
Abstract
Abstract
There are currently no simple tests in clinical use to detect acute placental damage. A case is described to demonstrate that a routinely used measurement such as alkaline phosphatase (ALP) can be employed to detect acute damage to the placenta. Seventeen serial blood samples, three pre-delivery, were collected from a 22-year-old primigravida who delivered a stillborn baby. Retrospectively, blood samples were analysed for total and heat-stable ALP as well as human chorionic gonadotropin (hCG) and alpha-fetoprotein (AFP) as a measure of placental function when an unusual pattern of change in ALP was noticed. Histological examination of the placenta revealed new and old placental infarcts. Total and heat-stable ALPs as well as AFP peaked by more than eight-, 19- and two-fold, respectively over 16 h. Plasma hCG fell sharply even before delivery of placenta by five-fold over 16 h before further falling slowly to baseline. The fall in hCG is also consistent with the placental damage being acute and critical. As far as we are aware this is the first description of changes in circulating proteins reflecting placental damage.
Introduction
Good obstetric practice involves appropriate assessment to detect and optimally manage the pregnant state. Placenta forms the interface between the mother and the fetus delivering oxygen and nutrients as well as removing carbon dioxide and waste. Damage to the placenta interferes with this crucial function and indicates a high-risk pregnancy requiring a change in therapeutic approach. There are currently no routine tests in clinical use to detect acute placental damage except ultrasound. Traditional monitoring of pregnancy has shown that plasma alkaline phosphatase (ALP) increases gradually approximately four- to six-fold during pregnancy to reach a peak value at the third trimester before declining promptly after the placenta has been delivered. 1 A steadily rising ALP has been used as a placental function test. 2 This is based on the fact that the placenta produces and secretes ALP into the maternal circulation and a larger functional placental mass is associated with higher circulating ALP. An inadequate rise in ALP has been associated with intrauterine growth retardation (IUGR) due to inadequate placental mass and function. 3
