
Abstract
Background
Recent recommendation advocates the reporting of HbA1c in terms of mean plasma glucose. We examined the impact of improving patients' interpretation of a given HbA1c value on glycaemic control.
Methods
We conducted a questionnaire survey among 111 patients attending a hospital diabetes clinic. Patients were provided with information relating to the association between HbA1c and mean plasma glucose levels. Glycaemic control among 80 patients with poor glycaemic control was assessed before and approximately seven months after such intervention.
Results
Of the respondents, 40.5% (45/111) were familiar (F) (31 type 1, 14 type 2) and 59.5% (66/111) were unfamiliar (U) (23 type 1, 43 type 2) with the term HbA1c. Following information about the interpretation of HbA1c, patients with poorly controlled diabetes (HbA1c >9%) showed a significant reduction in HbA1c levels if they were from group U (10.7% vs. 9.5%, P = 0.04) but not from group F (10.5 vs. 9.8, P = 0.28). Patients with moderately poor glycaemic control (HbA1c 7.5–9%) showed no significant change in HbA1c levels following intervention (8.3% vs. 8.2%, P = 0.57 group U; 8.3% vs. 8.2%, P = 0.79 group F).
Conclusion
Patients' knowledge of HbA1c is poor, especially among persons with type 2 diabetes. Improvement in patients' understanding of HbA1c, particularly among those with very poorly controlled diabetes with no prior knowledge of HbA1c is associated with improvement in their glycaemic control. Strategies to engage patients to know and interpret their HbA1c values should be encouraged within routine clinical practice.
Background
Despite irrefutable evidence on the benefits of tight glycaemic control among persons with diabetes, 1,2 many patients fail to achieve optimal glycaemic target and remain at risks of developing long-term vascular complications. Complexities of diabetes treatment regimen and personal psychosocial as well as physiological and genetic factors may contribute to this. The success of patients to manage their diabetes will therefore rely not only on their ability to adhere to a particular treatment regime, but also for health-care professionals to develop intervention strategies that would allow the patients to make appropriate lifestyle decisions, set treatment goals and assume responsibilities for their daily diabetes care. 3
Goal setting within this patient empowerment philosophy is a multistep process that provides patients with the knowledge they need to achieve their personal treatment requirements. 3,4 Embedded within this process is the therapeutic goal to which patients and carers of persons with diabetes strive to achieve. Clinicians have traditionally used HbA1c test results to guide treatment decisions, but few studies have assessed patient's knowledge on their ability to interpret a given HbA1c value and perhaps more importantly whether improving patients' understanding on the relationship between HbA1c and mean plasma glucose value would favourably affect their diabetes control. This issue is of particular importance, given the recent completion of the HbA1c-derived average glucose (ADAG) trial to document the relationship between HbA1c and mean plasma glucose values. 5 The study has led to the recommendation that in future, HbA1c results should be reported worldwide in IFCC (International Federation of Clinical Chemistry) units (mmol/mol) – derived from the IFCC-NGSP (National Glycohemoglobin Standardization Program) master equation and in terms of HbA1c-derived average blood glucose. 6,7 This would enable clinicians to convey the concept of chronic glycaemia in units most relevant to the values obtained from patient glucose self-monitoring. We therefore undertook a study to assess if our patients were (1) familiar with the terms HbA1c, (2) able to correctly interpret a given HbA1c value and (3) whether educating patients about the relationship between HbA1c and mean plasma glucose within routine clinical practice would improve their glycaemic status.
Methods
This was a clinical evaluation study within routine clinical practice. Questionnaires were given to 120 consecutive patients with type 1 and type 2 diabetes on their arrival at a hospital diabetes clinic between the months of June–August 2005 to assess their familiarity with the term HbA1c and their interpretation of a given HbA1c in terms of its association with mean plasma glucose values. Further information obtained from the questionnaire includes patient's age, type of diabetes, diabetes treatment, home glucose monitoring, current HbA1c levels, satisfaction and perception of their own blood glucose levels. Patients' HbA1c on the day was recorded on the questionnaire so that patients were aware of their current result and would be able to comment on them. Patients were educated about HbA1c by providing patients with written information on the association between HbA1c and mean blood glucose levels in the preceding three months. 8 Glycaemic status was reviewed before and at approximately seven months after such intervention among patients who required further follow-up appointment as clinically indicated within routine clinical care, to assess its impact on patients' glycaemic control. Results were expressed as mean (with standard deviation [SD]) unless mentioned otherwise. Statistical analysis was by Student's t-test and significance was at the level of P < 0.05.
