
Abstract
Abstract
It is crucially important to detect subarachnoid haemorrhage (SAH) in all patients in whom it has occurred to select patients for angiography and preventative surgery. A computerized tomography (CT) scan is positive in up to 98% of patients with SAH presenting within 12 h, but is positive in only 50% of those presenting within one week. Cerebrospinal fluid (CSF) bilirubin spectrophotometry can be used to determine the need for angiography in those few CT-negative patients in whom clinical suspicion of SAH remains high; it may remain positive up to two weeks after the event. A lumbar puncture (LP) should only be performed >12 h after the onset of presenting symptoms. Whenever possible collect sequential specimens. Always ensure that the least blood-stained CSF sample taken (usually the last) is sent for bilirubin analysis. Protect the CSF from light and avoid vacuum tube transport systems, if possible. Always use spectrophotometry in preference to visual inspection. All CSF specimens are precious and should always be analysed unless insufficient sample is received. Centrifuge the specimen at >2000 rpm for 5 min as soon as possible after receipt in the laboratory. Store the supernatant at 4°C in the dark until analysis. An increase in CSF bilirubin is the key finding, which supports the occurrence of SAH but is not specific for this. In most positive cases, bilirubin will occur with oxyhaemoglobin.
Introduction
Subarachnoid haemorrhage (SAH) is spontaneous arterial bleeding into the subarachnoid space, usually from a cerebral aneurysm. 1 Patients who have bled and in whom the diagnosis is initially missed often present with a further bleed, in a poorer condition and with a worse outcome than those in whom the correct diagnosis is made promptly. 2,3 It is thus crucially important to detect SAH in all patients in whom it has occurred.
The initial investigation – the demonstration of blood on a computed tomography (CT) scan – will, in experienced hands, be positive in 98% of patients with SAH presenting within the first 12 h after an event, 4 but positivity falls with time to about 50% in patients presenting after one week. 5 Patients with a positive CT usually proceed to angiography, a resource-intensive procedure, to confirm the presence of an aneurysm and locate its site so that it can be treated to prevent a re-bleed. There is a need for a procedure for detecting those CT-negative patients presenting with a history suggestive of SAH who actually have sustained SAH, 4 and to eliminate the possibility of SAH in the remainder without the need for angiography. Best estimates are that a UK hospital may see up to 150 patients per annum with symptoms of SAH who are CT-negative; some 2–3% of these will be proven to have a ruptured aneurysm. 4
Following haemorrhage into the CSF, red blood cells undergo lysis and phagocytosis; the liberated oxyhaemoglobin is converted in vivo in a time-dependent manner into bilirubin, 6 and sometimes methaemoglobin. 7 Of these three pigments, only bilirubin arises solely from in vivo conversion. However, CSF bilirubin will also be increased when CSF total protein or serum bilirubin is increased. Oxyhaemoglobin and methaemoglobin may both be produced in vitro as well as in vivo. 8
Bilirubin may be detected in CSF by spectrophotometry or by visual inspection for the yellow discoloration (xanthochromia) it imparts to CSF. Evidence clearly indicates that visual inspection is not a reliable method. 9,10 Analysis of bilirubin in CSF using diazo methods has not been adequately validated and should not be used.
We now propose revised guidelines for the specimen requirements, transport, handling and analysis of CSF and interpretation in suspected SAH with a negative CT scan. Notes to these guidelines, printed as Appendix 1, provide the reasoning behind our recommendations.
Specimen requirements and transport
A protocol for specimen requirements and transport is provided in Appendix 1, although modification may be required to meet local needs. Essentially, the requirements are:
CSF samples should ALWAYS be analysed if sufficient sample is received. The specimen for spectrophotometry should be the least blood-stained fraction of CSF to be taken (usually the last and ideally at least the fourth [Note a]). The volume requested must be that which enables the analysis to be undertaken without dilution (Note b), and will be determined by local requirements. The specimen should be protected from light (Note c). Use of pneumatic tube systems to transport the specimen to the laboratory is best avoided,
11
but the overriding consideration is rapid transport of the sample to the laboratory (Note a). A simultaneous blood specimen should be taken for serum bilirubin and total protein measurement. The timing of sampling relative to that of possible haemorrhage should be recorded. This should be no less than 12 h (Note d).
It is advised that prospective protocols are discussed with users of the service.
Specimen handling
The specimen designated for spectrophotometry should be centrifuged at >2000 rpm for 5 min as soon as possible after receipt in the laboratory and in any case within 1 h of collection. The supernatant should be stored in the dark at 4°C until analysis (Note c).
