirement for brain function, tissue development and growth. Despite wide variation in food intake and physical activity, blood glucose concentrations are held within narrow limits through the action of insulin. Insulin is released in response to glucose, release being dose-dependent. Oral glucose is a more potent stimulant than intravenous glucose due to increased sensitivity of the beta cell as a result of stimulation of incretins resulting from absorption of glucose in the GI tract. 133–135 In the absence of glucose, amino acids stimulate insulin secretion. Release of insulin into the circulation in response to food increases peripheral uptake and peripheral catabolism, lowers liver glucose production and increases uptake of nutrients in the liver. The release of insulin is inhibited predominantly by glucagon in response to hypoglycaemia. Somatostatin also inhibits insulin release.
Insulin, pro-insulin and C-peptide assay
For the diagnosis of insulinoma, it is best to use a pro-insulin assay or an assay that measures both pro-insulin and insulin in order to include the diagnosis of patients who predominantly secrete pro-insulin from a tumour. However, in many laboratories insulin is measured using automated methodology which measures insulin alone. When insulinoma is suspected, a C-peptide assay may be used in addition to insulin assay to exclude the possibility of interference from exogenous insulin. A robust commercial pro-insulin assay is also available. Table 1 gives details of some commercially available insulin and C-peptide assays and a reliable pro-insulin assay which is also available commercially.
For in-house RIA, high-titre antibodies may be raised in guinea pigs without coupling insulin to a carrier protein. Antibodies may be raised which cross-react with insulin and pro-insulin, resulting in an assay ideal for the diagnosis of insulinoma. Radiolabelled insulin is used as tracer which may be prepared in-house using conventional techniques 102 or is available commercially (GE Healthcare UK Ltd.; 125I-radiolabelled insulin, Product Code IM116). Insulin and pro-insulin are stable in blood and no proteolytic inhibitor need be added to the collection bottles. Because of basic amino acid residues in the primary structure of insulin, it adheres to surfaces and care must be taken to reduce this problem. This may be ensured by avoiding bubbling and frothing of the specimen and standard preparations, by adding albumin to all buffers used in the assay procedure and by using polypropylene tubes for storage of standards and quality control specimens for in-house assays (Table 2).
Circulating insulin rises rapidly postprandially and non-fasting specimens collected at outpatient clinics are not suitable for the diagnosis of insulinoma. When fasting insulin is measured, a simultaneous measurement of blood glucose will be necessary for the interpretation of results. Immunoreactive insulin is frequently raised in type II diabetes. Insulin may be only marginally or intermittently elevated in the circulation of patients with insulinoma. Although insulinoma is the most common endocrine pancreatic tumour, it is notoriously difficult to diagnose both radiologically and chemically. Radiological diagnosis is frequently difficult because tumours may be multifocal and very small (<1 cm in diameter). Hypoglycaemia with inappropriately raised insulin and pro-insulin or C-peptide, after the exclusion of insulin secretagogues, indicates insulinoma. Serial blood glucose measurement during a supervised 12–72-h fast will confirm the diagnosis. This test will frequently be abandoned due to hypoglycaemia long before 72 h (usually between 12 h and 36 h). Insulin abuse, often quoted as a confounding factor in the diagnosis of insulinoma, is uncommon. 136
Glucagon
Glucagon activity was observed by Murlin et al. 137 when administration of impure preparations of insulin produced an initial transient rise in blood glucose. Pancreatic glucagon was subsequently isolated by Collins and Muirin, 138 purified in 1955 139 and synthesized by Wunsch. 140 Glucagon activity was observed also in extracts of gut mucosa in 1948 by Sutherland and de Duve 141 and this was confirmed by Kenny and Say. 142 Glucagon is secreted from the alpha cells of the islets of Langerhans in the pancreas and by the L-cells in intestinal mucosa. 143 In 1983, the glucagon gene was identified by Bell et al. 144 and was found to encode pro-glucagon which is a 160-amino acid peptide. Tissue-specific post-translational processing occurs resulting in different peptides arising in the pancreas from those that arise in the gut. In the pancreas pro-glucagon is processed to give glicentin-related polypeptide (GRPP), 1–30 glucagon, 33–61 intervening peptide-1 64–69 and the major pro-glucagon fragment. 72–158 In the gut, pro-glucagon is cleaved to release glicentin 1–69 (sometimes referred to as gut-glucagon), glucagon-like peptide 1 (GLP-1), 78–107 intervening peptide-2 111–123 and glucagon-like peptide 2 (GLP-2). Glicentin contains the sequence of glucagon but is further processed in the gut to give glicentin-related peptide 1–30 and oxyntomodulin. 33–60 Pro-hormone convertase (PC1) has been shown to be responsible for the processing of pro-glucagon in gut epithelial cells. 145 There is significant homology between glucagon, GLP-1 and GLP-2 particularly in the N-terminal regions of glucagon and GLP-1 (Figure 1).
