
Abstract
Abstract
Phaeochromocytomas are rare tumours that require consideration among large numbers of patients with hypertension. If not diagnosed, the excessive secretion of catecholamines by these tumours can cause considerable morbidity and mortality. With a wide clinical variability in presentation, diagnosis can be difficult and invariably requires the biochemical confirmation of excessive catecholamine production by the tumour. At the First International Symposium on Phaeochromocytoma in October 2005, a panel of experts recommended that initial biochemical testing for phaeochromocytoma should include measurements of plasma and urinary metadrenalines. The accumulated evidence clearly indicates that measurement of fractionated metadrenalines in urine or plasma provides superior diagnostic sensitivity over plasma or urine measurements of catecholamines and metabolites. The low prevalence of phaeochromocytoma and paraganglioma (PGL) emphasizes the need to use biochemical tests of the highest sensitivity. To achieve this, it is recommended that the initial biochemical testing for phaeochromocytoma and secreting PGL should always include the measurements of metadrenalines in plasma or urine or both.
Introduction
Phaeochromocytoma (Phaeo) and functional paraganglioma (PGL) are catecholamine-producing tumours that can present with a wide range of diverse symptoms. Although a rare cause of hypertension, the tumour is frequently sought but rarely found. While the classical clinical triad of paroxysmal hypertension, sweating and tachycardia have high predictive value, the prevalence of the disease in the clinical population with any of these in isolation is low. However, as the tumour can be life threatening, it requires consideration among large numbers of patients. 1,2 To consider the diagnosis is the most crucial initial step in the management pathway while biochemical confirmation of excess tumoral production of catecholamines plays a fundamental role in the diagnosis. 3,4
Because of the low prevalence of Phaeo and PGL, the biochemical tests employed to detect these tumours should have high diagnostic sensitivity, as it is imperative not to miss the diagnosis. This is particularly important when reviewing patients with a hereditary predisposition of developing Phaeo or PGL. 5 Presymptomatic diagnosis is possible in such patients but requires the use of highly sensitive biochemical tests. What is apparent, is the availability of the biochemical tests in any centre will determine the investigation strategy in an individual patient. Thus, recommendation on the most appropriate test(s) and approach tends to be institution-based rather than evidence-based. Centres will also use combinations of biochemical tests to improve the diagnostic sensitivity and although plasma catecholamines are available in specialized centres, the mainstay of biochemical testing in the UK (Table 1) remains the measurement of urinary catecholamines. Yet, recent reports have highlighted the lower sensitivity that quantification of catecholamines in plasma or urine offer when compared with the measurement of metadrenalines. 6–12 In particular, metadrenalines (metanephrines) have been shown to exceed all other biochemical tests for the confirmation of catecholamine-secreting tumours in high-risk individuals with a genetic predisposition. 13
Number of laboratories reporting into the UK National External Quality Assessment Service for urinary catecholamines and metabolites
Initial biochemical screening for phaeochromocytoma
What is clear from the accumulated evidence is that measurement of fractionated metadrenalines (normetadrenaline and metadrenaline) in plasma or urine provides the highest diagnostic sensitivities for detection of Phaeo and PGL. 6–13 The measurement of catecholamines in plasma or urine is not sufficiently sensitive to reliably exclude the presence of a catecholamine-secreting tumour. Even using highly specific analytical procedures such as high-performance liquid chromatography (HPLC) with electrochemical detection (ECD), the measurement of catecholamines does not achieve a comparable sensitivity to fractionated metadrenalines. In a large series involving four referral centres and 214 patients with Phaeo, 6 plasma and urine metadrenalines measured by HPLC were shown to provide sensitivities of >97%, while catecholamines in plasma or urine did not exceed 86% sensitivity (Table 2). The study involved significant numbers of patients investigated because of suggestive signs and symptoms and in whom the diagnosis was excluded or confirmed by criteria that were independent of the biochemical tests being evaluated. This study further confirmed the findings of other reports 7–13 that the measurement of metadrenalines was clearly superior to catecholamines in the diagnosis of sporadic and hereditary Phaeo. The failure of catecholamines to detect Phaeo is not new, as previous reports have highlighted normal excretion patterns in patients with confirmed tumours, with potentially drastic consequences. 14–16 As long ago as 1964, Crout et al. 17 demonstrated that large cystic tumours could present with significantly increased urinary metadrenalines but with almost normal urinary catecholamines due to intratumoral metabolism of catecholamines.