Analysis
Perform a zero-order spectrophotometric scan on the supernatant between 350 and 600 nm using a recording spectrophotometer and a cuvette with a 1 cm path length. Use an initial full-scale deflection (FSD) of 0.1 absorbance units (AU). If any peaks exceed 0.1 AU, scale as appropriate but never use an FSD < 0.1 AU (Note e). The specimen should not be diluted.
Oxyhaemoglobin: absorbance maximum between 410 and 418 nm.
Bilirubin: either a broad peak in the range 450–460 nm or a shoulder adjacent to an oxyhaemoglobin peak if present.
Methaemoglobin: the rarest pigment and if present usually manifests as a broader peak than oxyhaemoglobin, occurring between 403 and 410 nm. Draw a predicted baseline, which forms a tangent to the scan between 350 and 400 nm and again between 430 and 530 nm. This baseline should never cut the scan. Measure the absorbance of the scan above this predicted baseline at 476 nm; this is the NBA. If the baseline forms a tangent to the scan before 476 nm, then the measured NBA is by definition zero. Also measure the absorbance of any oxyhaemoglobin peak above this predicted baseline; this is the net oxyhaemoglobin absorbance (NOA).
Inspect the scan and identify and record the presence of the following haem pigments:
Calculate the net bilirubin absorbance (NBA) according to Chalmers' modification
12
to the original method of Chalmers and Kiley
13
as follows (Note f):
Illustrative zero-order spectra are shown in Figures 1a–e.
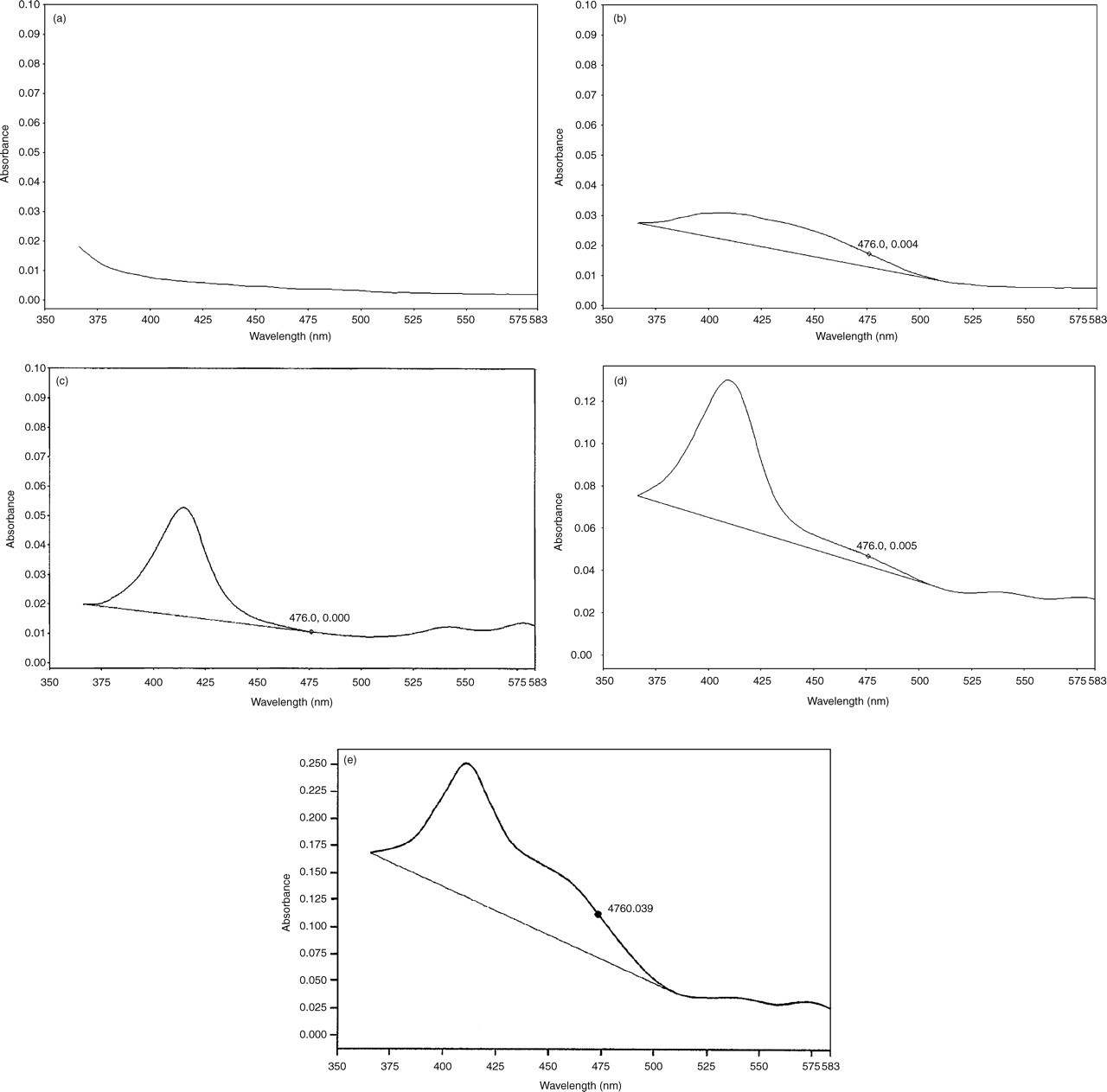
Representative spectrophotometric scans showing net bilirubin absorbance (NBA) at 476 nm above a tangential baseline as described in the text. 1(a) A normal cerebrospinal fluid with essentially no bilirubin; scan and baseline (not drawn) are superimposable. 1(b) NBA within the reference range. 1(c) Oxyhaemoglobin with zero NBA. 1(d) Oxyhaemoglobin with NBA within the reference range. 1(e) Oxyhaemoglobin with an increased NBA. In practice, such scans are best visualized filling the whole of an A4 page in landscape mode
Reporting and interpretation