Pancreatic glucagon is released in high concentrations into the portal circulation, in response to hypoglycaemia, where it stimulates glycogenolysis and gluconeogenesis mediated through the cyclic AMP chain. 146 In response, the liver changes from an organ of glucose storage to an organ of glucose release. Insulin and glucagon counter-balancing actions facilitate the control of glucose flux without major change in circulating glucose concentrations. Glucagon is also released in response to amino acid infusion. Glucagon release is inhibited by hyperglycaemia. Because glucose is required for cerebral metabolism and anoxic muscle metabolism, in stress situations circulating pancreatic glucagon is released even in the presence of hyperglycaemia. In addition to glycogenolysis and gluconeogenesis, glucagon also inhibits gastric emptying, and gastric acid output, inhibits pancreatic endocrine and exocrine secretion but increases bile flow. It increases cardiac muscle contraction. Glucagon also has lipolytic effects.
Glucagon and glicentin assay
Due to the sequence homology between pancreatic glucagon and glicentin (Figure 1), the selection of regional specific antisera is crucial for glucagon assay. Antibodies raised to the N-terminus of glucagon common with glicentin and GRPP will cross-react with all three peptides, giving a measure of total glucagon. Antisera raised to the C-terminus of pancreatic glucagon may or may not cross-react with glicentin and GRPP. To measure pancreatic glucagon, careful selection of non-cross-reactive antisera is essential, as antibodies used to measure pancreatic glucagon must be C-terminal-specific. Antibodies raised to the C-terminus of glicentin will not cross-react with pancreatic glucagon but may cross-react with GLP1. Sequence homology between pancreatic glucagon, GLP1 and GPL2 is not usually problematic. Frequently, two assays are used for the measurement of glucagons – a pancreatic glucagon-specific assay (C-terminal assay) and a total glucagon assay (N-terminal assay), which measures pancreatic glucagon, glicentin and GRPP. As a result of two possible post-translational processing pathways for proglucagon, pancreatic glucagon may not be raised in glucagonoma patients. In addition, the more rare tumours that produce GLP1 or GLP2 will also show an elevation in glycentin. 147 Some commercial glucagon RIAs are available but sensitivity may be poor. Some examples of commercial assays are given in Table 1. For in-house RIA, radiolabelled glucagon may be prepared using pancreatic glucagon and incorporating 125I using conventional means. 102 Radiolabelled glucagon is available from two sources. The preparation available from Bachem may not be suitable for use in RIA. A high quality preparation is available from Bachem (125I-radiolabelled glucagons. Product Code H-5274) and this preparation is suitable for use in both pancreatic and total glucagon assays (Table 2).
Both circulating pancreatic glucagon and glicentin show a rise after food, therefore patients should be fasted overnight before blood sampling. Circulating glucagon is raised in glucagonoma where the concentration may be 10–100 times the reference range. Glucagon is also raised in hypoglycaemia, malabsorption, with severe head trauma, burns and in cachexia.
