
Abstract
Abstract
Background
Protein S-100 is found in extracerebral sources. The aim of our study was to examine the content of protein S-100 in native pericardial fluid as well as in postoperative extracerebral fluids after cardiac surgery in children.
Methods
We conducted a prospective study in 90 children measuring protein S-100 concentration in pericardial fluid directly after opening the pericardial sac before starting with cardiac surgery. Postoperatively, we examined pleural, peritoneal and pericardial fluid.
Results
Pericardial fluid sampled directly after opening the pericardial sac has a protein S-100 content of 3.2 (1.3–5.4) μg/L. Postoperatively, protein S-100 content was 0.89 (0.56–2.6) μg/L in pleural effusion, 0.14 (0.1–1.1) μg/L in peritoneal fluid and 2.75 (2.2–24.4) μg/L in pericardial fluid. The protein S-100 concentration in pericardial fluid before and after cardiac operation did not differ significantly. Pericardial protein S-100 concentrations were significantly higher than pleural and peritoneal protein S-100 concentrations.
Conclusions
Protein S-100 is present in extracerebral fluids before and after cardiac surgery in children. The time point of fluid withdrawal after the operation did not influence the protein S-100 concentration.
Introduction
A simple biochemical test that could quantify neurological injury would be a major step forward in the evaluation of cerebral injuries after cardiac operations. Serum S-100 protein concentration has been proposed as a potential marker of cerebral injury after cardiac surgery. 1–3 Protein S-100 is a dimeric acidic calcium-binding protein constituting a major component of the cytosol of various cell types. Protein S-100B (ββ subunits) and S-100A (αβ subunits) are predominantly present in astrocytes and Schwann cells 4 and has a biological half-life of 25 min. 5 Recent study results differentiate between the early and the sustained increase in serum protein S-100 concentrations after cardiac surgery and their different significance in predicting neurological dysfunction. 6 Moreover, several studies suggest that extracerebral sources of protein S-100 may interfere with the interpretation of the serum S-100 concentration. 5–7
Only a few studies have examined the concentrations of protein S-100 in different extracerebral fluids after cardiac surgery 5,7,8 and data in children after cardiac surgery are lacking. There are no data concerning the protein S-100 content in native pericardial fluid or postoperative pericardial, pleural and peritoneal fluid after cardiac surgery, which was the reason for performing this study.
Methods
After institutional review board approval and informed consent from the parents were obtained, 90 children (45 boys, 45 girls; median age 26 months (7 days–12.6 years)) undergoing elective cardiac surgery for congenital heart disease with cardiopulmonary bypass (CPB) were entered into this study. Exclusion criteria were Down's syndrome, preoperative evidence of neurological injury and lacking parental consent. The study population was representative in age, gender and diagnosis of the overall patients operated on in our institution.
Samples were taken in 40 children directly after opening the pericardial sac by aspiration of pericardial fluid with a syringe before starting CPB. If the respiratory clinical situation was compromised due to pleural effusion, a single puncture of pleural fluid was performed (n = 24) at a mean of 4 (1–25) days after the operation. Peritoneal fluid (n = 13) was obtained postoperatively due to haemodynamically relevant ascites at a mean of 2.2 (1–14) days and pericardial fluid (n = 13) due to postpericardiotomy syndrome at a mean of 34 (23–76) days after cardiac surgery. Sample fluids were stored frozen at −20°C until analysis. We examined the content of protein S-100 in the different fluids and analysed its correlation to the date of withdrawal of the fluids.
A commercially available electrochemiluminescence immunoassay for protein S-100 running on an automated selective analyzer (Elecsys 2010, Roche Diagnostics, Mannheim, Germany), which measures both the S-100B (S-100ββ) and S-100A (S-100αβ), was used. As stated by the manufacturer, this assay has a direct measuring range of 0.005–39 μg/L and a functional sensitivity (at a run-to-run coefficient of variation [CV] of 20%) of 0.02 μg/L. Samples with values above the upper limit of 39 μg/L were remeasured with the sample manually diluted 1:5 in the S-100 zero calibrator.