Sensitivities and specificities of various biochemical tests for the diagnosis of phaeochromocytoma in a group of 214 patients with phaeochromocytoma
Adapted from Lenders et al. 6 HPLC, high-performance liquid chromatography
Sensitivity and specificity
The prevalence of phaeochromocytoma in patients with hypertension is estimated to be 0.1–0.5%. 6 With such low disease prevalence, the most important consideration is that the initial biochemical tests should reliably exclude or confirm the presence of a catecholamine-secreting tumour. In this context, the criteria used for test selection will inevitably be biased towards sensitivity. Diagnostic sensitivity and specificity are both dependent on valid reference ranges, derived from a large number of patients in whom the diagnosis has been excluded by tests other than the diagnostic tests being evaluated. The large multicentre study reported by Lenders et al. 6 achieved this goal, highlighting the diagnostic benefits of measuring metadrenalines in plasma and urine. Sporadic Phaeos are frequently larger and generally exhibit symptoms and signs that reflect excessive tumoral production of catecholamines. Thus, biochemical confirmation is more straightforward as catecholamines and metadrenalines are invariably more than four-fold above the upper reference ranges. However, with small tumours that produce and release catecholamines in lower amounts, patients can have an atypical presentation. Detecting the tumour in such patients requires the use of biochemical tests with the highest sensitivities and the finding of normal catecholamine excretion alone cannot reliably exclude the diagnosis of phaeochromocytoma. This is particularly relevant in patients with inherited Phaeo and PGL syndromes, and in patients with incidentally discovered adrenal masses (incidentalomas). While metadrenalines have the highest diagnostic sensitivity, such tests are known to exhibit a lower specificity than catecholamines or vanillymandelic acid (VMA) (Table 2): a feature that can have a negative impact on cost-effectiveness. In other words, there will be more false-positives associated with metadrenaline analysis. Against this must be considered the consequences of missing the diagnosis. A frequent practice is to use a combination of tests. This may improve the diagnostic sensitivity but may decrease specificity. The choice of such tests is again institution based and can include urine VMA and catecholamines, VMA and plasma catecholamines, or urine catecholamines followed by metadrenalines. As false-positive results frequently outnumber true-positive results, the main consideration is to distinguish the true-positive result from the false-positive result in patients with this rare tumour. With biochemical tests such as metadrenalines that have the highest sensitivity, a negative result can provide the best evidence for excluding the disease unlike catecholamines or VMA. Although there will be potentially more false-positive results with such a strategy, repeat testing after elimination of potential medications that can cause false-positive tests such as tricyclic antidepressants (Table 3) can help improve the specificity prior to further investigations such as imaging studies. 6,18,19 In addition, measurement of plasma metadrenalines with greater specificity can help resolve false-positive elevations observed more frequently with urine metadrenalines. Invariably, there will be exceptions such as small Phaeos <1 cm that may not produce catecholamines in sufficient amounts to be detected biochemically and will evade diagnosis irrespective of the biochemical testing strategy.
Examples of interferences associated with measurement of catecholamines and metadrenalines
HPLC, high-performance liquid chromatography
Why do metadrenalines achieve better sensitivity?
Measurement of fractionated metadrenalines exhibit superior sensitivity due to their continuous production within Phaeos, a process that occurs independently of catecholamine secretion by the tumour. Phaeos contain high concentrations of catechol-O-methyltransferase, an enzyme that metabolizes catecholamines into free metadrenalines. 20 Production of free metadrenalines within tumour cells is an ongoing process as catecholamines leak from storage vesicles. Even when the release of catecholamines into the bloodstream by the tumour is intermittent or at very low rates, the metabolism of catecholamines to free metadrenalines within the tumour cells will continue. Although current recommendations 21,22 for the initial biochemical detection of Phaeo includes the measurements of fractionated metadrenalines (normetadrenaline, metadrenaline, 3-methoxytyramine) in plasma or urine, many biochemistry laboratories in the UK seem to rely solely on the measurement of urinary catecholamines to exclude the presence of catecholamine-secreting tumours. Why is the UK seemingly ignoring the evidence?