Results
All patients were happy to fill in the questionnaire, but nine did not fully complete their questionnaire and were not included in further analysis. A total of 111 completed questionnaires were included in this analysis (Table 1). The term HbA1c was familiar to 40.5% (45/111; 31 type 1, 14 type 2 diabetes) of patients (F), and 59.5% (66/111; 23 type 1, 43 type 2 diabetes) were unfamiliar with the term (U) (Figure 1). Of those ‘familiar’ with HbA1c, only 13.3% (6/45) were aware of the correct interpretation of a given HbA1c value in terms of its association with mean plasma glucose over the preceding 3 months); the majority, 57.8%, thought that HbA1c of 9% reflected an average blood glucose of 9 mmol/L in the preceding three months and 6.7% (3/45) thought that an HbA1c of 9 correlated with a blood glucose reading of 9 on the same day. After providing information to patients regarding the association between HbA1c level (%) and mean plasma glucose (mmol/L), 84.2% (101/120) declared that the information given to them was new, and 65.8% (79/120) of people felt the information regarding the meaning of HbA1c would favourably influence how they managed their blood sugar levels.
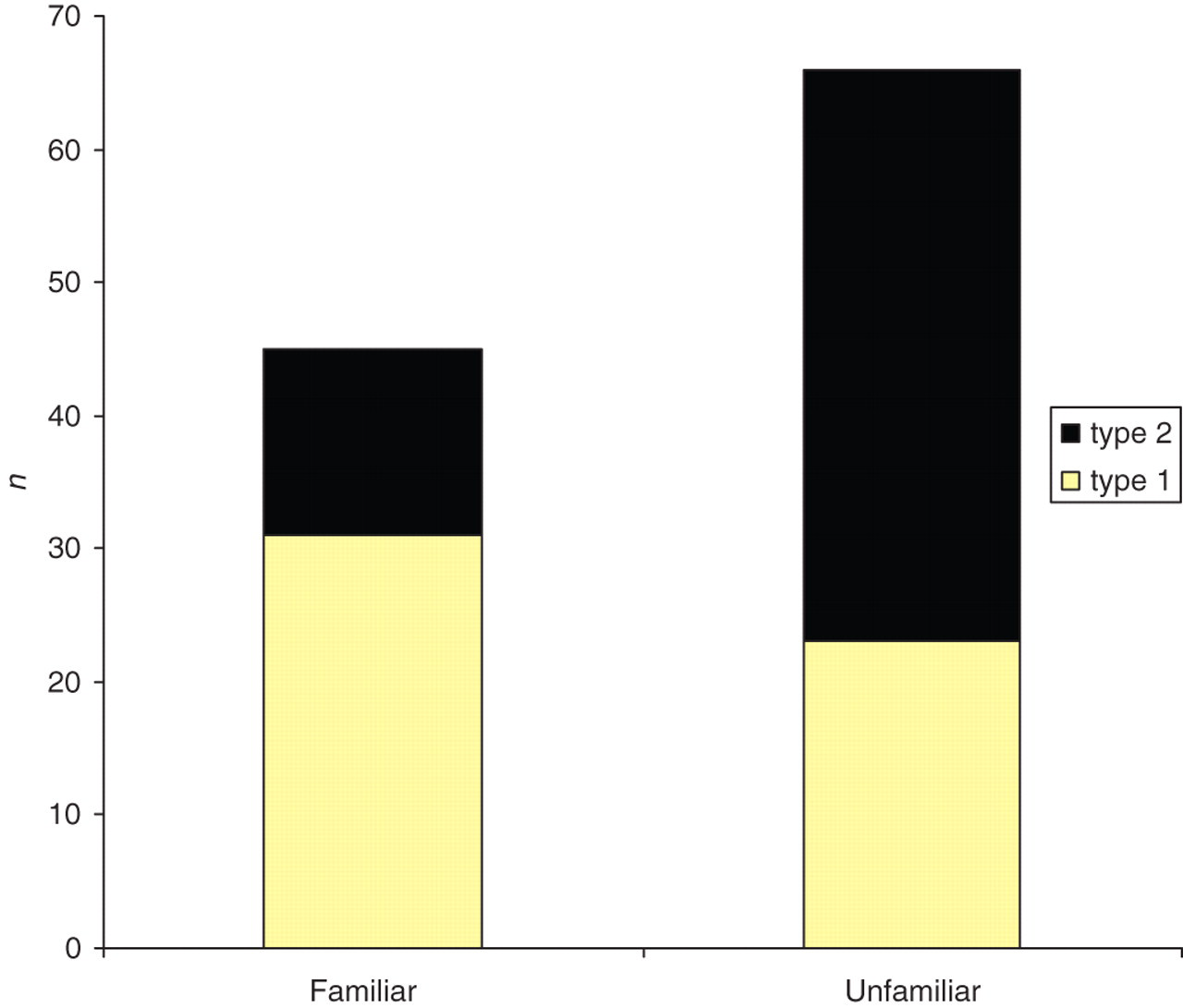
Familiarity with HbA1c and types of diabetes
Baseline clinical features of patients included in this analysis
Total patient group refers to all patients who completed their questionnaire. Followed-up patients group is a subset of the total group who attended follow-up at seven months within routine clinical practice
Follow-up data were available on 80 patients who attended routine follow-up following their previous visit after approximately seven months (Table 1). Results showed a significant reduction in HbA1c levels following the intervention, (mean HbA1c ± SD before and after: 9.3 ± 1.7% vs. 8.7 ± 1.7%, P = 0.05) (Figure 2). When the cohort was stratified into different levels of glycaemia at