The following is the most appropriate advice that we can provide regarding reporting and suggested interpretative comments. For each case, the final interpretation should take into account the available clinical information and the known dynamic production of haem pigments following a bleed as outlined in the Introduction. Following SAH, the appearance of the CSF may be bloodstained and the CSF protein may be raised. Bilirubin is the key spectrophotometric finding. Most positive cases exhibit both bilirubin and oxyhaemoglobin. Bilirubin occurring on its own would not be expected within the first few days, but becomes an increasingly possible finding as the second week progresses.
NBA ≤ 0.007 AU and NOA ≤ 0.02 AU
Report as: ‘Bilirubin and oxyhaemoglobin not increased. No evidence to support SAH.’
NBA ≤ 0.007 AU and NOA >0.02 AU but <0.1 AU
Report as: ‘Bilirubin not increased. Small amount of oxyhaemoglobin detected. No evidence to support SAH.’
NBA ≤ 0.007 AU and NOA ≥ 0.1 AU
Report as: ‘Oxyhaemoglobin is present in sufficient concentration to impair the ability to detect bilirubin. SAH not excluded.’
NBA > 0.007 AU and NOA ≤ 0.02 AU or NOA > 0.02 AU but with no visible oxyhaemoglobin peak (a) Serum bilirubin ≤20 μmol/L and CSF protein ≤1.0 g/L.
Report as: ‘Increased CSF bilirubin. Consistent with SAH.’ (This would be an unusual pattern within the first week after an event.)
(b) Serum bilirubin >20 μmol/L and CSF protein ≤1.0 g/L.
Apply formula to calculate an adjusted NBA (Appendix 2).
If adjusted NBA > 0.007 AU
then report as: ‘Increased CSF bilirubin. Consistent with SAH.’ (This would be an unusual pattern within the first week after an event.)
If adjusted NBA ≤ 0.007 AU
then report as: ‘Increased CSF bilirubin but probably totally accounted for by increase in serum bilirubin. Not supportive of SAH.’
(c) CSF protein >1.0 g/L, whatever the serum bilirubin.
Report as: ‘Increased CSF bilirubin. This finding may be consistent with: SAH; an increased bilirubin accompanying the increased CSF protein; or other source of CSF blood. Interpret result with caution in relation to SAH especially if within first week of event.’
NBA >0.007 AU and NOA >0.02 AU with visible oxyhaemoglobin peak
Report as ‘Bilirubin and oxyhaemoglobin increased. Consistent with SAH’
Methaemoglobin detected
This is an unusual finding and probably related to artefactual conversion of oxyhaemoglobin (Note k). Therefore, when methaemoglobin is present, the significance of the finding is the same as if oxyhaemoglobin had been detected.