Somatostatin
Somatostatin was identified and isolated as the growth hormone release inhibiting factor found in extracts of ovine 148,149 and porcine hypothalamus. 150 The importance of this discovery and its impact thereafter was recognized when the Nobel Prize for Medicine in 1977 was awarded to Guillemin and Schally for their work in this area. Somatostatin is present throughout the central nervous system. 151 It is also found throughout the gut, in the pancreas, the thyroid, adrenal medulla and the salivary glands. 152 Somatostatin is located in the pancreatic D-cell 153 and in morphologically similar cells in the gut. Somatostatin is very highly conserved throughout the animal kingdom. It is a cyclic peptide with a disulphide bond between residues 3 and 14. It occurs in two forms: somatostatin 14 (S14), and the N-terminally extended somatostatin 28 (S28) (Figure 1). The distribution of these two molecules varies from one site to the other. S14 is the predominant form in nerve tissue and in pancreatic and duodenal cells, whereas S28 is the predominant form in the stomach and ileum.
Somatostatin acts as a neurotransmitter, but in the endocrine cells of the pancreas and gut it acts in a paracrine fashion. All the actions of somatostatin that have been identified are inhibitory. It inhibits the release of growth hormone and thyroid-stimulating hormone from the anterior pituitary and insulin, glucagon and PP from the pancreas. It also inhibits the release of the gastrointestinal hormones and peptides gastrin, CCK, secretin, motilin, GIP, VIP and glicentin. 154 Inhibitory effects are due, more to suppression of release rather than inhibition of production of the various cellular products. Somatostatin inhibits gastric acid secretion, and the release of pepsin, acetylcholine and intrinsic factor. It delays gastric emptying, suppresses pancreatic exocrine function and slows intestinal motility. Somatostatin modulates many organs in a paracrine fashion.
The therapeutic potential of somatostatin was recognized soon after the peptide had been identified. Five somatostatin receptor subtypes have been isolated, 155–157 some are further subdivided. Somatostatin analogues have been developed which have an extended half-life compared with the native peptide. Currently available analogues to somatostatin, octreotide and lanreotide, bind to receptors SS2 and SS5 with high affinity and to the receptor SS1 with lower affinity. 158 Somatostatin analogues have been used for the treatment of acromegaly, pancreatic NETs and carcinoid tumours with considerable symptomatic success. 159–161 Seventy percent of patients with NETs show a biochemical response to somatostatin analogue therapy with symptomatic relief in 60% and reports of tumour response in 5–10%. 162 Analogues to the other receptor subtypes SS3 and SS4 and to combinations of the receptors are in various stages of development.
Somatostatin is released in response to food, although the rise in the peripheral circulation is small. 163 Beta-adrenergic agonists cause the release of somatostatin, calcitonin, CGRP, motilin, VIP, GIP and glucagon. Somatostatin release is inhibited by acetylcholine and by opioid receptor antagonists.
Somatostatin assay
Somatostatin is measured by immunoassay and several commercial assays are available. Examples are shown in Table 1. For in-house assay, antibodies may be raised to S14 or S28. Antibodies to S14 generally cross-react with S28. As somatostatin circulates in a cyclic form it is important that antibodies recognize somatostatins in their cyclic configuration. Somatostatin is poorly immunogenic due to the total conservation of the molecule across all species. Some excellent antibodies have however been produced. It is essential that antibodies do not cross-react with somatostatin analogues, which are used in the treatment of endocrine tumours and are administered in high doses. Antibodies may be raised to S14 coupled to a carrier protein using the methods referred to previously for other peptides. Radiolabelled somatostatin may be prepared using Tyr-0 or Tyr-1 somatostatin. The products are purified using HPLC. Radiolabelled S14 is also available commercially (GE Healthcare UK Ltd.; 125I-radiolabelled somatostatin, Product Code IM161). In the UK there is an assay available for routine clinical use in both the laboratory referral centres. Somatostatin requires a blood extraction preassay preparation, which may be achieved using precipitation with alcohol or using Sep-pak®. Some laboratories use Sep-pak® in order to concentrate the sample as normal physiological circulating concentrations of somatostatin are extremely low.