baseline, patients with moderately poor glycaemic control (HbA1c 7.5–9%), showed no significant change in HbA1c levels following HbA1c information (8.3 ± 0.5% vs. 8.2 ± 1.0%, P = 0.57, n = 29 in group U; 8.3 ± 0.5% vs. 8.2 ± 1.1%, P = 0.79, n = 14 in group F) (Figure 2). However, for patients with very poorly controlled diabetes (HbA1c >9%), intervention produced a significant improvement in glycaemic control among those who were originally unfamiliar with HbA1c (U), (10.7 ± 1.8% vs. 9.5 ± 1.7%, P = 0.04; n = 20) but not among those who were familiar with HbA1c value (F), (10.5 ± 1.8 vs. 9.8 ± 2.1, P = 0.28; n = 17) (Figures 2 and 3). In order to adjust the observed measurement for regression to mean, we used analysis of covariance (ANCOVA) to estimate the mean HbA1c change adjusted for baseline HbA1c in group (U). Our analysis showed similar conclusion with significant reduction in mean HbA1c levels in group U stratified for baseline HbA1c >9%: mean HbA1c reduction: 1.27 ± 0.10; 95% confidence interval (CI) 1.029, 1.504, suggesting that the observation is not likely to be due to the effect of regression to mean.
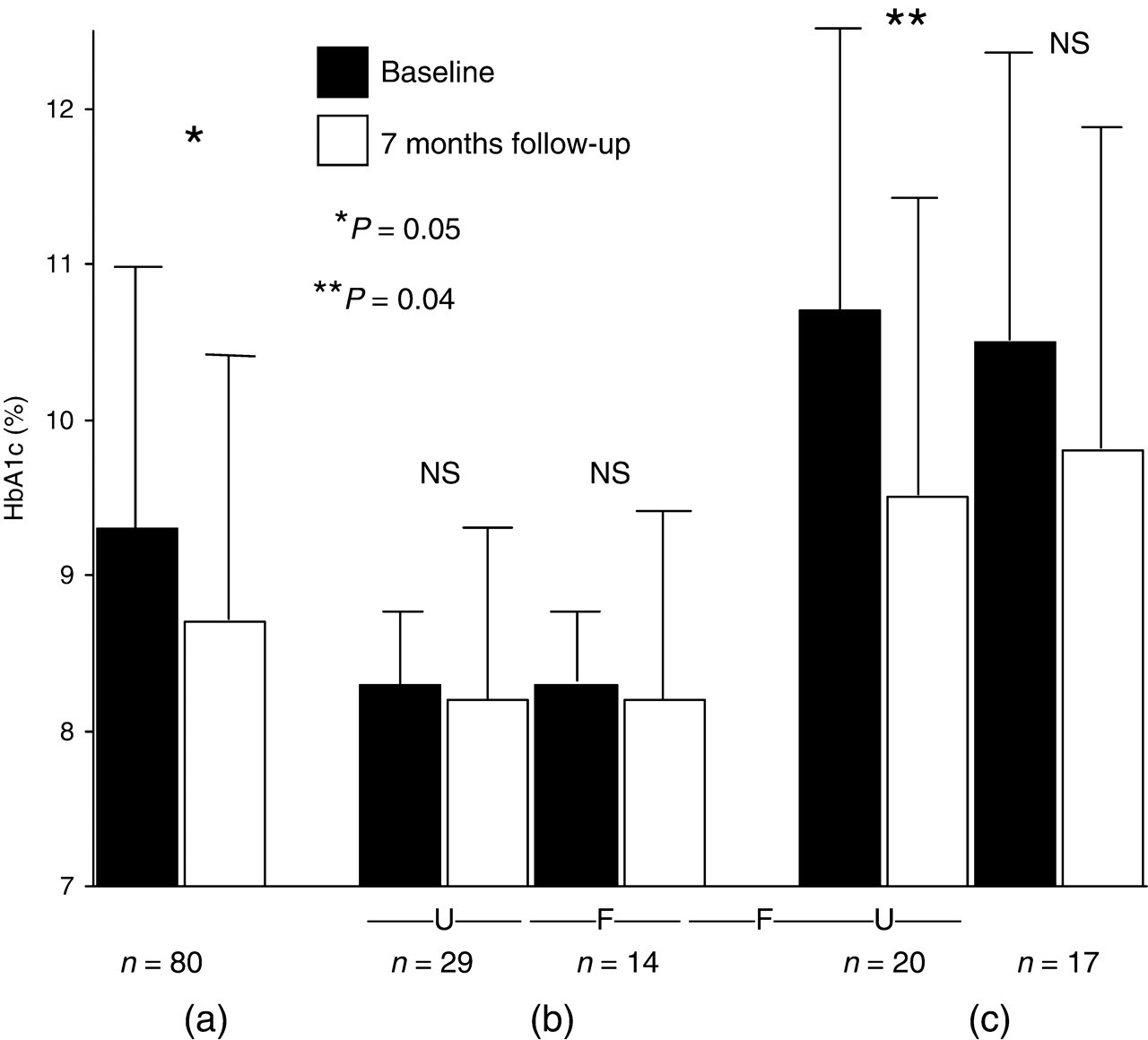
Changes in HbA1c after informing patients about the association between HbA1c and mean plasma glucose. (a) represents the total cohort n = 80; (b) represents patients with moderately poor glycaemic control (HbA1c 7.5–9%; n = 43) and (c) represents patients with poor glycaemic control (HbA1c >9%; n = 37). ‘U’ = unfamiliar and ‘F’ = familiar with the term and meaning of HbA1c before information. Error bars: standard deviation
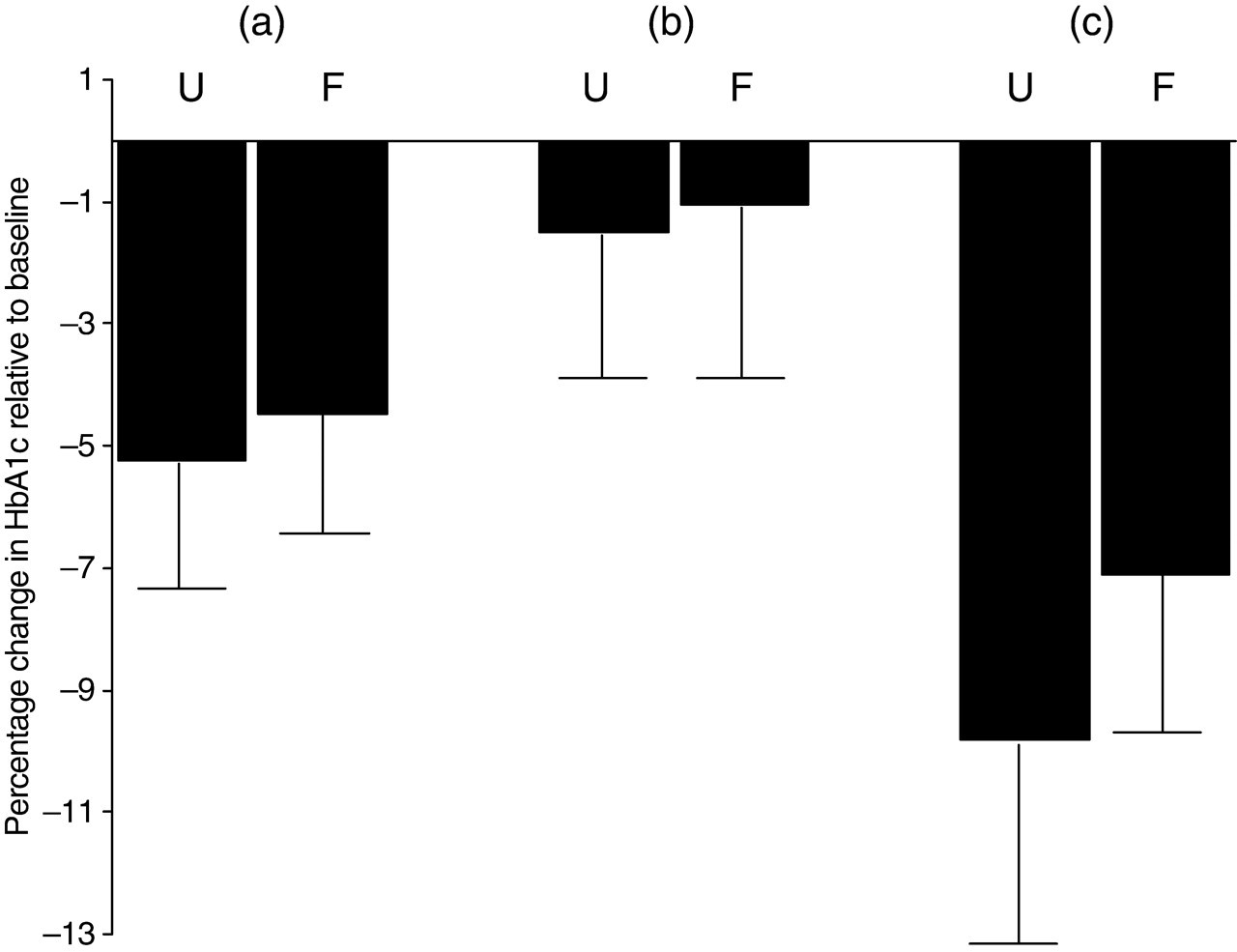
Percentage changes of HbA1c relative to baseline HbA1c values for (a) total cohort n = 80, (b) patients with moderately poor glycaemic control (n = 43) and (c) patients with poor glycaemic control (n = 37). ‘U’ = unfamiliar and ‘F’ = familiar with the term and meaning of HbA1c before information
Discussion
