
Abstract
Background
Increased triglyceride (TG)-rich lipoproteins and decreased HDL that are implicated in the progression of atherosclerotic vascular diseases, are present in serum samples of patients undergoing haemodialysis (HD) therapy. Therefore, it is important to measure serum TG-rich lipoprotein concentrations to prevent the diseases.
Methods
The cholesterol concentrations of lipoprotein classes in serum samples from the HD patients (n = 18) and healthy subjects (n = 18) were analysed by our recently developed method of high-performance liquid chromatography (HPLC), in which the lipoprotein classes were separated using an anion-exchange column, and the cholesterol concentrations of each of those were measured enzymatically using a post-column reaction. The ability of fractionated lipoprotein cholesterol determination by this HPLC method is mostly equivalent to the determination ability of an ultracentrifugation (UC).
Results
HDL, LDL, and TG-rich lipoproteins, i.e. IDL, VLDL and chylomicrons, were well separated in the chromatograms. HDL cholesterol concentrations in the HD patients were significantly lower than in the healthy subjects (P < 0.0001), and IDL cholesterol concentrations and VLDL cholesterol concentrations in the HD patients were significantly higher than in the healthy subjects (P < 0.05). Profiles of these measured lipoprotein values were consistent with the previously reported lipoprotein values, measured ultracentrifugally characteristic of HD patients.
Conclusion
These results suggest that the HPLC method may be sufficiently applied to the assessment of serum lipoprotein profile in HD patients in place of the other method including an UC.
Introduction
Patients undergoing haemodialysis (HD) therapy over a long term are susceptible to premature cardiovascular diseases. 1 It is also known that cardiovascular disease is a major cause of mortality in HD patients. 2,3 HD patients have a characteristic dyslipidaemia typified by hypertriglyceridaemia. 4–6 Serum lipoprotein fractions of HD patients with dyslipidaemia is characterized by increased concentrations of VLDL and intermediate-density lipoproteins (IDL), mostly normally ranged concentrations of LDL and decreased HDL. 4,5 The increased triglyceride (TG)-rich lipoproteins and decreased HDL are implicated in the progression of atherosclerotic cardiovascular diseases. 4–6 Therefore, it is important to monitor the concentrations of TG-rich lipoproteins in HD patients to prevent cardiovascular diseases. However, TG-rich lipoproteins in HD patients are basically analysed using an ultracentrifugation (UC) method, which is time-consuming and laborious. It is known that the other methods, including gel-permeation chromatography and electrophoresis, have a poor ability to separate heterogeneous TG-rich lipoproteins. 7,8 We have recently developed a convenient method for analysing serum fractionated lipoprotein classes by high-performance liquid chromatography (HPLC) with an anion-exchange column, which has a high ability to separate TG-rich lipoproteins, IDL, VLDL and chylomicron. 9 In our developed HPLC method, cholesterol concentrations of HDL, LDL, IDL, VLDL and chylomicron were highly correlated with those estimated by the UC method. 9 Therefore, we attempted to measure cholesterol concentrations of TG-rich lipoprotein classes in HD patients using the HPLC method.
Methods
The study samples were obtained from HD patients (n = 18) and the same number of age-matched healthy subjects after a 12 hour-overnight fast. Their clinical characteristics were shown in Table 1. The HD patients included subjects with diabetes mellitus (n = 11) and chronic glomerulonephritis (n = 7), and were undergoing thrice-weekly three- to four-hour HD therapy using high-flux polysulphone dialysis membranes (Toray Medical Co., Tokyo, Japan) and standard heparin doses for anti-coagulation.
Characteristics and lipoprotein profiles of haemodyalysis patients and healthy subjects
NS, non-significant; BP, blood pressure
The column size and the flow rates in the HPLC method reported previously 9 was partially modified, and used for measuring cholesterol concentrations of serum lipoprotein classes (HDL, LDL, IDL, VLDL and chylomicron) The anion-exchange column, which contained 2.5 μm of non-porous polymer-based gel with diethylaminoethyl ligands, and 3.0 mm ID × 25 mm in size, and a post-column reactor, which contained an enzymatic cholesterol reagent (TCHO-CL, Serotec Co., Hokkaido, Japan), were used for the modified HPLC method. The flow rates of eluent and the enzymatic cholesterol reagent were 0.5 mL/minute and 0.2 mL/minute, respectively. It took 23 minutes to complete the assay of one sample. Serum sample (4.5 μL) was injected to the column, and lipoprotein classes in the sample were eluted by a step-gradient of perchlorate ion concentrations in order. Serum sample (500 μL) was mixed with 250 μL of the stock solution (sucrose 760 g/L, EDTA2K 1.5 g/L), and stored at −40°C until measured. The stored samples were analysed within one month. The coefficient data of variation in between-day assay (n = 10) and within-day assay (n = 10) using hyperlipidaemic serum samples by this HPLC method were as follows: HDL cholesterol 3.2 and 1.8%, LDL cholesterol 3.2 and 2.0%, IDL cholesterol 7.3 and 3.4%, VLDL cholesterol 5.0 and 3.3% and chylomicron cholesterol 7.5 and 6.1%, respectively.