A mixed meal is followed by a rise in circulating somatostatin by approximately 5%. It is therefore not necessary to fast patients prior to somatostatin measurement. Somatostatin is raised in the circulation of patients with duodenal endocrine tumours (20%) 164 or hindgut carcinoid (30–35%) 62 where elevations are two to four times the reference range. Somatostatin is grossly elevated in patients with somatostatinoma. This is a rare tumour most commonly originating in the pancreas and frequently presents at a late stage with widespread metastases, due to the mild symptoms associated with this tumour.
Vasoactive intestinal polypeptide
VIP was discovered by Mutt in 1970 165 and isolated from porcine duodenal mucosa. It is a 28-amino acid peptide which has considerable homology with the secretin-glucagon family, particularly at the N-terminal region of the molecule. The strongest homology is with peptide histidine methionine (PHM), a 27-amino acid peptide and the human equivalent of peptide histidine isoleucine (PHI), which is encoded by the same mRNA as VIP. 166,167 In tumour tissue from VIPoma and in the circulation of these patients, VIP is also found in a larger form (15 kD); 50% of VIP may be in this form. This large molecule is not detected in the circulation of normal subjects. 168 Although it was originally thought that VIP was released from endocrine cells, it has long been established that the vast majority of VIP arises in neurones in the tissues in which it is found. VIP is found in peripheral ganglia and VIP neurons are found throughout the GI tract, in the pancreas, the urogenital tract, the respiratory tract and in blood vessels. 169,170 VIP has widespread biological activities. In the GI tract, it relaxes the lower oesophageal sphincter and fundic smooth muscle. It suppresses gastric acid secretion. It inhibits the contractile effects of CCK, also absorption in the ileum. Like secretin, it stimulates the secretion of water and bicarbonate and stimulates secretion of water and chloride from the large intestine. VIP stimulates adenylate cyclase activity and the release of insulin and glucagon. It stimulates the release of prolactin, growth hormone and luteinizing hormone while suppressing the release of somatostatin from the hypothalamus. VIP is a potent vasodilator and bronchodilator. In the immune system, it inhibits transformation of T-lymphocytes, mast cell histamine release, platelet aggregation and secretion and stimulates immunoglobulin synthesis. 171–174 PHM possesses many of the properties of VIP also and is a potent stimulant of small intestine secretion but is less potent than VIP.
Vasoactive intestinal polypeptide assay
At least one reliable, sensitive commercial assay is available for VIP (Table 1). For in-house RIA, antibodies may be raised to synthetic human VIP using carbodiimide or any of the established methods used to couple peptides to carrier proteins. 102 Because of the considerable homology between PHM and VIP, the specificity of VIP antisera must be thoroughly assessed. Cross-reaction with glucagon, glicentin, secretin and GIP must also be excluded. Radiolabelled VIP is prepared using iodogen or chloramine-T as oxidant followed by purification using HPLC. Radiolabelled VIP is available commercially (GE Healthcare UK Ltd.; 125I radiolabelled VIP Product Code IM158) (Table 2).
