
Abstract
Intermittent failure of two endocrine systems is unusual and presents diagnostic and management challenges. We report a case of a young woman with intermittent thyroid and ovarian failure who had spontaneous twin gestation four years after the diagnosis of premature ovarian failure was made. This case demonstrates coincidental biochemical and clinical thyroid and ovarian failure both of which spontaneously resolved with no treatment, although subsequently irreversible hypothyroidism ensued after the initial recovery. Elevated gonadotrophins with a menopausal pattern on more than one occasion, in an amenorrhoeic patient with menopausal symptoms, usually indicates permanent ovarian failure. This case demonstrates that this may not be true and while this is probably a rare occurrence, clinicians need to be aware of this possibility. It also re-emphasizes the need to consider the clinical picture when interpreting biochemical results.
Introduction
Premature ovarian failure (POF) is characterized by the occurrence of amenorrhea, raised gonadotrophins and oestrogen deficiency in women under the age of 40 years. 1 The prevalence is estimated to be between 0.9 and 1.2%. 2 Spontaneous pregnancy in patients with POF, although previously reported, remains quite rare. We report a case of a young woman with intermittent thyroid and ovarian failure who had spontaneous twin gestation four years after the diagnosis of POF was made. This case demonstrated coincidental biochemical and clinical thyroid and ovarian failure both of which spontaneously resolved with no treatment, although subsequently irreversible hypothyroidism ensued after the initial recovery.
Case report
A 27-year-old woman was initially referred to the metabolic and endocrine clinic for medical management of renal stones. She had spontaneously passed a stone in her urine, which was composed of calcium oxalate. Subsequent urogram was normal. No biochemical abnormality was found in her blood or 24-h urine sample and the patient was discharged.
She was referred again eight months later with complaints of gradually worsening hot flushes, mood swings and slight increase in weight. She had missed one period. She had menarche at the age of 12 years, and her periods had been regular (5/28). She had an identical twin sister who was in good health. She was a known asthmatic. She was a non-smoker and drank alcohol rarely. She was not on any regular medication. There was no family history of ovarian or thyroid problem, although interestingly her mother had her menopause in her early forties.
On examination, she weighed 76 kg, and her body mass index (BMI) was 30.6 kg/m2. There were no other significant findings on examination. Biochemical investigations revealed high luteinizing hormone (LH) and follicle-stimulating hormone (FSH) of 20.2 and 44 IU/L, respectively and low oestradiol concentrations of less than 150 pmol/L consistent with primary POF. Her other results were as follows: thyroid-stimulating hormone (TSH) 1.26 mU/L, testosterone 1.4 nmol/L, dehydroepiandrosterone sulphate (DHEAS) 6.2 µmol/L, sex hormone binding globulin (SHBG) 17 nmol/L, free androgen index (FAI) 8.2%.
Repeat tests performed one month later showed similar results. A diagnosis of POF was made based on clinical presentation and laboratory findings. However, she resumed normal menstruation after two months and her gonadotrophins and oestradiol returned to premenopausal levels.
Two years later, she presented again with similar complaints and increasing tiredness. She also had dry skin and hair on this occasion. Her LH, FSH and oestradiol were 21 IU/L, 40 IU/L and 66 pmol/L, respectively. Fasting glucose was 4.9 mmol/L, and she had no signs or symptoms suggestive of diabetes mellitus. Liver function tests and urea and electrolytes were within the reference range. Her TSH was 107.7 mU/L. Before thyroid replacement was started, her TSH had fallen to 20.9 mU/L and eventually normalized without treatment.
Over the following year, there were wide fluctuations in her thyroid hormone status as well as the concentrations of gonadotrophins (Figure 1). Whenever possible gonadotrophin measurements were taken during the follicular phase. Thyroxine therapy was instigated after the TSH increased to 45.3 mU/L and she had clinical symptoms of hypothyroidism. Similarly, her LH, FSH and oestradiol varied from normal premenopausal levels to postmenopausal levels (Figure 1). An autoimmune condition causing intermittent thyroid and ovarian failure was suspected. Her immunology results were interesting in that her thyroid peroxidase antibodies were negative but she had weak positive ovarian antibodies. Repeat ovarian antibody screen was however negative. To investigate the possibility of multiendocrine involvement, a short Synacthen test was performed to check the adrenal reserve. Serum cortisol value at 0 and 30 min after 250 µg of intravenous Synacthen were 702 and 788 nmol/L, respectively. Even though an increment of 200 nmol/L was not observed at 30 min, the 30-min cortisol was well above the standard cut off of 550 nmol/L used in this test, and the baseline serum cortisol of 702 nmol/L made hypoadrenalism unlikely. She was stabilized on thyroxine 125 µg daily.