Measurement of HbA1c values is widely used to assess glycaemic control and risks of microvascular complications among patients with diabetes. Since diabetes self-management education is an important component of an effective diabetes care, 3,4 patients' knowledge and understanding of what HbA1c represents is crucial to improving clinical outcomes. 9 The success of such educational interventions has been seen within a randomized controlled trial setting, 10 but its effectiveness within routine clinical practice remains unclear. The importance of this, however, was reflected in the recent considerations by the IFCC in collaboration with the American Diabetes Association (ADA)/European Association of the Study of Diabetes (EASD)/International Diabetes Federation (IDF) working group to universally report HbA1c in the context of mean plasma glucose values. 6,7 Our findings confirmed observations from previous studies that showed patients' knowledge and awareness of HbA1c values are quite poor. 11,12,13 Only a third of patients attending our diabetes clinic were familiar with the term HbA1c. Knowledge about HbA1c was higher among type 1 compared with type 2 diabetes, most likely a reflection of longer disease duration and more intensive education programme. In contrast to other studies, familiarity with HbA1c is not associated with better glycaemic control. 13 Importantly, providing information about the relationship between HbA1c and mean plasma glucose values within routine clinical practice to patients who were unfamiliar with the term HbA1c resulted in a significant improvement in HbA1c values. This observation was not seen among patients who were already familiar with the term HbA1c or in those with good to moderate glycaemic control.
