
Abstract
Abstract
Background
Most medical school curricula have reduced the amount of time available for teaching in pathology despite the fact that junior staff in the early stages of their training were responsible for requesting the majority of pathology tests on acutely ill hospital patients. So, the lack of specific training in this area means that test requesting may be poorly performed and the results ill understood by these staff. This paper describes a questionnaire, which was designed to assist laboratory staff providing targeted teaching in this area.
Methods
Doctors in Foundation year 1 (F1) and Foundation year 2 (F2) in Sheffield teaching hospitals were given a questionnaire to ascertain how confident they were in requesting and interpreting the results of clinical biochemistry tests. The doctors were also asked about which areas of laboratory medicine they would like to be taught.
Results
Responses were received from 82 doctors, about half those in F1 and F2. The survey revealed areas where juniors are less confident in requesting tests and interpreting results. Despite lack of confidence in interpreting the result, 18% were confident about requesting tests. Doctors were also unsure of the effects of common problems like haemolysis on the interpretation of results. More than 70% of the doctors requested specific teaching in these areas.
Conclusions
Foundation doctors have learning needs in clinical biochemistry, addressing which would assist them in patient care. While better training in medical school may help in future, there are specific needs for those on the wards now that require targeted teaching.
Introduction
Junior doctors have significant responsibility in the early years of their training for requesting tests and interpreting the results on the patients for whom they are responsible. However, as the teaching of clinical biochemistry becomes ever more limited in the curriculum, there is considerable concern among laboratory staff as to whether doctors receive sufficient training in basic science and the optimal use of laboratory investigations. In 2003, the General Medical Council (GMC) published ‘Tomorrow's Doctors’
1
which made three main education points addressing these issues:
Basic knowledge: ‘Graduates must have a knowledge and understanding of the clinical and basic sciences … (including) … normal and abnormal structure and function, … responses to illness and the response to treatment.’ Skills: ‘Graduates must be able to do the following safely and effectively: interpret the results of commonly used investigations … (and) make clinical decisions based on the evidence they have gathered.’ Teaching: ‘The clinical and basic sciences should be taught in an integrated way throughout the curriculum.’
The literature is sparse about whether these recommendations are being implemented. Most studies of requesting by doctors predate ‘Tomorrow's Doctors’ or have been carried out in countries other than Britain. However, it is reasonable to assume that the above points have always been desirable in any medical education. In 1982, Smith et al.
2
found that if tests were requested by senior clinicians, the request rate fell by 13%, suggesting that some of the tests being ordered by junior staff were unnecessary. A more recent study by Smellie et al.
3
found that 25% of all emergency requests were inappropriate. A study done in Australia in 19934 looked at patterns of unnecessary test requesting, one of which was ordering tests too frequently. All of the above studies mention that it is the junior staff that generated most of requests and therefore beg the question as to whether they are being appropriately taught to make the best use of laboratory services.
There is some evidence that the use of laboratory services can be improved by educating clinicians. Bareford and Hayling 5 showed that there was a definite and sustained reduction in inappropriate requests when certain measures such as issuing guidelines, fact sheets and holding seminars on clinical biochemistry were implemented. In a study done in 2000, 6 98% of doctors and medical students agreed that clinicians should be invited to seminars to improve their skills in interpreting laboratory investigations. When asked about the best method of delivering teaching on the subject, 93% preferred seminars with active participation to lectures or symposia.
This survey was born out of the frustrations of laboratory staff who found considerable gaps in the knowledge of junior staff when discussing significant results with them. Most of these junior doctors would have trained in Sheffield at a time when there was no specialist clinical biochemistry input to medical student teaching at all. At this Trust, junior staff get a teaching session once a week; so, the aim of this study was to investigate what foundation doctors already know and what they want to be taught about clinical biochemistry with a view to initiating appropriate teaching in order to improve the use of laboratory tests. Although intended as a local survey to inform local teaching practice, when the results were received it was felt to be of sufficient interest to bring to wider attention.
Participants and methods
A structured questionnaire (see appendix) was sent to Foundation year 1 (F1) and Foundation year 2 (F2) doctors working at the Sheffield Teaching Hospitals Trust between September and November 2006. The questions explored how confident these trainee doctors felt in requesting and interpreting biochemical tests. The doctors were also asked which particular topics in clinical biochemistry they would like to be taught about and at what stage in their medical training such teaching would be most useful. They were also asked for their preferred teaching method.