VIP shows no significant rise after food. It is not therefore necessary to collect fasting specimens for assay. VIP is raised in VIPoma, ganglioneuroma and neuroblastoma. 175,176 Elevation in VIP may be small, 10–20% above the reference range, as it is a potent molecule and patients will present with severe watery diarrhoea at an early stage of disease. 177
Gastrin-releasing peptide
Mammalian gastrin-releasing peptide (GRP) was originally isolated from porcine gastric tissue by McDonald et al. 178 and was shown to exhibit properties similar to bombesin, the amphibian skin peptide which had previously been isolated by Anastasi. 179 Human GRP mRNA was later isolated from a lung carcinoid and the sequence deduced. 180 The sequence was later confirmed by Orloff. 181 Early studies of the distribution of GRP employed the measurement of bombesin-like immunoreactivity 182 and found the highest concentration to be in the hypothalamus. In particular, the major concentrations were in the ventro-medial, preoptic and posterior hypothalamus, although significant quantities of GRP have been identified throughout the central and peripheral nervous systems. GRP is present in nerve fibres throughout the GI tract, with the highest concentrations found in the antrum of the stomach. It is also found in the respiratory tract. In the foetus it is located in the epithelial cells where it is thought to be involved in lung development, 183 whereas in the adult GRP is predominantly found in nerve fibres. GRP is released in response to protein in the stomach. GRP stimulates the release of gastrin, 184 which in turn stimulates the ECL cells to produce histamine, which in turn stimulates the parietal cells to produce acid. GRP also activates inhibitory pathways involved in the regulation of gastric acid secretion, 185 thus playing a major role in the mediation of meal-stimulated acid secretion. 186 GRP is released in response to electrical stimulation of the vagus. Intravenous administration of GRP stimulates the endocrine pancreas and in particular the release of insulin, but also to a lesser degree the release of glucagon and PP. At high doses GRP stimulates pancreatic acinar cells. GRP stimulates the release of glicentin, GIP, CCK, VIP and motilin. In addition, intravenous injection of GRP causes an increase in arterial blood pressure and heart rate.
Gastrin-releasing peptide assay
At this time, the author has experience of no satisfactory sensitive commercial GRP assay kit available for the measurement of circulating GRP concentrations in human plasma. GRP may be measured by in-house RIA. Antibodies are raised to synthetic human GRP or a synthetic fragment coupled to a carrier protein using conventional methods. Radiolabelled GRP is prepared using the iodogen method and the products are purified by reverse-phase HPLC. Radiolabelled GRP is also available commercially (GE Healthcare UK Ltd.; 125I-radiolabelled GRP Product Code IM169). A GRP assay is available in the laboratory represented by the author (Table 2). 187
The rise in circulating GRP postprandially is not significant. GRP may be raised in the circulation of patients with endocrine tumours of the stomach 31,62 and lung carcinoid. GRP may also be raised in the circulation of patients with some non-endocrine carcinomas including small cell lung tumours.
Neurokinin A and the other tachykinins
Tachykinins are a large family of neuropeptides and are the most common of all neuropeptides. Isolated from equine brain and later frog, 188,189 they are found throughout the animal kingdom. 190,191 NKA is one of the three tachykinins found in humans, the others being Substance P (SP) and Neurokinin B (NKB). In addition, NKA is found in two extended forms (Figure 1). Tachykinins are encoded from two pre-pro-tachykinin genes, PPT-A, encoding SP, NKA and the two longer forms of NKA and PPT-B that encodes NKB. The PPT-A gene may undergo alternate splicing but the significance of this is not fully understood. 192,193
Tachykinins have a widespread distribution in the central and peripheral nervous system. In humans, tachykinins are found throughout the brain and in the intrinsic enteric neurons of the myenteric and submucosal plexuses also in extrinsic primary afferent fibres. SP and NKA are found in the renal pelvis, the bladder, uterus and in the respiratory tract. In normal physiology, the EC cells of the gut mucosa also contain tachykinins and probably account for these peptides being present in the circulation. 194 NKA is a decapeptide as is NKB. SP has one more amino acid residue. All three peptides share an almost identical C-terminus, which is the active site (Figure 1). Tachykinins are released in response to physiological and non-physiological stimuli through a calcium-dependent mechanism. Tachykinins administered intravenously in human, decrease blood pressure, increases respiration rate, stimulate vasodilation, increasing body temperature and peripheral blood flow, to the skin and particularly to the head. 195 SP is between five and 20 times more potent than NKA, although both are much less potent than noradrenaline, angiotensin and serotonin. It is possible that tachykinins play a role in the vascular control in certain areas of the body. NKA and SP have an effect on respiratory airways, 196 although there is some debate as to which is more potent. Tachykinins are implicated in the regulation of learning and memory pathways. 197 Investigations of physiological and pharmacological effects of tachykinins on all tissues have been carried out in many species with conflicting results between species. It is therefore difficult to draw conclusions for humans from investigations undertaken in other species.