Total cholesterol, TG, and creatinine concentrations were measured enzymatically with commercially available kits (Daiichi Pure Chemical Industries, Tokyo, Japan). Apolipoprotein concentrations were measured by immuno-nephelometry with commercial kits (Daiichi Pure Chemical Industries).
Results were expressed as mean ± SD. The comparative significance of variables between the different groups was assessed with an unpaired Welch's t-test. A value of P < 0.05 was considered statistically significant.
Results
Figure 1 shows the typical chromatograms of serum samples from the two HD patients and the healthy subject. In the chromatograms, HDL, LDL, IDL, VLDL and chylomicron were sufficiently separated.
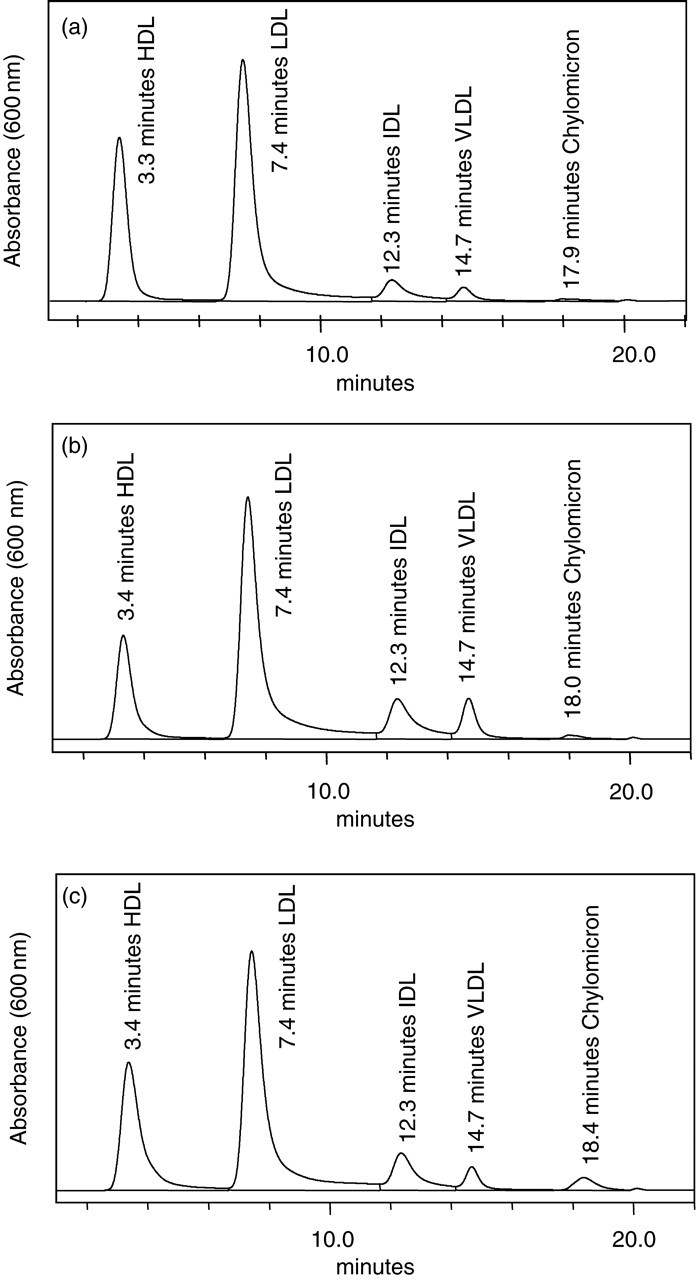
Chromatograms in serum samples from haemodialysis (HD) patient and healthy subject. Part figures a, b, and c are chromatograms of a healthy serum (a) and serum samples of two HD patients' (b and c), respectively. The basic data of sex, age and cholesterol concentrations of HDL, LDL, IDL, VLDL and chylomicrons were as follows: (a) male, 65, 1.58 mmol/L, 3.06 mmol/L, 0.305 mmol/L, 0.148 mmol/L and 0.031 mmol/L; (b) male, 62, 0.94 mmol/L, 2.83 mmol/L, 0.506 mmol/L, 0.344 mmol/L and 0.039 mmol/L; (c) female, 61, 1.12 mmol/L, 2.23 mmol/L, 0.393 mmol/L, 0.155 mmol/L and 0.144 mmol/L, respectively
Body mass index, total cholesterol and apolipoprotein A1 of the HD patients were significantly lower than those of age- and sex-matched healthy subjects (P < 0.05, P < 0.05 and P < 0.0001, respectively), while systolic BP, creatinine and TG of the HD patients were significantly higher than those of the healthy subjects (P < 0.001, P < 0.0001 and P < 0.001, respectively) as shown in Table 1. In the HPLC analysis, HDL cholesterol concentrations of the HD patients were significantly lower than those of the healthy subjects (P < 0.0001), and IDL and VLDL cholesterol concentrations of the HD patients were significantly higher than those of the healthy subjects (P < 0.05) (Table 1).