The questionnaires were emailed to all F1 and F2 doctors in the Trust but due to a poor response they were also handed out personally by VK at teaching sessions. Care was taken not to include any duplicates.
Results
Eighty-two questionnaires were returned. Fifty by F1 doctors (56% of total employed) and 32 by F2 doctors (41% of total employed). Twenty questionnaires were not filled completely: 11 had Q2 not filled out completely, 10 had Q6 and Q7 not filled completely. However, all the data collected were used in the analysis.
Figures 1 and 2 show how confident junior doctors feel in requesting and interpreting results, respectively. Many junior doctors do not feel confident requesting or interpreting magnesium (Mg) and phosphate (PO4), parathyroid hormone (PTH), short synacthen tests, and urine sodium and osmolality. Liver function tests, proteins and haematinics are tests that most junior doctors feel confident requesting, but less confident in interpreting. Only a minority of people feel confident interpreting haemolysed sample results. The data also show that 18% of doctors are ‘very confident’ in requesting tests they are ‘not confident’ in interpreting. Figure 3 show the results for the question ‘are you confident in interpreting haemolysed samples’ with only one-third replying ‘yes’. There was little difference in confidence between F1 and F2 doctors, the only significant finding being that F2 doctors were more confident in interpreting urea and electrolytes (U&E) and requesting Troponin I (Trop I).
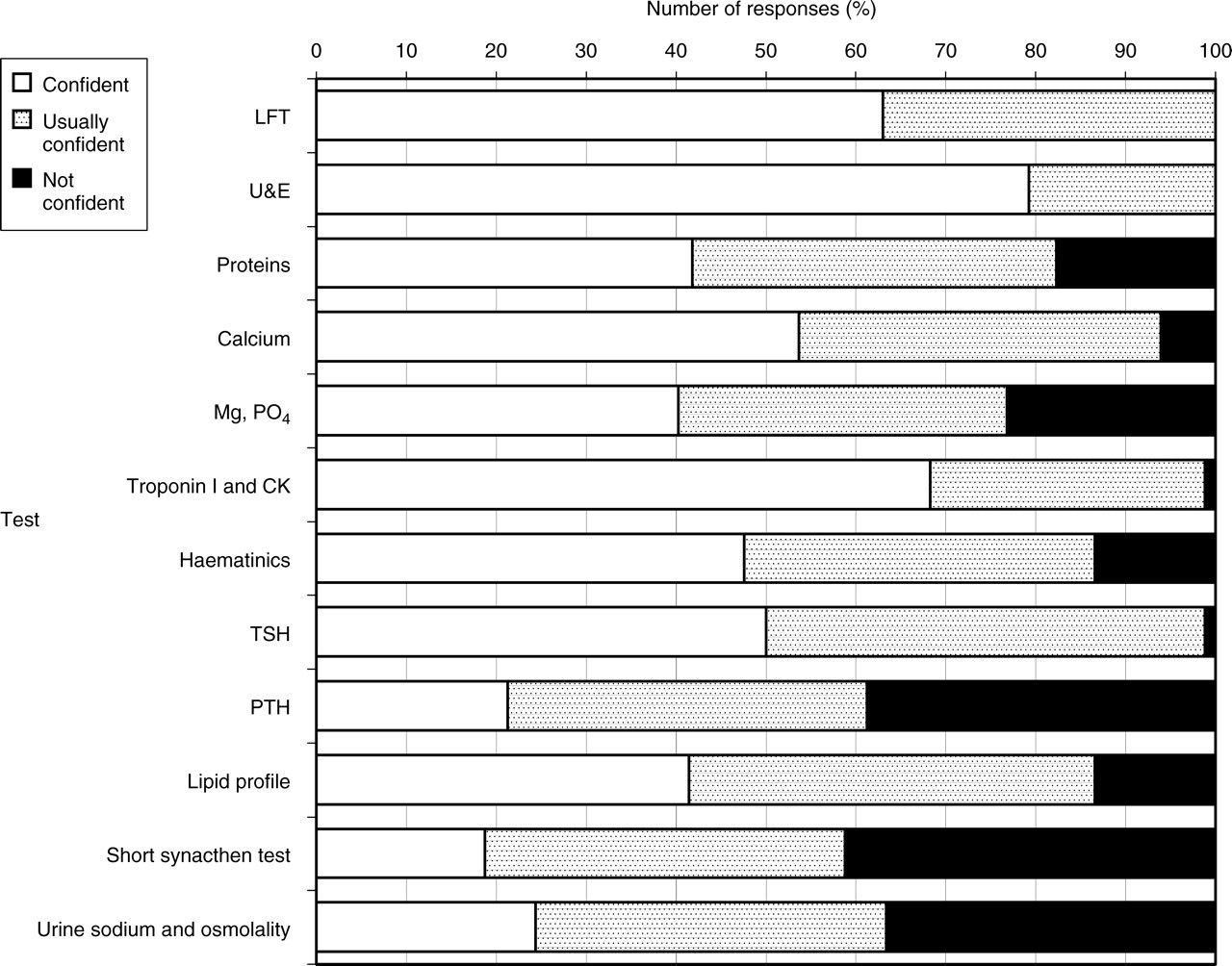
Confidence in requesting tests. The percentage of respondents who were confident, usually confident, or not confident about requesting tests. CK, creatine kinase; LFT, liver function tests; Mg, magnesium; PO4, phosphate; PTH, parathyroid hormone; TSH, thyroid-stimulating hormone; U&E, urea and electrolytes
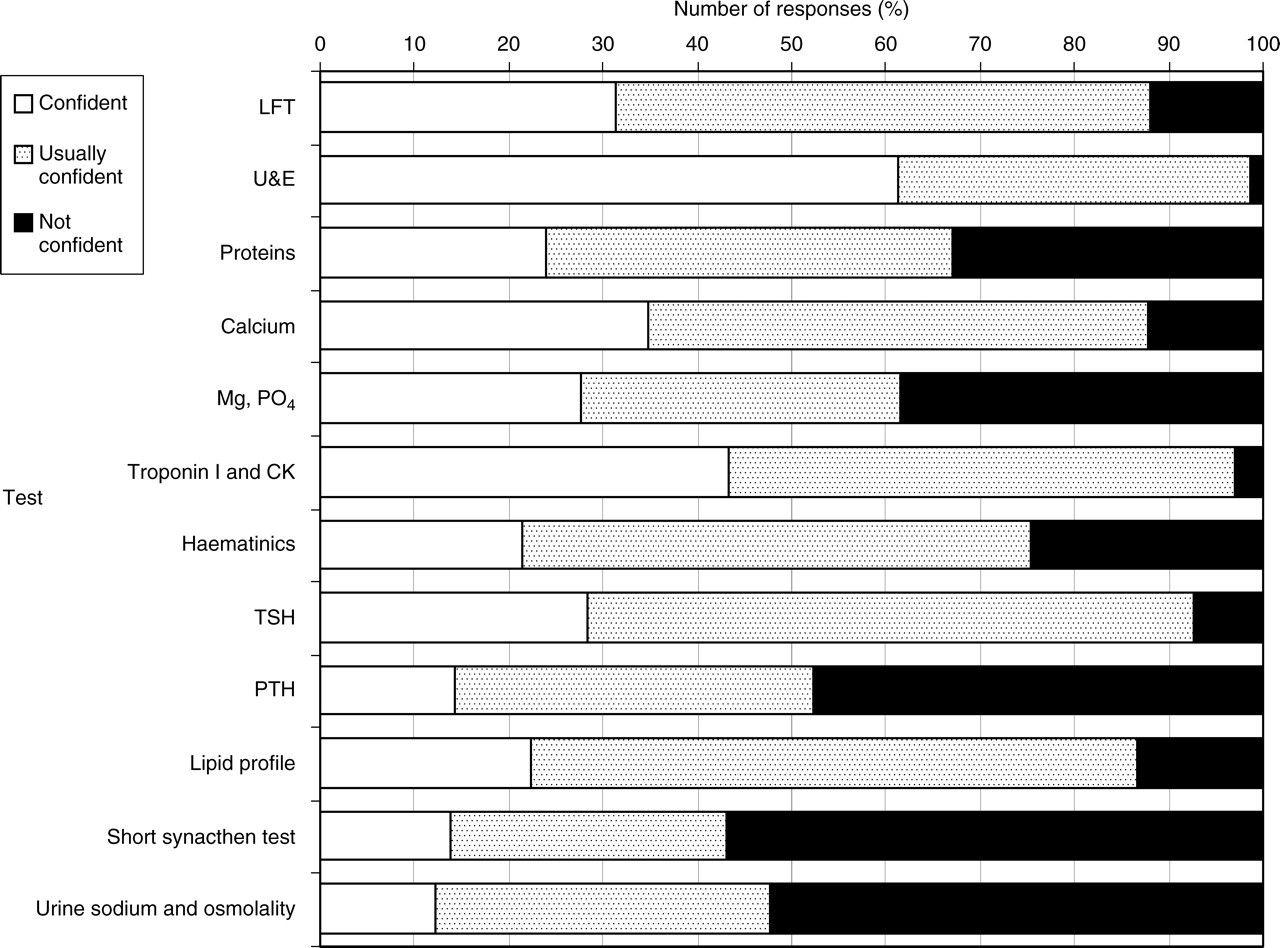