To identify the nature of S-100 produced in the pericardium, we analysed the S-100α subunit and S-100β subunit protein concentration in the pericardial tissue using the Western blot technique.
After removal, pericardial tissue samples were homogenized with RIPA-lysis buffer and inhibitors and was incubated 10 min on ice. Protein concentration was determined using the BCA-Protein Assay Kit (Pierce Biotechnology, Rockford, USA). Equivalent amounts of protein (50 μg/slot) were loaded along with the prestained protein ladder (MIB-Fermentas, St. Leon-Roth, Germany) on to 15% sodium dodecyl sulfate polyacrylamide gel electrophoresis. Immunoblotting was performed using the tank blotting transfer method (Biorad, Carlifornia, USA). Immunodetection processing was done with the following primary antibodies: monoclonal S-100α (Biozol, Eching, Germany) and S-100β (Biozol, Eching, Germany). As secondary antibody peroxidase conjugated anti-rabbit IgG (Jackson Laboratory, Maine, USA) was used. Proteins were visualized using enhanced chemoluminescence technology according to the manufacturer's instructions (Pierce Biotechnology). Hydridization with the house-keeping protein β-actin (Sigma-Aldrich, Deisenhofen, Germany) was used to ensure equal loading and protein quality.
Neurological examination was performed each day after cardiac operation until discharge; cranial ultrasound was performed within 24 h after cardiac surgery and if neurological sequelae were present.
Data were expressed as medians and interquartile ranges. Group comparisons were performed with the Mann-Whitney U test. Correlations were tested with the Pearson correlation test.
All calculations and tests were performed by means of SPSS for Windows 7.0 (SPSS Inc., Chicago, IL, USA). A P value < 0.05 was considered to be significant.
Results
The demographic data of the patients are given in Table 1. Eighty-six patients had an operation with CPB, four patients had a shunt without CPB. No patient suffered from neurological disabilities after the operation and all cranial ultrasounds (n = 55) were without pathological findings.
Clinical data and congenital heart defects (n = 52) in 43 children leading to surgical repair
Native pericardial fluid sampled directly after opening the pericardial sac had a protein S-100 content of 3.2 (1.3–5.4) mg/L. Measurement of protein S-100 in postoperative pericardial fluid showed 2.75 (2.2–24.4) mg/L. The protein S-100 concentration in pericardial fluid before and after cardiac operation did not differ significantly (P = 0.395).
In Western blot analyses of pericardial tissue, we distinguished a significantly higher S-100β subunit concentration in comparison with the measured S-100α subunit (Figure 1).
Postoperative pleural fluid had a protein S-100 content of 0.89 (0.56–2.6) mg/L, and peritoneal fluid contained 0.14 (0.1–1.1) mg/L. Native and postoperative pericardial protein S-100 concentrations were significantly higher than pleural and peritoneal protein S-100 concentrations (P < 0.001 and P = 0.024 versus P < 0.001 and P = 0.002, respectively). Figure 2 shows the different concentrations of extracerebral protein S-100 concentrations before and after cardiac surgery in our study population.
There was no correlation between the number of days postoperatively the fluid was tested and the concentration of S-100 protein in pericardial, pleural or peritoneal fluid.
Discussion
The significance of serum S-100 as a predictor of cerebral brain damage after cardiac surgery is not sufficiently clarified. 3,9,10–12 It has been postulated that serum S-100 protein is usually released after cerebral damage, but serum S-100 found immediately after CPB may not originate only from the brain. 5,7 Mediastinal fat (median 108 μg/g), skeletal muscle (median 20 μg/g) and sternal bone marrow aspirate (median 29 μg/g) contain very high concentrations of S-100. 7 Anderson et al. 8 demonstrated that blood aspirated from the midline incision before sternotomy contains 200 times more S-100 than preoperative serum. 8 In our samples of the so-called ‘native’ pericardial effusion, we postulate no contamination by mediastinal blood because the pericardial fluid was withdrawn directly after opening the pericardial sac by a small surgical incision without any contact with any other tissues. Thus, our results give evidence that protein S-100 is also present in native pericardial fluid.