Discussion
HDL, LDL, VLDL and chylomicron in human serum samples can be well separated using gel-permeation chromatography or agarose-gel electrophoresis, but IDL cannot be sufficiently separated. 7,8 Therefore, we conducted the separation of lipoprotein classes in human serum samples by the HPLC method with the anion-exchange column, and two HDL peaks, one broad LDL peak, one small IDL peak and one broad VLDL peak can be insufficiently separated in a hyperlipidaemic serum using the anion-exchange chromatography with 0–155 mmol/L linear gradient of sodium perchlorate (data not shown). Hence, we established the novel anion-exchange chromatographic method with a step-gradient of sodium perchlorate concentration for the sufficient separation of HDL, LDL, IDL, VLDL and chylomicron in human serum. 9 The present study attempted to analyse lipoprotein profiles of HD patients using the HPLC method.
In the present study, HDL cholesterol concentrations were significantly lower, and IDL and VLDL cholesterol concentrations were significantly higher in the HD patients than age- and sex-matched control subjects. In addition, LDL cholesterol concentrations were modestly but insignificantly lower in the HD patients compared with the control subjects. Using the UC method, Shoji et al. 4,5 reported that HDL and LDL cholesterol concentrations were significantly lower, and IDL and VLDL cholesterol values were significantly higher in HD patients than in control subjects. Quaschning et al. 6 reported that when compared four groups of HD patients (HD-NTG group, normotriglyceridaemic HD patients without diabetes mellitus; HD-HTG group, hypertriglyceridaemic HD patients without diabetes mellitus; HD-NIDDM-NTG group, normotriglyceridaemic HD patients with non-insulin-dependent diabetes mellitus; HD-NIDDM-HTG, hypertriglyceridaemic HD patients with non-insulin-dependent diabetes mellitus) with control subjects, HDL cholesterol concentrations were significantly lower in HD-HTG and HD-NIDDM-HTG groups than in control subjects, LDL cholesterol concentrations were similarly calculated between the four groups of HD patients and control subjects, and VLDL cholesterol concentrations were significantly higher in HD-HTG, HD-NIDDM-NTG and HD-NIDDM-HTG groups than in control subjects, revealed by the UC method.
In the UC method, 200 μL of plasma was mixed with the appropriate density solution with potassium bromide, and the sample was spun in three hours. 4,5 The HPLC method required only a small volume of sample (4.5 μL) to determine the cholesterol concentrations of major lipoprotein classes. In addition, the assay time of one sample was merely 23 minutes in the HPLC method, so that subsequently any alteration of sample lipoproteins may be little found during the course of lipoprotein separation in the HPLC assay in contrast to the UC method which may have the possibility of altering lipoproteins because of requiring long assay times.
Recently, non-HDL cholesterol (total cholesterol − HDL cholesterol) has been proposed as a risk marker for cardiovascular diseases. 10,11 Several epidemiologic studies have shown that non-HDL cholesterol is a better predictor of cardiovascular events than LDL cholesterol, and that non-HDL cholesterol is a potential predictor of risk for carotid atherosclerosis in the elderly. 12–14 Nishizawa et al. 15 have reported that non-HDL cholesterol was a significant and independent predictor of cardiovascular mortality in HD patients. Precise measurement of non-HDL cholesterol may be more useful in HD patients with elevated TG, because HD patients have normal concentrations of LDL cholesterol in contrast to increased TG-rich lipoproteins. In HD patients, IDL and VLDL cholesterol presumably account for major part of non-HDL cholesterol. Furthermore, several studies have reported that increased concentrations of VLDL and IDL were associated with the increased cardiovascular risk. 16–21 Koba et al. 16 reported that an increased number of VLDL particles was strongly associated with coronary heart disease in men. Tatami et al. 17 also reported that moderately increased concentrations of IDL cholesterol were closely associated with a high frequency of coronary heart disease in consecutive patients evaluated by selective coronary cineangiography. Therefore, because the precise measurement of IDL and VLDL cholesterol is likely to be useful for cardiovascular risk assessment in HD patients, our convenient HPLC assay for IDL and VLDL cholesterol may be helpful in clinical practice for HD patients.
In conclusion, HD patients have the impaired lipoprotein metabolism characteristic of the elevated TG-rich lipoproteins (IDL and VLDL) in lipoprotein profiles analysed by our developed HPLC method, of which data were consistent with those shown by the other study groups with the UC method. HPLC chromatograms show the excellent separation of TG-rich lipoproteins. Taken together, our developed HPLC method may be sufficiently applied to the routine assay for TG-rich lipoproteins in clinical practice for the diagnosis and treatment of dyslipidaemia to prevent atherosclerotic cardiovascular diseases in HD patients.
GRANT/FUNDING SUPPORT
The present study was supported by a grant from Tosoh Corporation and the Jikei University Research Fund.
Footnotes
ACKNOWLEDGEMENTS
We wish to thank Mika Komori and Yukako Uchihashi for their excellent technical assistance.