Confidence in interpreting results. The percentage of respondents who were confident, usually confident or not confident about interpreting results. CK, creatine kinase; LFT, liver function tests; Mg, magnesium; PO4, phosphate; PTH, parathyroid hormone; TSH, thyroid-stimulating hormone; U&E, urea and electrolytes
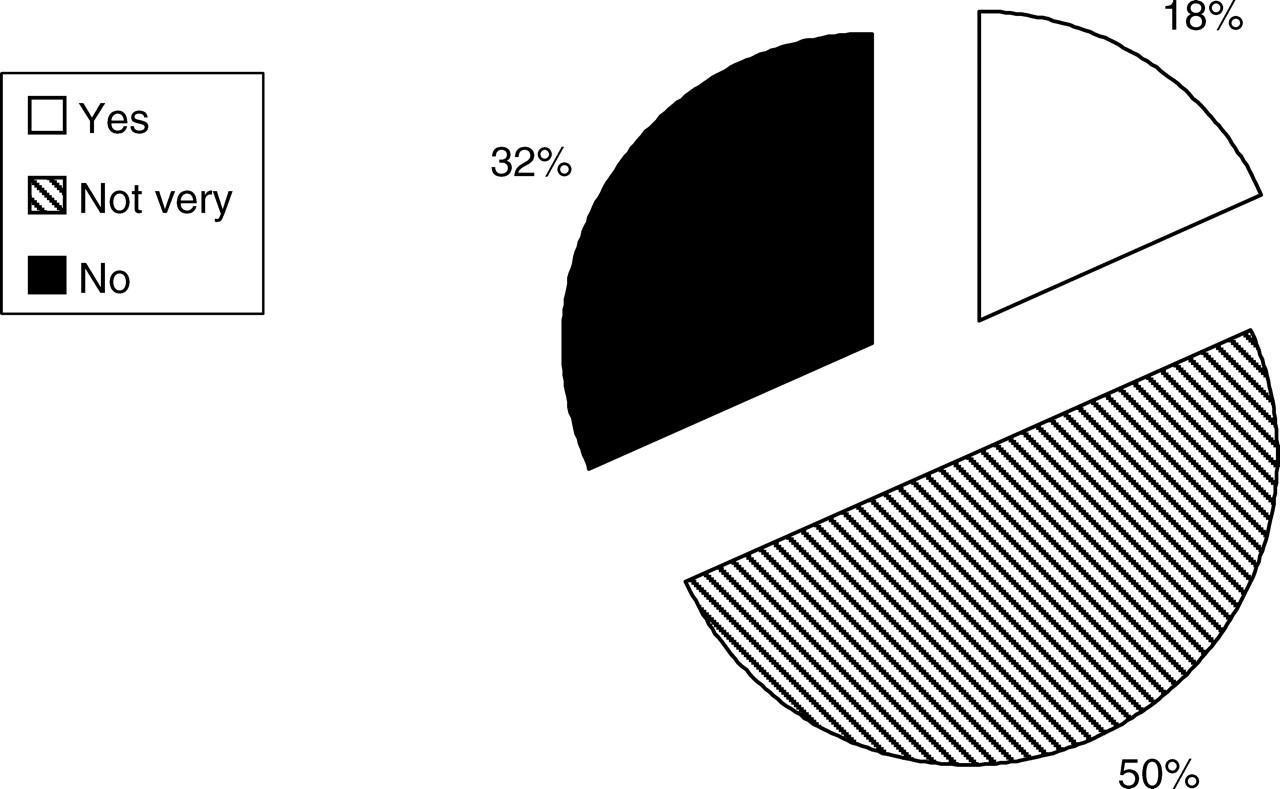
Confidence in interpreting haemolysed samples. The percentage of respondents who were confident, not very or not confident about interpreting results in haemolysed samples
Figure 4 shows the subjects on which junior doctors requested teaching, with short synacthen tests, urine sodium and osmolality, and haemolysed samples being the most frequently requested. In the free text at the end, some also requested teaching on the following topics: coagulation tests, estimated glomerular filtration rate (eGFR), sex hormones, relating clinical picture to results, trends in results in different conditions, groups of tests for certain clinical situations, and correction of electrolytes especially Mg and PO4.
