
Abstract
Circulating sodium concentration is commonly measured by both direct and indirect ion-sensitive electrode (ISE). We describe an unusual case with a high elevation of serum glucose (162 mmol/L) where direct ISE sodium measurement was 9 mmol/L higher than the indirect measurement in the absence of any cause for pseudohyponatraemia. In vitro experiments showed that very high glucose concentrations increased the sodium in direct, but not in indirect ISE measurement. This effect was insufficient to account for the entire difference between the measurements seen in the patient, indicating that other factors, for example pH and bicarbonate concentration, must also be involved. This effect may influence interpretation of sodium status in patients with gross hyperglycaemia.
Introduction
The measurement of serum sodium by ion-sensitive electrode (ISE) is routinely performed using either direct or indirect methods. In general, these methods are extremely robust to analytical interferences, however, differences between these two methods may be caused by high concentrations of serum protein or lipid causing lowered results on indirect analysis known as pseudohyponatraemia. 1 In addition, the opposite effect can occur with low concentrations of protein in a sample. 2
We present a case with a marked difference between direct and indirect ISE sodium results in a patient with severe hyponatraemia secondary to extreme hyperglycaemia that was not explained on the basis of known interferences. This phenomenon has been observed elsewhere. 3 This observation prompted the investigation of the effect of glucose on the measurement of serum sodium with direct and indirect ISE.
Case report
A 23-year-old woman with insulin-dependent diabetes mellitus was presented to the Emergency Department after presumed drug overdose. Initial pathology results showed marked hyperglycaemia (serum glucose 162 mmol/L) and severe hyponatraemia, with a difference between direct and indirect ISE (109 mmol/L on direct ISE and 100 mmol/L on indirect ISE). The total protein was 59 g/L and triglycerides were 9.1 mmol/L, excluding significant pseudohyponatraemia and a severe metabolic acidosis was present with a pH of 6.98, serum bicarbonate of 7 mmol/L and base excess of −22 on blood gas analysis. Other results included whole blood β-hydroxybutyrate of 5.4 mmol/L, lactate of 5.6 mmol/L, serum osmolality of 444 mmol/L, urea 21.8 mmol/L and potassium 6.3 mmol/L. The patient was treated with insulin and fluid resuscitation and had a good recovery with normalization of serum sodium concentration 10 hours after presentation. The sodium measurements on direct and indirect ISE at this time were 141 and 142 mmol/L, respectively, at a glucose concentration of 34 mmol/L and pH of 7.34. Further treatment led to normalization of serum glucose (Figure 1).
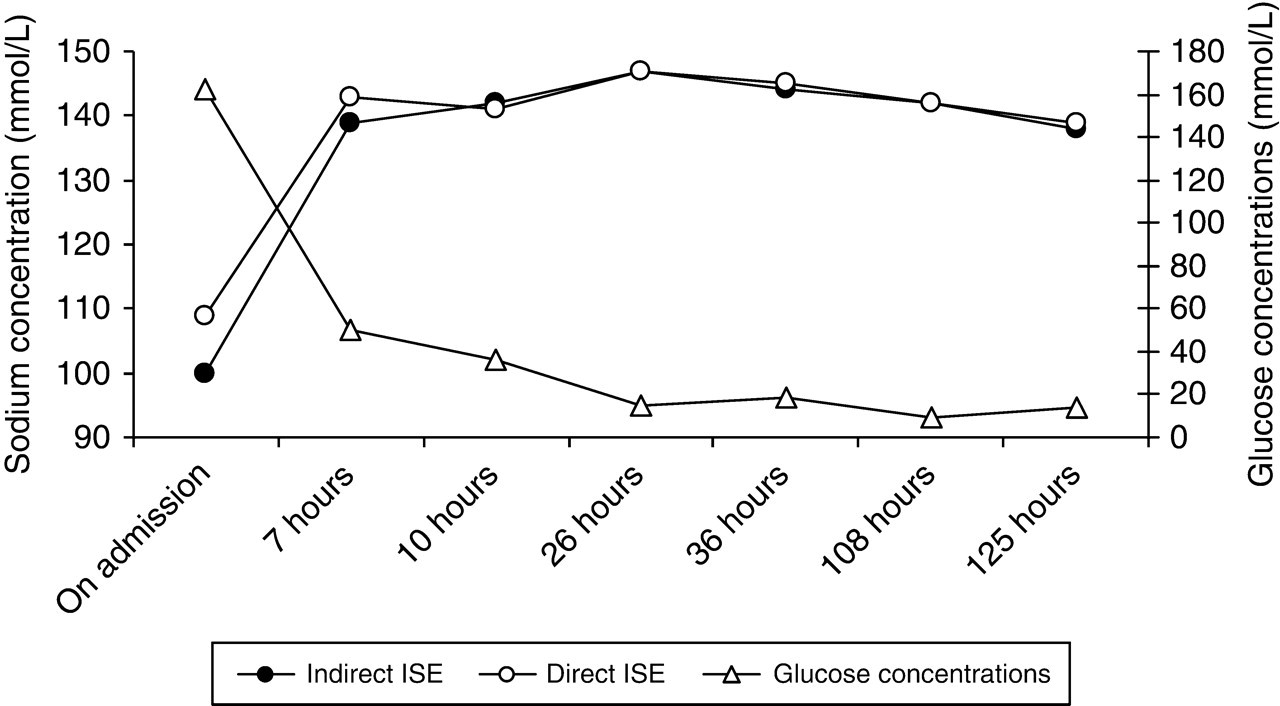
Index case results for sodium and glucose