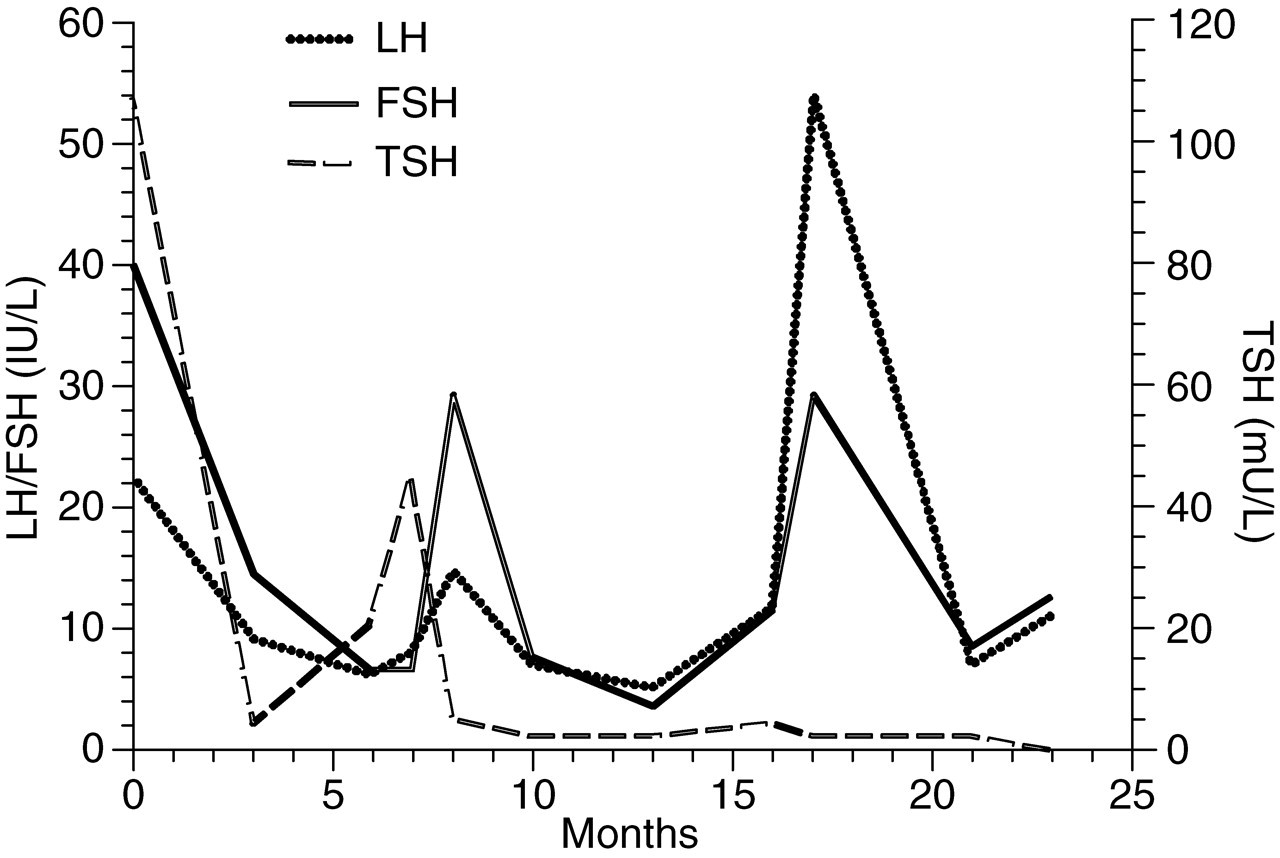
Graph showing variation of TSH (thyroid-stimulating hormone) and gonadotrophins with time. Peak results indicate end organ failure, with complete biochemical resolution between peaks. LH, luteinizing hormone; FSH, follicle-stimulating hormone
A full screen was also requested on her identical twin sister. The results were all normal; LH was 5.5 IU/L, FSH was 3.0 IU/L, serum day 21 progesterone was 45 nmol/L and TSH was 3.1 IU/L.
In view of her ovarian dysfunction, the patient was advised to start a family sooner rather than later. Hormone replacement therapy was considered and she was subsequently referred to the infertility clinic. Day 21 progesterone concentrations done on two occasions were inconclusive (13 and 21 nmol/L). However, before any treatment could be initiated, she conceived spontaneously. Her pregnancy was uneventful and she delivered healthy twins: a boy and a girl.
The patient has normal ovarian function at the time of reporting this case. She continues to take thyroxine for her hypothyroidism.
Discussion
Most reported pregnancies in patients with POF occur while patients are receiving active treatment. 3–8 Overall, POF patients have 5–10% chance of conceiving at some time after diagnosis and treatment. 9,10 There are no adequate tools available for categorizing the majority of POF patients according to aetiological factors, the presence of oocytes, or the potential to achieve a pregnancy. It is noteworthy that our patient conceived spontaneously without any treatment. It is also possible that our patient had some form of follicular dysfunction rather than complete ovarian failure. However, the gonadotrophins might not be expected to be so elevated with the typical menopausal pattern if this were the case. In a recent update, Nelson et al. stressed that ovarian failure in this disorder is not permanent in all patients and that POF is not the same as premature menopause. 10 It is important that menopause should not be diagnosed unless periods have been absent for twelve months. The course of pregnancy in patients with POF appears to be normal.