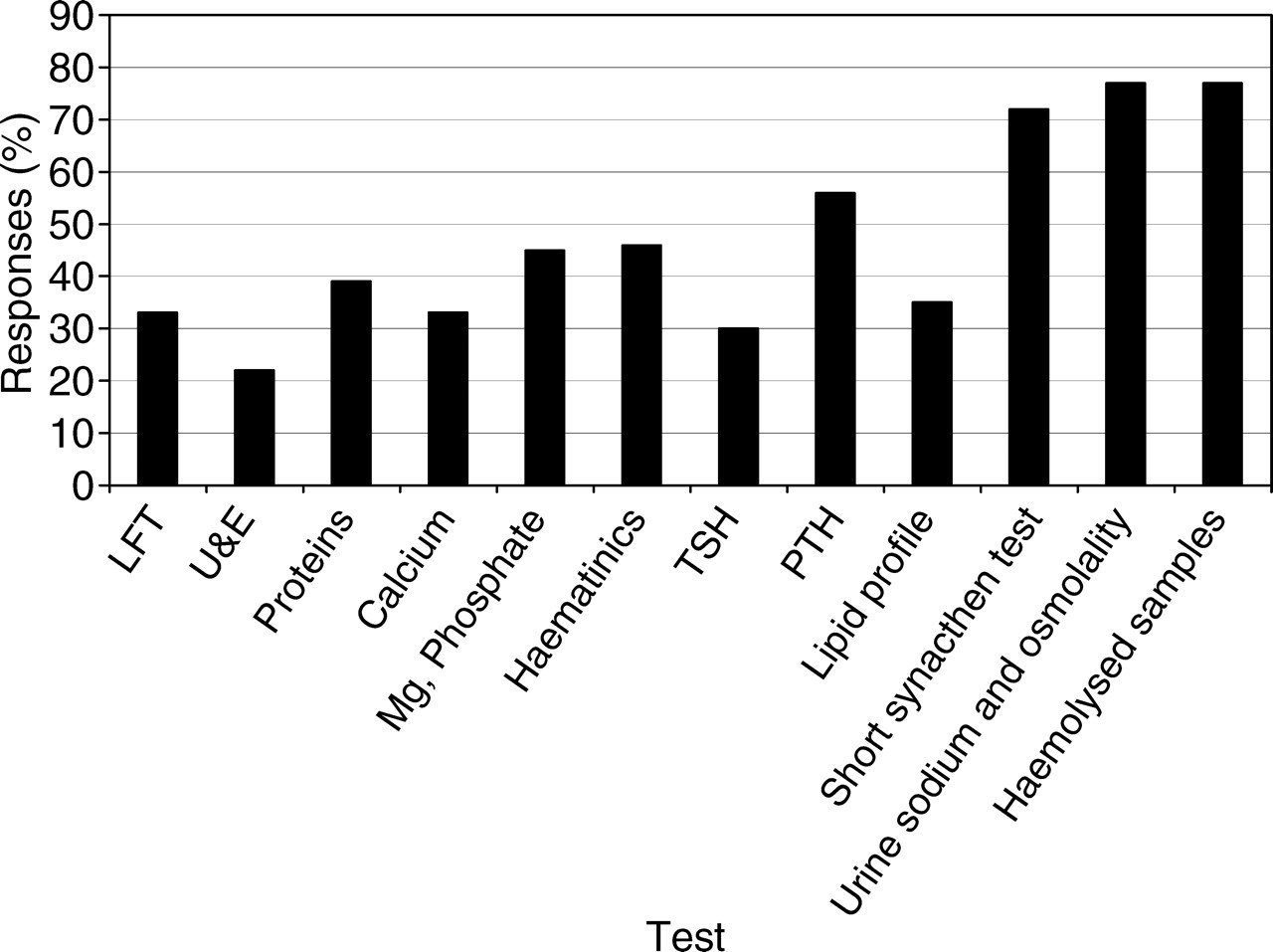
Subjects on which doctors would like further teaching. See Figure 2 for abbreviations
Figure 5 shows the preferred time of teaching, the alternatives being the last year of medical school, or during F1 or F2. Over 95% agree that this should be done either in the final year of medical school, or in F1 or both, with F1 being the most popular choice by a narrow margin. Figure 6 shows the preferred teaching methods. The preferred teaching method is a small group seminar, with lectures being a close second. However, many people expressed verbally that an online tutorial would be a useful adjunct and over one-third of respondents felt that they were very likely to complete such a tutorial.
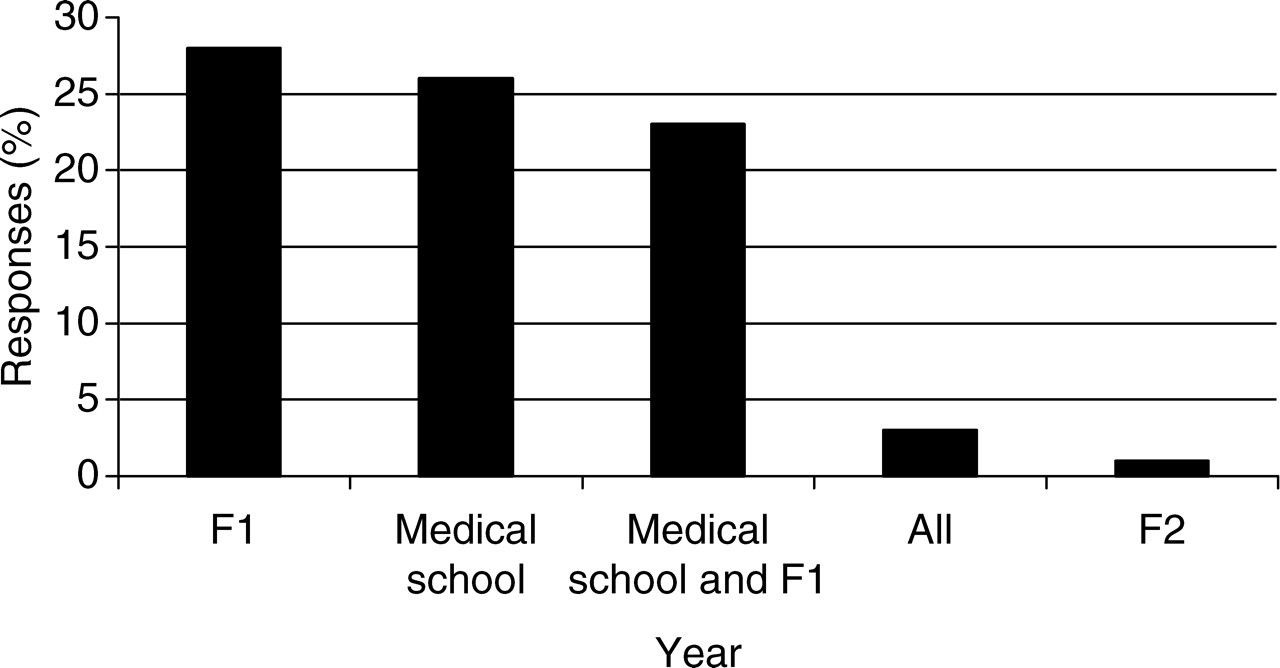
Preferred time for further teaching. F1, Foundation year 1; F2, Foundation year 2
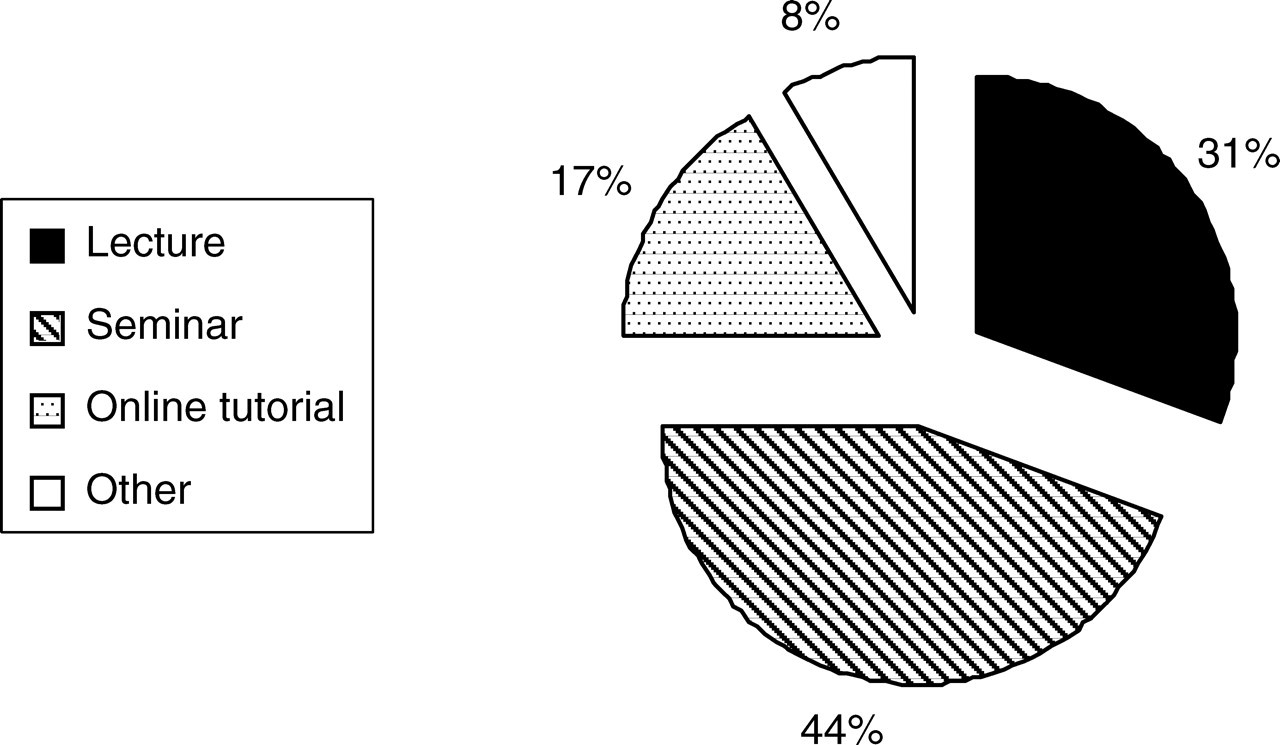