Tachykinin assay
Tachykinins are readily measured in plasma or serum using RIA or ELISA. More than one reliable commercial assay is available for the measurement of SP, but these are dependent on stringent specimen collection procedures (Table 1).
For in-house RIA, antibodies may be raised to NKA in rabbits or guinea pigs and larger species. The use of glutaraldehyde as coupling agent will produce an antibody which cross-reacts with NKB and may cross-react with neuropeptide K and SP. This may not be undesirable in the clinical situation; in tumours where there are elevated circulating tachykinins, a measure of all the tachykinins rather than one may be appropriate. NKA radiolabel is prepared using conditions for radiolabelling that are suitable for incorporation of iodine into histidine followed by HPLC purification of the products. Radiolabelled NKA is available commercially (GE Healthcare UK Ltd.; 125I-radiolabelled NKA, Product Code IM168) (Table 1). After release, tachykinins are susceptible to enzyme degradation in the circulation, the most vulnerable being SP. Under routine clinical specimen collection conditions, without sufficient care, SP assay is unreliable. Both NKA and NKB are more resilient. As NKA is found in significant concentrations, it is the tachykinin of choice to measure routinely in the circulation. Tachykinins are found in high concentrations in metastatic endocrine tumours of the ileum-MGC. 31 Tachykinins do not show a significant rise postprandially. In a retrospective study, it has been shown that NKA is a sensitive indicator of poor prognosis in midgut carcinoid. 40 NKA assay is available for clinical diagnosis and as a prognostic indicator for MGC in the laboratory represented by the author. 40 Tachykinins are raised in asthma particularly during asthmatic attack. 198
Calcitonin
Calcitonin is encoded on chromosome 11 by two genes and is produced in a 136-amino acid precursor, pro-calcitonin. 199 Within the secretory granules, it is processed to produce calcitonin which is a 32-amino acid peptide with a disulphide bond between residues 1 and 7, forming a N-terminal loop. In normal physiology, calcitonin is found exclusively in the non-follicular C-cells of the thyroid. The synthesis and release of calcitonin is closely associated with calcium concentrations. Calcitonin is also secreted in response to CGRP, glucagons, gastrin, CCK and β-adrenergic agents. 200,201 Somatostatin suppresses the release of calcitonin. In fish, calcitonin circulates at very high concentrations and is very potent in controlling blood calcium. However, calcitonin control in calcium homeostasis in humans has not been proven.
Calcitonin assay
Calcitonin is measured by RIA or by MIA. Specimen collection tubes may be important depending on the method used. There are many commercial assays available for the measurement of calcitonin and a small selection of these are detailed in Table 1. For immunoassay, antibodies may be raised to human calcitonin according to conventional methods. For RIA, radiolabelled calcitonin is prepared using the iodogen or chloramine-T methods and the products are purified using reverse phase HPLC. Radiolabelled calcitonin is available commercially. (GE Healthcare UK Ltd.; 125I-radiolabelled calcitonin, Product Code IM175). The reference range for calcitonin is heavily method-dependent. MIA methods give much lower concentrations in the circulation than do RIA methods. Calcitonin is stable in blood and a fasting specimen is not required. Calcitonin is raised in medullary thyroid cancer (MTC) where concentrations may be more than a thousand-fold the reference range. In monitoring the progression of disease, attention should be paid to the method used for assay. Twenty five percent of MTC cases are familial where there is a germline mutation on chromosome 10. 202 For this reason family members were screened for MTC and a pentagastrin stimulation test may be used to stimulate the secretion of calcitonin in such subjects. MTC tumours frequently arise as part of the multiple endocrine neoplasia type 2 (MEN2) syndrome. Calcitonin may also be raised in some pancreatic endocrine tumours, particularly those that are multihormone producing and in some non-endocrine cancers. 203
The calcitonin family of peptides (includes CGRP, amylin, adrenomedullin and intermedin-I)
Calcitonin gene-related peptide occurs in two forms: CGRP I (α-CGRP) and CGRP II (β-CGRP) that are encoded by the two calcitonin genes on chromosome 11. 204 CGRP has a widespread distribution in the nervous system. It is found in the highest concentration in the hypothalamus but is also found in specific nuclei of the brain stem. In the peripheral nervous system, it is found in sensory afferent nerves close to the spinal cord, in nerve fibres that are found in association with blood vessels, and in motor neurones, at the muscular junctions where it co-localizes with acetylcholine. 205 CGRP is frequently identified in close association with other neuropeptides including the tachykinins.