Further investigation
Before proceeding with the investigation of the difference between direct and indirect sodium measurement, we sought to eliminate any possibility of analytical errors. We confirmed that both the direct ISE (ABL 725 analyser, Radiometer Australia) and the indirect ISE (Modular P analyser, Roche Diagnostics, Australia) were operating satisfactorily on the admission day by reviewing both internal quality control (QC) data and other patient results. We also excluded systematic bias at low sodium concentrations by reviewing the results of other patients in our pathology database having very low sodium and normal glucose concentrations (n = 3), and by measuring of sodium using both methods in patient samples with high protein diluted to give low sodium and normal protein concentrations (n = 4, data not shown).
After confirming satisfactory performance of both the analysers, the difference between the direct and indirect ISEs was assessed by performing an in vitro experiment, whereby variable glucose concentrations were added to serum pools and to saline aliquots, and the measurement of sodium performed using the direct and indirect ISEs. As the concentration of glucose in the samples was increased from 5.8 to 161 mmol/L, we observed a progressive increase in sodium measurements in the direct ISE method (slope 0.021 mmol/L sodium per mmol/L glucose, 90% confidence limits [CI] 0.016–0.025) without significant change in indirect results (slope −0.044 mmol/L sodium per mmol/L glucose, 90% CI −0.009 to 0.005). The results from these in vitro experiments are shown in Figure 2 together with the results from the index case and other patients with high serum glucose identified from our pathology database. The slope for the line of best fit for the difference between direct and indirect sodium results for the in vitro study is 0.021 mmol/L sodium per mmol/L glucose with 90% CI being 0.019–0.0319. La Milia et al. 4 showed a similar response of direct ISE sodium measurements to very high glucose concentrations using peritoneal dialysis solutions; however, the effect was less marked.
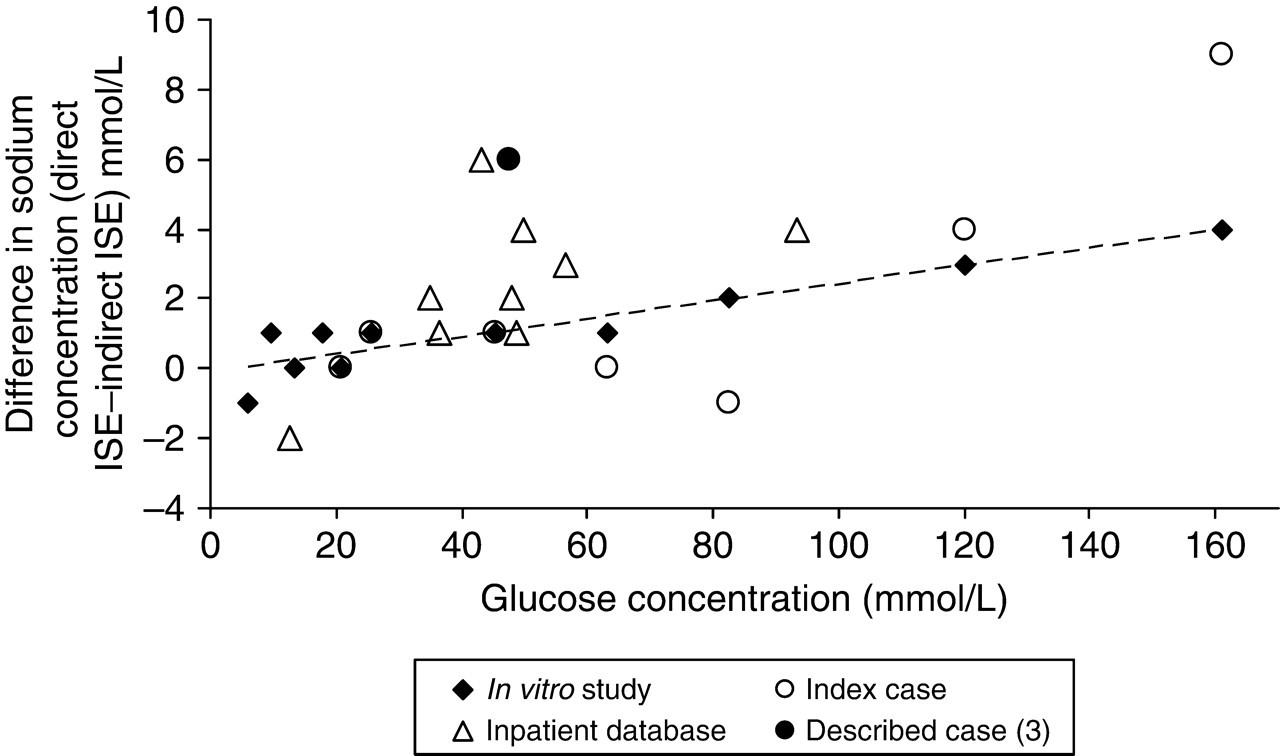
Bias plot showing the differences between direct and indirect ion-sensitive electrodes for the index case, patients with hyperglycaemia, and in vitro glucose addition. The dashed line is the line of best fit for the in vitro study
Discussion
Pseudohyponatraemia in indirect ISE measurements is caused by hyperproteinaemia and hypertriglyceridaemia. The effect is ascribed to changes in the solid content of the plasma or serum specimen producing smaller amounts of water per unit volume of the sample and direct ISE is considered to provide reliable analysis in these patients. 