Furthermore, we can postulate that the subunit S-100 B is produced in the pericardial tissue as demonstrated by the Western blot analysis. We assume the concentrations of protein S-100 measured in native pericardial fluid in the present study to be ‘normal’ values, which originate from the pericardium itself.
From the statistical point of view, there was no significant difference between the preoperative and postoperative concentrations of S-100 in the pericardial fluid, but the range of the results obtained in the postoperative group is substantially higher than that in the preoperative group, as demonstrated in Figure 1. Some of the S-100 concentrations seen postoperatively in the pericardial fluid are of the same order of magnitude as those found in the cerebrospinal fluid of patients with either subarachnoidal haemorrhage or traumatic brain injury (26.11 ± 3.73 μg/L) using the same analytical system. 13 This implies that the high postoperative S-100 concentrations reached in pericardial fluid represent a significant pathological span.
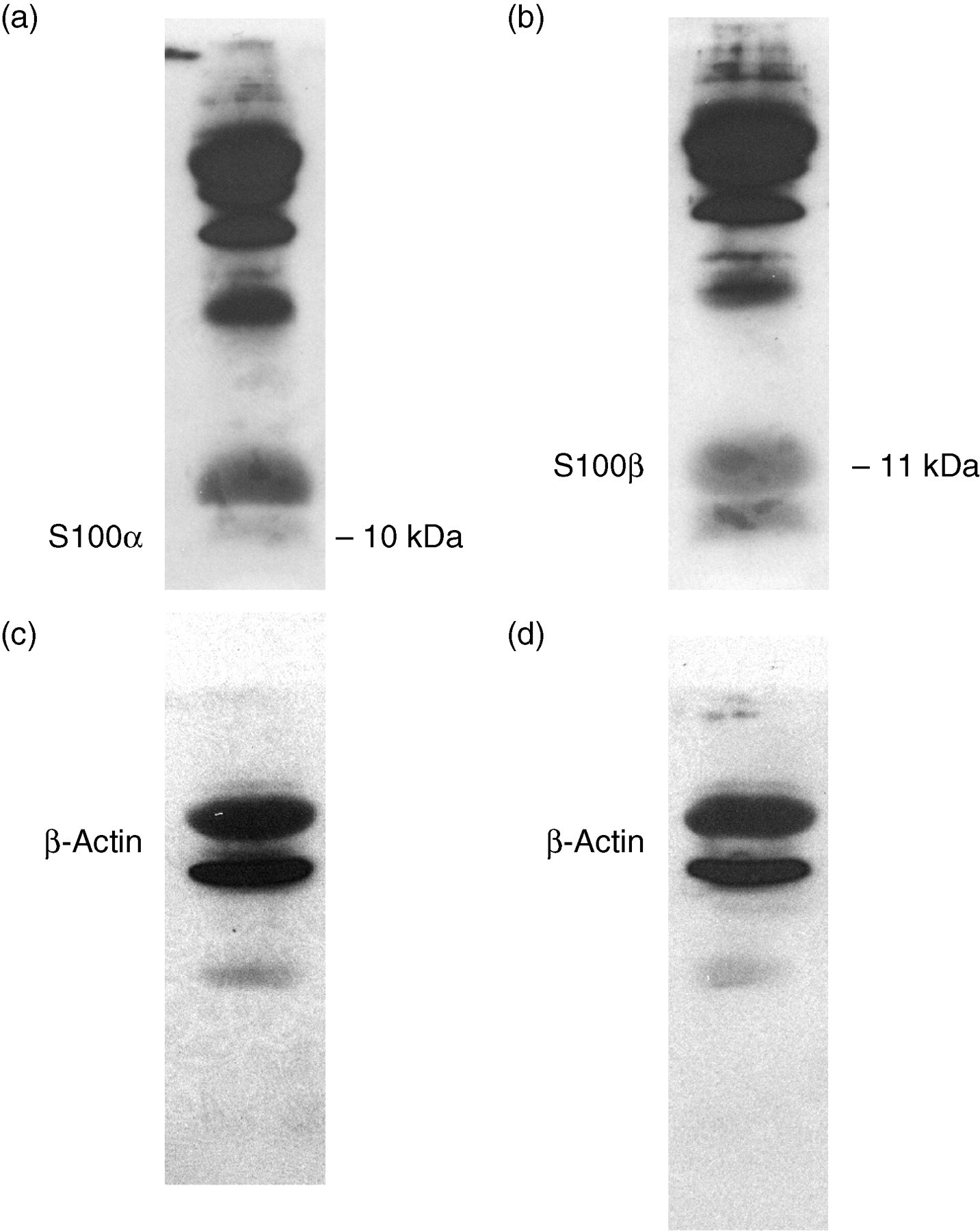
(a) Protein concentrations of S-100α subunit, (b) protein concentration of S-100β subunit (c) and (d) β actin in pericardial tissue as equal loading control to (a) and (b)
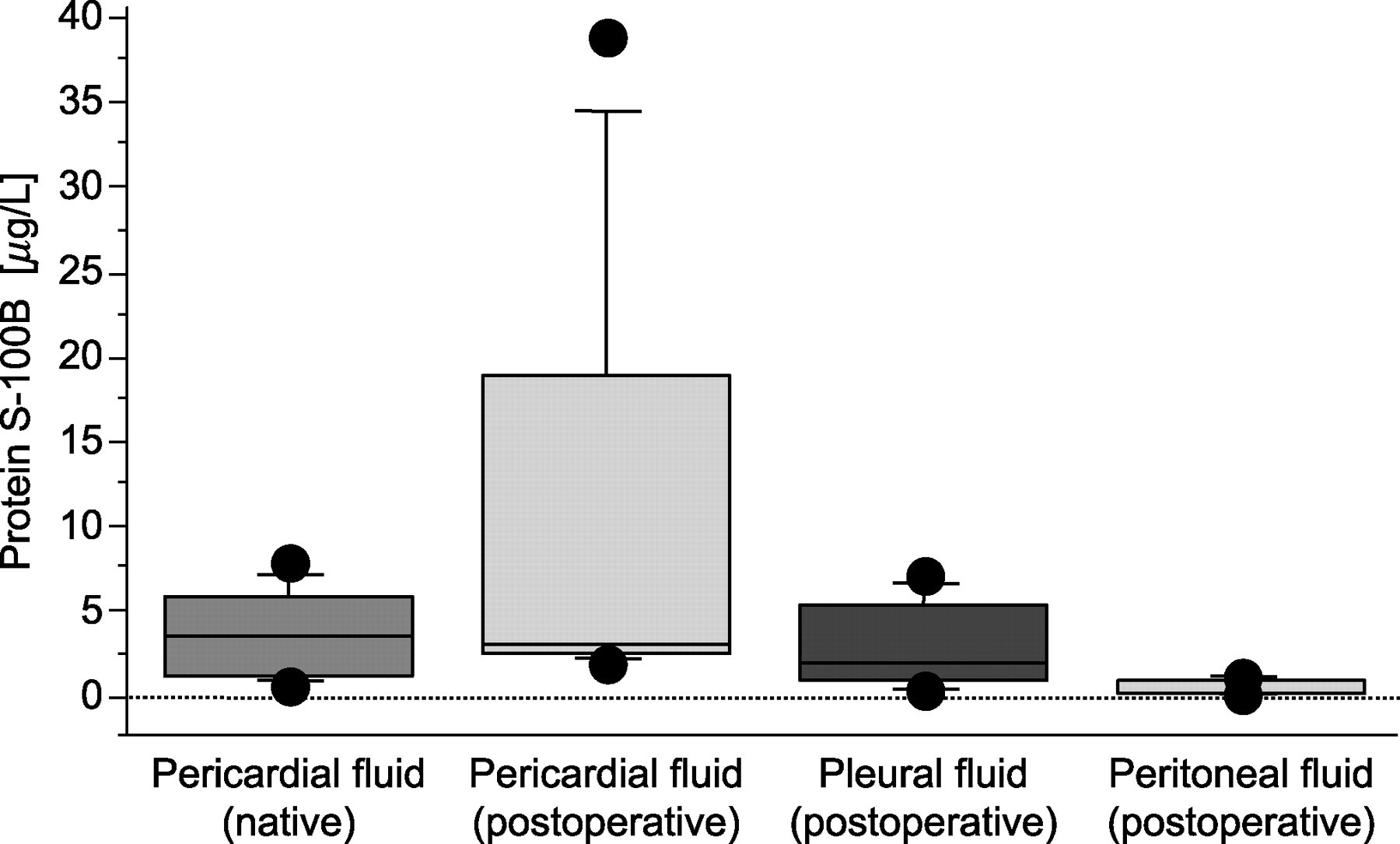
Concentrations of protein S-100 B in extracerebral fluids before and after cardiac surgery in children