Current practice in the UK
A recent report from the UK National External Quality Assessment Service (UKNEQAS) group (Table 1) indicates that presently there are more laboratories measuring urinary catecholamines (noradrenaline, adrenaline and dopamine) than fractionated metadrenalines (normetadrenaline, metadrenaline). There were 92 laboratories reporting urinary catecholamine while 42 laboratories reported fractionated metadrenaline results. Thus >50% of laboratories reporting in the UKNEQAS scheme appear to be relying exclusively on catecholamines to exclude or confirm the biochemical diagnosis of this rare tumour. This will have a serious impact on the detection of Phaeo (Table 2). In addition, there were more laboratories measuring VMA concentrations than fractionated metadrenalines (58 and 42, respectively). Some of these laboratories will be using VMA analysis in conjunction with homovanillic acid for the diagnosis and prognosis of neuroblastoma. However, it is very worrying that a biochemical test that has been shown to exhibit the poorest sensitivity of all the tests for detecting a Phaeo may still be utilized in the UK in the initial investigation of patients for this rare tumour. 6,23,24 With the highest sensitivity of all the biochemical tests, a finding of a normal result for urine or plasma metadrenalines provides a high probability of excluding the presence of Phaeo. In contrast, the use of catecholamines and VMA for the initial biochemical testing does not reliably exclude the presence of the tumour. The limitations of measuring catecholamines and metabolites such as VMA in the initial biochemical screening of patients for the presence of a catecholamine-secreting tumour is summarized in Figure 1.
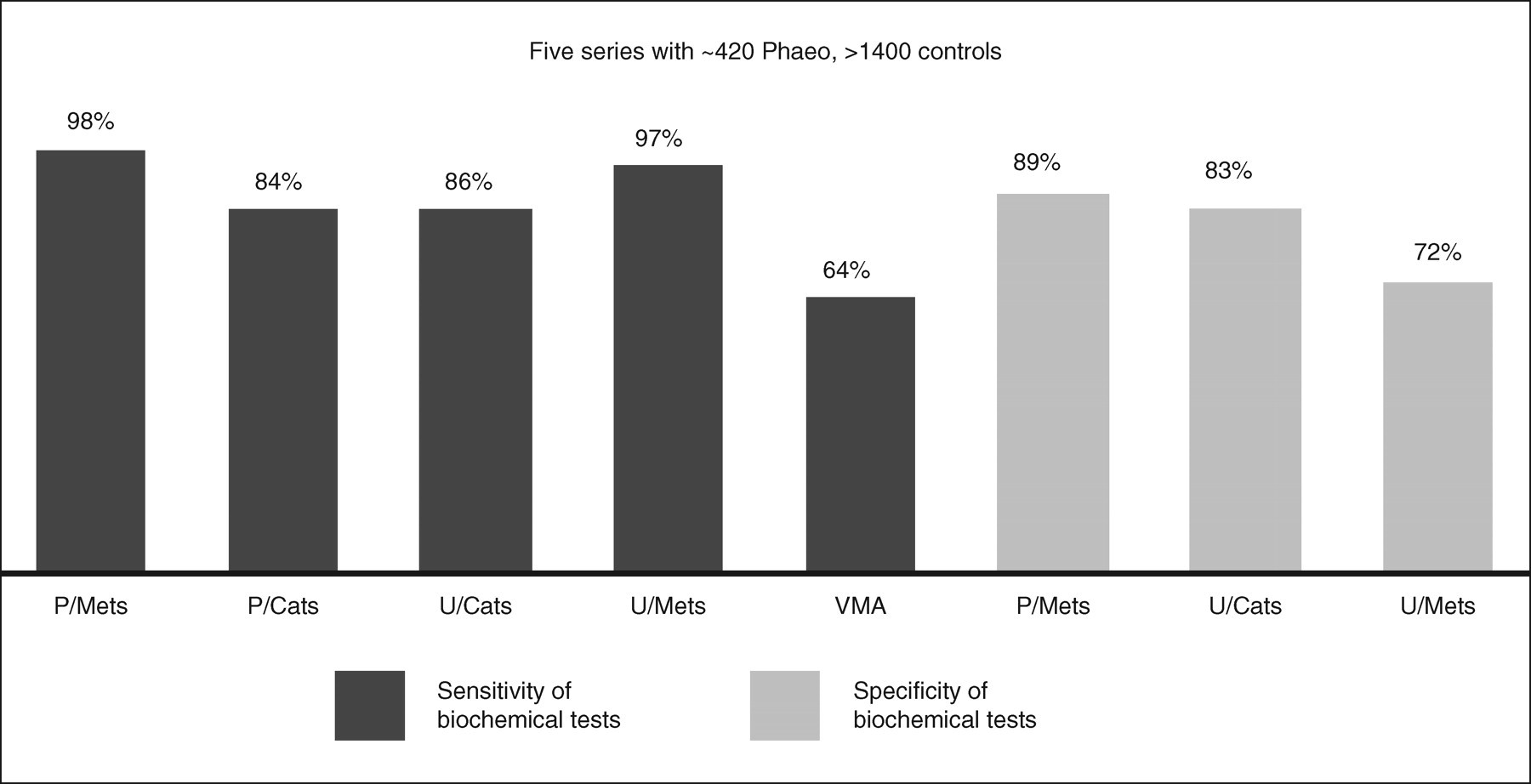
Summary of five reports dealing with the diagnostic sensitivity and specificity of biochemical tests in the detection of phaeochromocytoma. P/Mets, plasma metadrenalines; P/Cats, plasma catecholamines; U/Cats, urinary catecholamines; U/Mets, urinary metadrenalines; VMA, vanillymandelic acid
Plasma or urine metadrenalines?