Autoimmunity has been postulated as one of the aetiological factors in pathogenesis of POF. 11,12 Association of autoimmune hypothyroidism, Addison's disease, vitiligo and POF has been documented. 4,13,14 There has been one case report describing transient symptomatic POF and primary hypothyroidism. 15 The authors reported initial peaks of FSH and TSH at presentation, which gradually fell over a period of six months and returned within the reference range; however, the condition was not intermittent. In contrast to this, the concentrations of gonadotrophins returned to normal and then peaked again into the menopausal range in the case presented here. A similar intermittent pattern was also observed for TSH. The intermittent nature of her condition may have been secondary to an autoimmune process with the waxing and waning nature of antibodies. In the case described here, hypoadrenalism was excluded by the short Synacthen test. However, an autoimmune aetiology could not be excluded on the basis of negative thyroid and ovarian antibody screen. The search for antiovarian antibodies undertaken by several authors in POF has yielded somewhat conflicting results, probably due to methodological differences and by the multiplicity of potential immune targets. 16 The rise in TSH seen on two occasions seems to coincide with elevations of FSH into the menopausal range. This might suggest a common aetiology, but in the absence of any further TSH peaks, this can only be speculative.
POF may be associated with other endocrinopathies. 17 This patient was screened for diabetes mellitus and Addison's disease with negative results. It is possible that the patient had components of one of the autoimmune polyglandular disorders. Autoimmune polyglandular syndromes are characterized by multiple endocrine insufficiencies. They are broadly classified into four distinct types. 18,19 Type 1 is rare and presents in childhood. It usually is comprised of mucocutaneous candidiasis, hypoparathyroidism and primary adrenal insufficiency. Type 2 is the most common form and occurs mostly in women. It is characterized by obligatory occurrence of Addison's disease in combination with autoimmune hypothyroidism and/or type 1 diabetes mellitus. Myasthenia gravis, coeliac disease, vitiligo, chronic atrophic gastritis and primary hypogonadism may also be observed in these patients. Type 3 is the co-occurrence of thyroid autoimmune disease with other autoimmune disorders including type 1 diabetes mellitus, pernicious anaemia or a non-endocrine autoimmune disorder but in the absence of Addison's disease. Type 4 is the combination of organ specific autoimmune diseases not included in the previous group. It may be that our patient had components of autoimmune polyglandular syndrome type 2 or 3. However, in absence of type 1 diabetes mellitus, Addison's disease and any other non-endocrine autoimmune disease, she does not strictly fit into any of the above-mentioned types. It is rare for patients to have a complete syndrome from the outset, but may have the simultaneous presentation two or more major endocrinopathies. After a variable latent period, they may develop other components of the syndrome. It is therefore important to screen these patients every two or three years to identify those at risk of future development of the fully expressed syndrome. 18
The intermittent nature of her problems posed difficulties in diagnosis as well as in management. The emotional and psychological issues associated with POF need to be addressed in these patients. 20 In this case, these issues were complicated by the intermittent nature of the condition and the fact that the patient had indicated a desire to postpone any pregnancies for some years. It was suspected that the ovaries could fail and not recover in the same way that the thyroid did, and so she was advised against this postponement. Oestrogen replacement was considered, but she resumed normal periods and her menopausal symptoms resolved before this was instigated.
It is also interesting to note that the ovarian function was completely normal in the identical twin. This discordance in POF among monozygous twins has recently been studied in detail by Gosden et al. 21 They found some striking differences in POF including age of onset, within monozygous twin-pairs. Earlier, the same group had reported successful ovarian tissue transplantation from unaffected twin sister which resulted in normal pregnancy after a natural conception. 22 Thus, if the ovarian function in these patients does not return, ovarian transplant may be considered as a treatment option, if they have an unaffected identical twin. It may have been an option in this case, but this became unnecessary when she conceived without assistance.
The mechanism of current remission in this patient is unknown. We speculate that the hormonal as well as autoimmune changes related to pregnancy and the post-partum period might have had a role. Patel et al. 14 have described a patient with POF who after a pregnancy achieved a prolonged remission which had lasted 10 years. They also reported spontaneous remission of hypothyroidism and vitiligo in the same patient.
In summary, we report a case made unusual by the combination of intermittent failure of two endocrine systems. Transient hypothyroidism is not unknown, although it is unusual for very high TSH values–as seen in this case–to spontaneously resolve. Our case highlights the diagnostic and management challenges in such patients. Gonadotrophins showing a menopausal pattern in amenorrhoeic women with menopausal symptoms usually indicate primary ovarian failure that is generally considered to be irreversible. This case suggests that reversibility can occur. This case re-emphasizes the fact that although rare, spontaneous pregnancy is a possibility in patients of POF. It also re-emphasizes the need to consider the clinical picture when interpreting biochemical results.