Calcitonin gene-related peptide shows considerable conservation across species. Human CGRP 1 and 2 are both 37-amino acid peptides differing only by three residues. Both the CGRPs have a disulphide bridge between residues 2 and 7 forming a loop at the N-terminus. This is a common feature of all calcitonin gene products (Figure 1). The properties and functions of CGRP1 and CGRP2 are very similar. CGRP is a potent vasodilator. GRP is important in satiety and administration of CGRP results in a decrease in food intake. It also decreases gastric secretion and reduces intestinal motility. Pharmacological studies suggest that CGRP may play a role in the regulation of calcium and in insulin secretion. It may also have a role in the synthesis of acetylcholine receptors and in peripheral nerve regeneration.
Calcitonin gene-related peptide assay
There are several commercial assays available for CGRP and at least one sensitive ELISA is suitable for measuring circulating concentrations (Table 1). Calcitonin gene-related peptide may also be measured by in-house RIA. Antibodies that are raised to the C-terminal region of CGRP will measure both CGRP1 and CGRP2. This is desirable for tumour diagnosis. Radiolabelled CGRP is prepared by incorporating 125I into histidine and products are purified by reverse-phase HPLC. Radiolabelled CGRP is available commercially (GE Healthcare UK Ltd.; 125I-radiolabelled CGRP, Product Code IM184). CGRP circulates in low concentrations and does not rise significantly in response to food. CGRP is elevated in MTC and in some lung carcinoid tumours (30%). 31,206 CGRP may be raised in some non-endocrine tumours, particularly in small cell lung tumours. 207
Conclusion
GEP NETs are an uncommon yet significant group of tumours, that are usually slow growing but may vary considerably from indolent to aggressive disease. Some are benign but the majority are malignant and probably almost all possess the potential to become malignant. If diagnosed at an early stage, even with metastatic disease, patients may survive for many years with a good quality of life. Many of these tumours are associated with syndromes that result from the production of bioactive peptides and amines. These syndromes are frequently potentially more life-threatening than is the malignancy. While surgery offers the only possibility of cure this is not usually secured except for benign tumours of the pancreas and small carcinoid tumours of the respiratory tract. Palliative treatments are numerous and range from somatostatin analogue therapies for control of symptoms to more aggressive options such as hepatic embolization. It is important that the timing for intervention is optimal, as slow growing tumours may require little intervention, whereas rapidly progressing disease must be addressed immediately. It is strongly recommended that patients suffering from NETs be referred to specialist clinics and in the UK there are more than 15 such centres. 63 The measurement of the secretory products of NETs offer a diagnostic tool and a means of monitoring disease progression. Increasing attention is now also directed towards the possibility of prognostic indicators in the light of the potential of aggressive disease in some patients. CgA is the best general marker for NETs and reliable commercial assays are available for the measurement of CgA. In addition to CgA, there are specific peptides which are secreted into the circulation from specific tumours and reliable assays are available for the measurement of these cell products too, some commercial and some in-house assays. The measurement of these specific peptides is important to monitor tumour activity, progression of disease, response to treatment, recurrence and change in cell type associated with worsening prognosis. Because of the rarity of these tumours, the expertise required for interpretation of peptide estimations and the cost of providing these assays, only a few reference laboratories offer a full screening and monitoring service with consultant advice.