Several limitations need to be highlighted. This is an observational study within routine clinical practice. Patient information and questionnaires were provided by written information and patients' clinical management and follow-up were within routine clinical practice. Thus, all patients received similar specialist input in order to improve their glycaemic control and this did not differ between those who were familiar or unfamiliar with the term HbA1c. Since the majority of patients in our care were insulin treated, clinical input would often include advice on insulin dose adjustment regimes in order to achieve target HbA1c. Similarly, all patients (where appropriate) would have undergone a structured education programme either by diabetes specialist nurses or dietician as part of routine care. The in-house structured education programme that we offer, however, does not formally include education to patients about the association between the mean three-month blood glucose with HbA1c level. Patients who were not followed up in our study were those who were discharged from specialist (hospital) care and thus are likely to have glycaemic control which does not require further specialist intervention. For the same reason, we were unable to assess whether any improvements in HbA1c is sustained after the initial seven months. The multichoice format of our patient assessment questionnaire may introduce bias to patients' response. Consequently, our study merely showed associations with improved glycaemic control as a result of educating patients about HbA1c rather than causality.
In conclusion, patients' knowledge of HbA1c is poor, especially among those with type 2 diabetes. Improvement in patients' knowledge and understanding of HbA1c, particularly among those with very poorly controlled diabetes and no prior understanding of HbA1c is associated with improvements in glycaemic control, at least in the short term. Our finding emphasizes the need for clinicians to engage patients more in understanding and interpreting their HbA1c results and arguably supports current efforts to report HbA1c values in more meaningful units.