2 In diabetic patients, severe hyperglycaemia may result in dilutional hyponatraemia where water shifts from the intracellular space to the extracellular space under the osmotic influence of hyperglycaemia. In our case, we observed an overall reduction in the measured sodium consistent with dilutional hyponatraemia, which was more marked in indirect ISE when compared with direct ISE. As the glucose concentration was lowered with insulin therapy, the sodium concentrations increased and the difference between the methods resolved. This is qualitatively consistent with the in vitro results where the presence of high concentrations of glucose produced an increase in sodium measurements by direct ISE.
The effect of glucose seen experimentally was not sufficient to quantitatively account for the increased difference between direct and indirect ISE seen in patient samples. Therefore, additional factors should be considered. A factor that may influence sodium measurement in patient samples is the low pH of the patient. 4,5 As a fraction of serum sodium is bound to bicarbonate in plasma, and direct ISE does not measure this fraction, a fall in bicarbonate may increase measured (unbound) sodium by direct ISE, but not by indirect ISE which measures total sodium. The expected effect of this in our patient would be about +3 mmol/L. 5
In clinical practice, sodium concentrations are used in the assessment of sodium and water status, calculating the osmolar gap and the anion gap and, in the setting of high glucose, predicting serum sodium after normalization of the serum glucose. Using a common correction formula,
6
the indirect ISE provided a better prediction of post-treatment sodium (144 mmol/L) than the direct ISE (153 mmol/L). The authors of this formula do not specify the method used for their data, but in 1973, it is likely that flame photometry was in use, which closely matches the indirect ISE measurements.
6

The effect is also significant in other calculations, e.g. anion gap 33 mmol/L (indirect), 42 mmol/L (direct) and osmolar gap 60 mmol/L (direct) and 42 mmol/L (indirect).
The other case described 3 showed sodium on direct ISE 135 mmol/L, indirect ISE 127 mmol/L, glucose 48 mmol/L and total protein of 98 g/L. The difference in sodium measurements after accounting for the high protein is also more than that accounted for by glucose alone (Figure 2).
In summary, we present evidence that glucose, when present at higher concentrations, can produce an artefactual increase in the measurement of sodium concentration by direct ISE although other factors in the patients may further contribute to differences between direct and indirect sodium ISE results. Further work is required to clarify the effect of sodium measurement method on common equations involving serum sodium measurements when very high glucose concentrations are present.
Footnotes
ACKNOWLEDGEMENTS
The contents of this paper have been presented in poster format at the Australasian Association of Clinical Biochemistry Annual Scientific Meeting in Melbourne, September 2007.