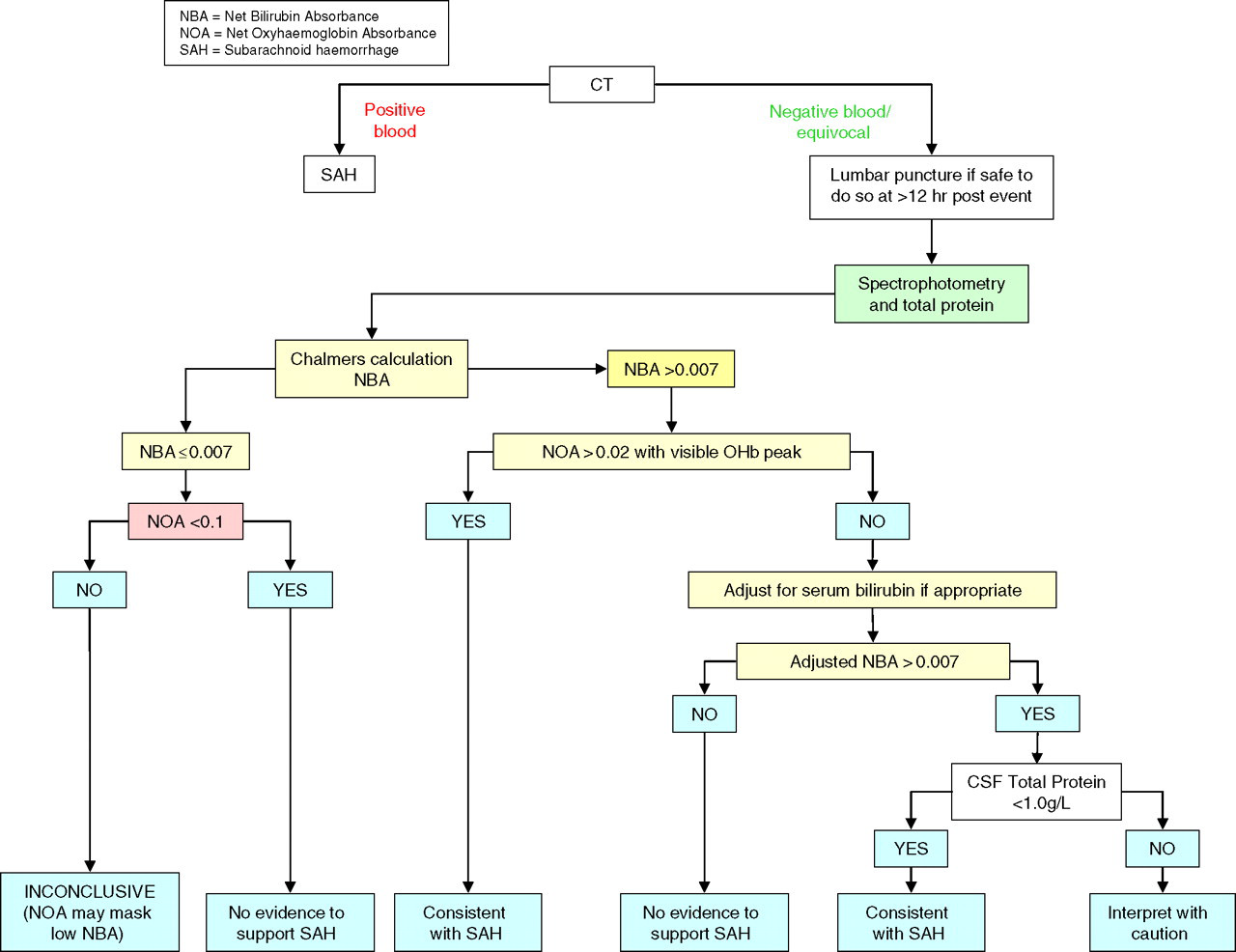
Decision tree
A decision tree (Figure 2) outlines the steps involved in producing the key laboratory information for the detection of a subarachnoid bleed.
Bilirubin absorbance in cerebrospinal fluid for detection of intra-cranial bleed
Standards based on these guidelines
The laboratory should provide instructions for users which provide details of requesting, specimen requirements, transport and interpretation (see example in Appendix 1). There should be standard operating procedures (SOPs) in place for specimen handling, analysis, reporting and interpretation. The laboratory must participate in an appropriate external quality assurance scheme. It is unlikely that a laboratory will build up sufficient expertise unless a minimum of 25 specimens are analysed annually. The nature of the analytical service that a laboratory provides, e.g. whether it is available only within certain hours or at all times, will be dependent upon local needs. In particular, these will be determined by the tertiary centre's referral policy, access to its beds and availability of angiography. Both the analytical and interpretative aspects of the service should be provided together. To meet the requirements of clinical governance all spectrophotometric scans should be kept in an appropriate form for recall for a minimum of two years. Spectrophotometers should be serviced regularly and undergo regular absorption and wavelength checks.