Lenders, Eisenhofer and others have aptly demonstrated that plasma metadrenalines offer the highest diagnostic sensitivity of all the biochemical tests for the detection of Phaeo. 6,8–13 However, the differences in sensitivity between urine and plasma are relatively small (Table 2 and Figure 1) and while plasma metadrenaline analysis avoids the problems associated with urine collections, the test is presently available in very few centres. This has led to recommendations that when plasma metadrenaline analysis is not available, urine-fractionated metadrenalines should be utilized in the initial investigation of patients with suspected Phaeo. 21 As there are commercial procedures available for both urinary catecholamines and metadrenalines and the analysis can be performed on the same HPLC equipment, changing protocols from measuring catecholamines to metadrenalines should not present too much difficulty. What is apparent from the evidence is that fractionated metadrenalines in either plasma or urine should replace catecholamines and VMA in the initial biochemical screening for Phaeo. The choices of plasma or urine metadrenalines will invariably depend on the pretest probability for the disease. Plasma metadrenalines with the highest sensitivity are the test of choice in patients with a high probability of developing Phaeo such as individuals with genetic syndromes, past history or family history of Phaeo. While plasma metadrenalines measured by HPLC/ECD is a particularly challenging procedure, a recent report has utilized a radioimmunoassay method in the investigation of patients with suspected phaeochromocytoma. 8 Until plasma metadrenaline measurements are more widely available, urine metadrenalines should be used in preference to catecholamines in patients with relatively low risk such as hypertension. However, with a lower specificity and potentially increased frequency of false-positive results, due consideration should be given to the magnitude of any increased metadrenaline values. A single urinary metadrenaline concentration slightly above the upper reference ranges will only marginally increase the pretest probability of a tumour being present, while an elevation of four-fold above the intervals can almost provide 100% probability of a Phaeo. To improve the interpretation of urinary metadrenalines, use of a formula incorporating age- and sex-specific reference ranges has also recently been shown to improve the sensitivity and specificity of urinary metadrenaline measurements in an unselected hospital population. 25 In addition, after exclusion of false-positives due to medication (Table 3) and repeat testing, subsequent measurement of plasma metadrenalines with blood samples collected in the supine position to maintain the highest diagnostic sensitivity and specificity 26 can further help distinguish true-positives from false-positives. Compared with measuring urinary catecholamines, there are additional benefits associated with measuring urine metadrenalines. Willemsen et al. 27 has demonstrated the stability of metadrenalines in urine samples without preservatives, thus offering the possibility of urine collections without acid preservatives.
Conclusion
Without doubt, clinical suspicion of Phaeo remains the single most important factor while diagnosis crucially depends on biochemical confirmation of increased catecholamine production by the tumour. Accumulated evidence over the last 10 years strongly indicates that the measurement of metadrenalines in plasma and urine offer significant advantages over the measurement of catecholamines in the diagnosis of this rare tumour. In the initial biochemical investigation of patients with possible Phaeo, it is recommended that the current practice of relying on catecholamine and VMA measurements should stop and be replaced with metadrenaline analyses in plasma and urine. Laboratory medicine is well experienced in the selection of the most appropriate test and strategies for ruling in or ruling out the likelihood of a diagnosis. The biochemical diagnosis of phaeochromocytoma is such an example.
Footnotes
Acknowledgement
We are most grateful to Dr Finlay MacKenzie at UKNEQAS for his permission to include examples of UKNEQAS data.