Preferred method of teaching. Other refers to a combination of the teaching methods listed
Discussion
This survey confirmed that foundation doctors have gaps in their knowledge of when to request and how to interpret laboratory tests. The doctors themselves were usually aware of these lacunae in their knowledge and expressed a wish for additional teaching in clinical biochemistry.
The survey was designed as a pragmatic tool to answer a local question and therefore it did have some limitations. First, only about half the doctors responded to the questionnaire sent by email and therefore most questionnaires were filled at teaching sessions or on the wards and not at the leisure of the junior doctors. This may explain why 24% of the questionnaires were not filled in completely. There was a particular difficulty in obtaining replies from F2 doctors mainly because they have few group teaching sessions. Secondly, the questionnaire only used a three-point scale, providing less information than a five-point scale. Thirdly, this was only a subjective look at how junior doctors rate themselves, and not an objective view of how much knowledge about clinical biochemistry they possess. However, in the current climate of adult learning and self-appraisal these views are valuable. Despite these limitations, the results were felt to be of sufficient general interest to provoke further discussion, particularly as to whether the current training of medical students is fit for the purposes outlined by the GMC. The pattern of answers indicates that foundation doctors are aware of areas of weakness and would like to have more teaching on particular subjects in clinical biochemistry, especially on the subjects of Mg, PO4, haematinics, PTH, short synacthen tests, urine sodium/osmolality and haemolysed samples.