Notes to the guidelines
In addition to the oxyhaemoglobin which appears after a SAH, it also commonly arises either from the in vitro lysis of red cells in the CSF obtained following puncture, or from the trauma of the puncture itself. As explained in note (g) below, such oxyhaemoglobin may interfere with the detection of bilirubin and is a confounding element in interpretation. Therefore every effort should be made to eliminate it. It is for this reason that CSF taken for spectrophotometry should be collected into a separate container to those in which the first few mL of fluid are placed, and why transport by pneumatic tube is not recommended. As explained in note (j) even small increases above the reference range are sufficient to be consistent with a SAH and therefore indicate the need for angiography. Dilution of the specimen will decrease the certainty with which such increases may be detected. Stability studies have shown that CSF stored in a plastic tube and exposed to spring daylight through a north-facing window showed a bilirubin decay rate of at least 0.005 AU/h. CSF specimens must therefore be protected from light to avoid this phenomenon, which may lead to false-negative results. Current consensus is that CSF should not be examined for bilirubin earlier than 12 h after an event. This is based on two strands of evidence.
That bilirubin forms 9–15 h after a bleed.
6,14
We have been unable to review the evidence on which this statement has been made. That in a series of 111 patients positive for blood on CT, all subject to LP after 12 h, xanthochromia was present in all.
15
This evidence must be reviewed with caution due to the ambiguous definition of xanthochromia. Derivative spectroscopy has been found to be of value by some analysts, but requires considerable experience in interpretation. It is therefore not recommended. We have confirmed that, on 58 CSF specimens with bilirubin NBA 0.003–0.251 (24 of which contained oxyhaemoglobin in addition to bilirubin), there was no significant difference between the NBA obtained by the original Chalmers and Kiley method
13
and that by the modification of Chalmers.
12
Out of 740 spectrophotometric scans reviewed from CT-negative patients in four participating centres, 425 had no oxyhaemoglobin and ≤0.007. Angiograms were performed in 31 of these 425 patients and no aneurysms were found. From the same series, 204 CSFs were reported as containing oxyhaemoglobin with NBA ≤ 0.007. Twenty-nine of these patients had angiography. In only two instances was an aneurysm found and in one of these the NOA was >0.1 AU. Experiments using a combination of increasing bilirubin and oxyhaemoglobin concentrations have indicated that at an NOA of >0.1 AU there begins to be an under recording of NBA. Originally, Chalmers and Kiley
13
indicated a reference range for NBA of 0–0.007; values 0.010–0.015 were classed as equivocal and values >0.015 as positive. In the series quoted above, CSFs from three patients with proven ruptured aneurysms have yielded NBA of 0.008, 0.015 and 0.016. In addition, we are aware of three CT-positive patients with proven aneurysms where the CSFs have yielded NBA of 0.008, 0.012 and 0.019. We therefore recommend that values of a NBA > 0.007 are a clear indication for angiography. In the series quoted above, 27 patients with NBA > 0.007 proceeded to angiography of which 12 were found to have aneurysms. While there is documented evidence for the production of methaemoglobin following SAH, it was such an uncommon finding in the series quoted (in four patients, one of whom was angiography positive) that no clear indication of its significance could be obtained. Very recent work, which needs to be confirmed, has implicated high concentrations of iodine (widely used as a skin disinfectant) as being involved in in vitro methaemoglobin formation.
It is also commonly believed that xanthochromia will be evident in all patients up to two weeks following a bleed. Again this is based on an inappropriate group, those who were positive for blood on CT.
15
In patients who are negative for blood on CT who may be negative due to late presentation or small bleeds, we cannot be certain about this period of two weeks. In our experience, we have detected an increased CSF bilirubin in two patients subsequently shown to have ruptured aneurysms where the CSF was taken at 11 and 14 days after the onset of symptoms.
Footnotes
Acknowledgements
The Specialist Advisory Group acknowledge with thanks the assistance of D O'Connell, H Gunawardena and PLM Lynch in the provision of data which has been used by the group, and to D O'Connell for Figure 1. It also acknowledges the formulation of guidelines by other groups particularly the All Wales Audit Group and the Northern Ireland Audit Group, and the contributions of former members M Fahie-Wilson, PR Wenham, P Thomas and K Allen.