Concentrating on the four patients with protein S-100 concentrations of more than 10 μg/L, we could not detect poorer postoperative recovery, longer hospitalization, different severity of postpericardiotomy syndrome or any other features that make them unique. Like the other nine patients in this group, they developed postpericardiotomy syndrome after the initial uneventful cardiac operation.
We cannot compare directly our results for protein S-100 in postoperative pleural and pericardial fluid to the data from former studies, where protein S-100 was examined in the chest-drain reservoir directly and 1, 2, 3, 6 and 20 h after the end of the operation 7 or from the cardiotomy reservoir. 5 Concentrations in blood from the chest drain increased more than fourfold during the 6 h after the operation and reached values of more than 200 μg/L7 as did mediastinal blood shed from the cardiotomy reservoir with a mean concentration of protein of 70 μg/L. 5 We postulate that the chest-drain reservoir fluid incorporates mainly fluid from the operation field. We, however, sampled postoperative pericardial fluid on postoperative day 23–76, much later than in the former study. Therefore, we measured much lower concentrations of S-100, which can be explained by the short biological half-life of protein S-100 ß of approximately 30 min. 5
The concentration of protein S-100 in the postoperative peritoneal fluid is very low compared with those measured in preoperative serum of infants. 14 It seems unlikely that the measured concentrations of protein S-100 in peritoneal fluid are contaminated by the puncture through the abdominal wall. Anderson et al. 7 suggested a shift of intrathoracic protein S-100 to the peritoneum due to a concentration gradient from thorax to abdomen in the early postoperative period. However, taking into account that there is no correlation with the postoperative time (i.e. there is no tendency for concentrations to decrease within days) it is very likely that this is a baseline concentration in peritoneal fluid, as in the unaffected pericardial fluid.
Unfortunately, we did not examine the serum protein S-100 concentrations in our study population to compare it directly with the protein S-100 values in native pericardial and other postoperative fluids. Therefore we compared our results with that in studies where serum protein S-100 concentrations were measured in a comparable patient population of neonates and children. Serum protein S-100 concentrations were approximately in a range of 0.7–1.4 μg/L. 14,15
The so-called native protein S-100 concentrations in pericardial fluid seem to be higher than the preoperative concentrations in neonates and infants. Possibly, there might be a cell turnover of epithelial cells of the pericardium which leads to a release of protein S-100 into the pericardial fluid.
In conclusion, protein S-100 is found postoperatively in pleural, pericardial and peritoneal effusions, but also preoperatively in the native pericardial fluid. In native pericardial fluid it can be detected in concentrations of 3.2 (1.3–5.4) μg/L.
Footnotes
Acknowledgement
The authors thank Anne Gale, Editor in the Life Sciences, for editorial assistance.