It is not known how many of the respondents trained in Sheffield as the questionnaire was anonymous and the question was not asked. Historically, Sheffield has a very low uptake of trainees from other deaneries and at least 80% of these trainees would have been Sheffield-trained. Due to recent changes in Sheffield teaching, this cohort of F1 and F2 doctors would have received a different training to those currently at medical school in Sheffield. Although elements of clinical biochemistry appeared in their assessments (for example biochemistry results as part of a case scenario), these doctors would not have received any specific teaching of clinical biochemistry under the then current Sheffield curriculum. It is difficult to determine whether the teaching methods now employed with current students, utilizing more problem-based learning, but also with a very limited (3 h) clinical biochemistry input in the final year, will prove more successful in preparing students for utilizing clinical biochemistry laboratory services. However, this survey has highlighted a problem with the apparent knowledge of the current cohort of foundation doctors. The fact that there is little difference between the confidence levels of F1 and F2 doctors suggests that for many tests this is unlikely to improve without further teaching (i.e. through work-related learning alone). However, the two areas where there did seem to be a growth in confidence (U&E and Troponin I) from F1 to F2 are areas where results are used frequently or there are guidelines for the use of biochemical tests. Doctors will have used U&E for assessing hydration, prescribing nephrotoxic drugs, and preoperative and postoperative assessment; and there are clear local guidelines for the use of Troponin I in the accident and emergency department in patients with chest pain. So, this may indicate that with appropriate guidance and sufficient experience, doctors do gain confidence in the use of biochemical tests. Conversely, in those areas where there is infrequent experience, little guidance and less understanding (e.g. Mg or PO4 where the laboratory is often asked for help) doctors do not feel confident in handling the results. In some areas (e.g. haemolysed samples), F1 doctors appear to display more confidence. This may be because they have recently passed their exams and such knowledge is fresher in their mind, which could indicate that some knowledge is lost during training. Alternatively, it may be because they are not as aware of their lack of knowledge as F2 doctors and may feel falsely confident. A surprising finding is that 18% of doctors were confident in requesting tests that they were not confident in interpreting. This may again show some lack of awareness of their own limitations, or may indicate that tests are requested on behalf of senior clinicians without junior doctors understanding how to use them. It would be of considerable interest to extend this study using a revised questionnaire to doctors from other medical schools using different teaching methods. This may indicate whether these results are generalizable or limited to schools like Sheffield with little clinical biochemistry content in the curriculum and thus, try to influence the teaching of clinical biochemistry to UK trainees.
This study has confirmed concerns about the limited extent to which medical students are prepared for their role as foundation doctors looking after patients on the wards. It is clear that additional teaching in clinical biochemistry is required and would be welcomed by the doctors. The topics on which this cohort of Sheffield doctors would like teaching encompassed a wide range of tests and the use of laboratory services in general, suggesting that a fairly comprehensive teaching package is required. The preferred method is small group teaching, which can be delivered to small cohorts of foundation year trainees, although it is often difficult to timetable. This would be better delivered at medical school, possibly in the final year, although there are significant practical difficulties in arranging small group teaching for the whole year cohort of students, especially when laboratory staff are under significant pressure. F1 trainees in Sheffield get protected teaching time, so it may be easier for laboratory staff to access and teach foundation year staff in smaller groups utilizing this protected time. Trainees did indicate that an online tutorial could be a useful adjunct to this teaching and the department is using some online tutorials that are appropriate to the specialty which are available through BMJ learning. 7
Footnotes
Acknowledgements
The substance of this paper was presented as an oral communication and poster at Focus 2007. VK is a foundation doctor (F2). TAG has spent many frustrating hours trying to increase the amount of teaching of clinical biochemistry in the Sheffield curriculum without any success.