The course of pregnancy in a primigravida is described below when serendipity allowed a unique pattern of rise in ALP and other proteins to be recognized.
Case report
A 22-year-old primigravida with a low-risk pregnancy with uncomplicated antenatal course of 37+2 weeks' gestation was admitted with acute abdominal pain and no fetal movements. At admission she was pale, anxious, with a blood pressure 128/87 mmHg, pulse 108/min. Ultrasound scan revealed placental abruption and intrauterine death of the fetus. A stillborn male baby was delivered weighing 3.28 kg. The patient was resuscitated following infusions of blood and crystalloids and made a full recovery 14 days later. During her hospital stay blood samples were collected as part of her clinical management and an unusual pattern of change in ALP was noticed and is shown in Figure 1. Seventeen serial blood samples, three pre-delivery, were collected and blood samples were retrospectively analysed for total and heat-stable ALP as well as human chorionic gonadotropin (hCG) and alpha-fetoprotein (AFP) as a measure of placental function. Histological examination of the placenta was also carried out.
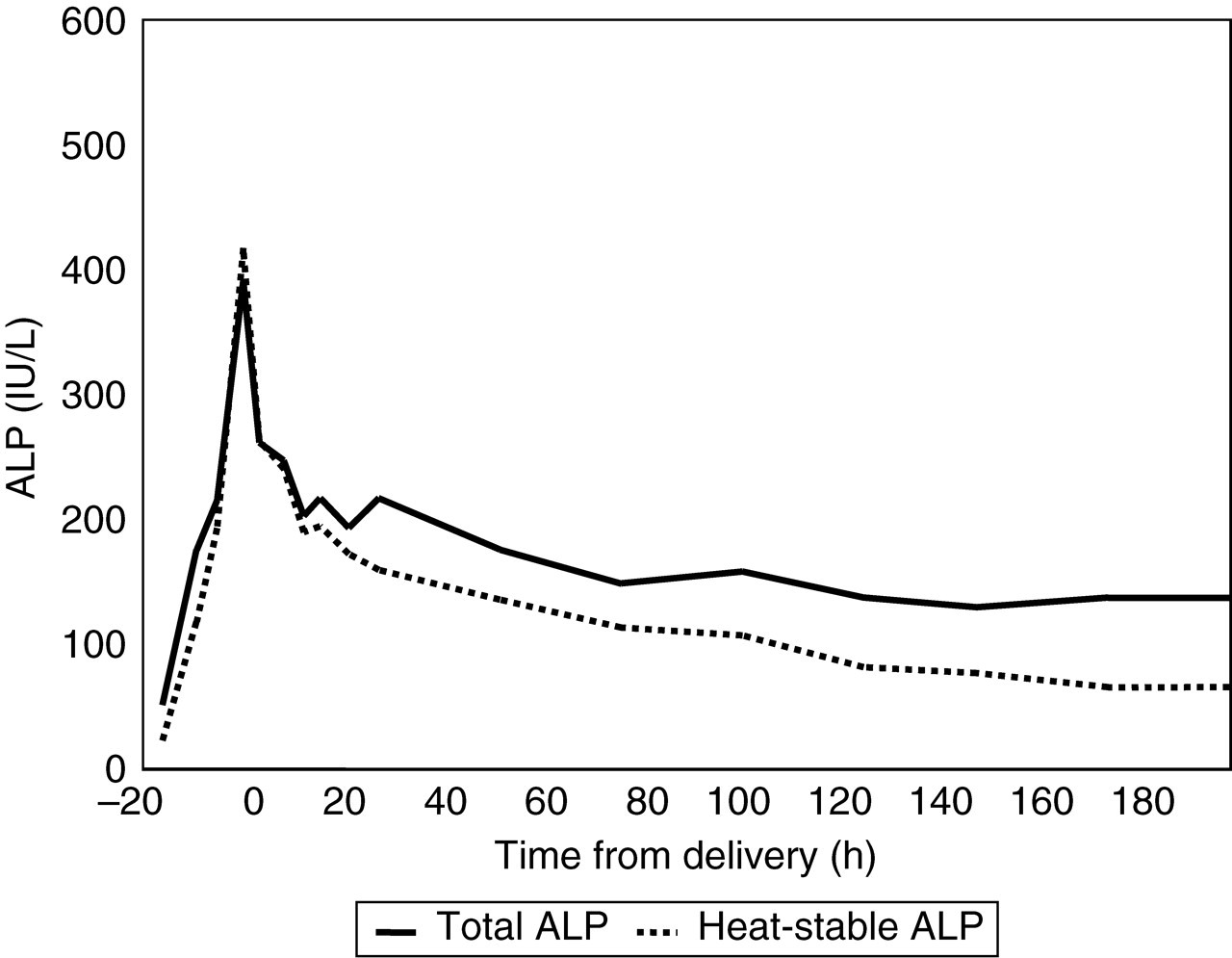
Profile of change in total and heat-stable alkaline phosphatase (ALP)
Changes in circulating proteins: Over a period of 16 h the ALP rose from 50 to 391 U/L (third trimester reference range 133–418 U/L) and following delivery of the still-born fetus and the placenta, before gradually decreasing over the next five to seven days into the reference range. The sudden increase in ALP is shown in Figure 2 comparing it with the change in ALP in a normal pregnancy. The gel electrophoresis of the peak ALP is shown in Figure 3 confirming the predominant heat-stable nature of the enzyme. Other placental proteins hCG and AFP were also measured on all samples collected (Figure 4). hCG was appropriately high soon after admission suggesting that placenta was viable or in the very early stages of damage at this time declining rapidly to time of delivery. AFP increased by 2.3-fold to a peak value at delivery before decreasing sharply after delivery to pre-pregnant concentrations.
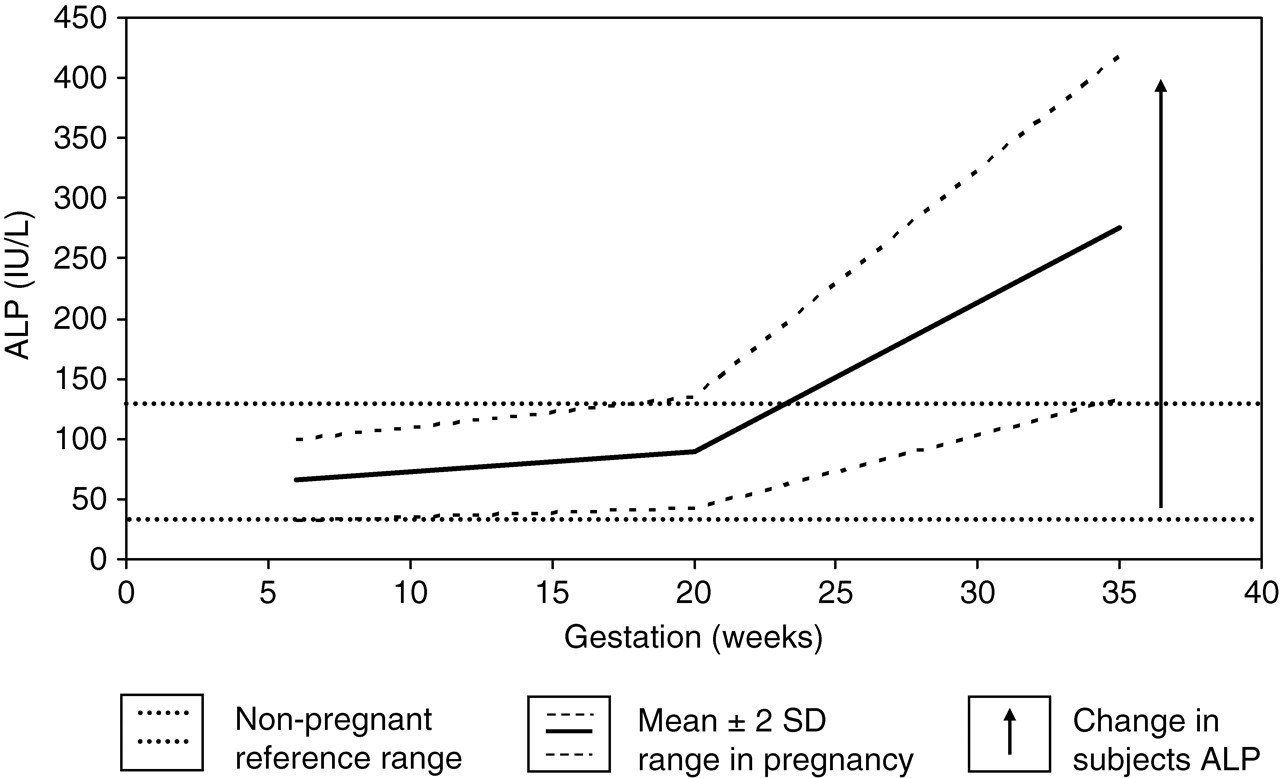
Variation in total alkaline phosphatase (ALP) in pregnancy
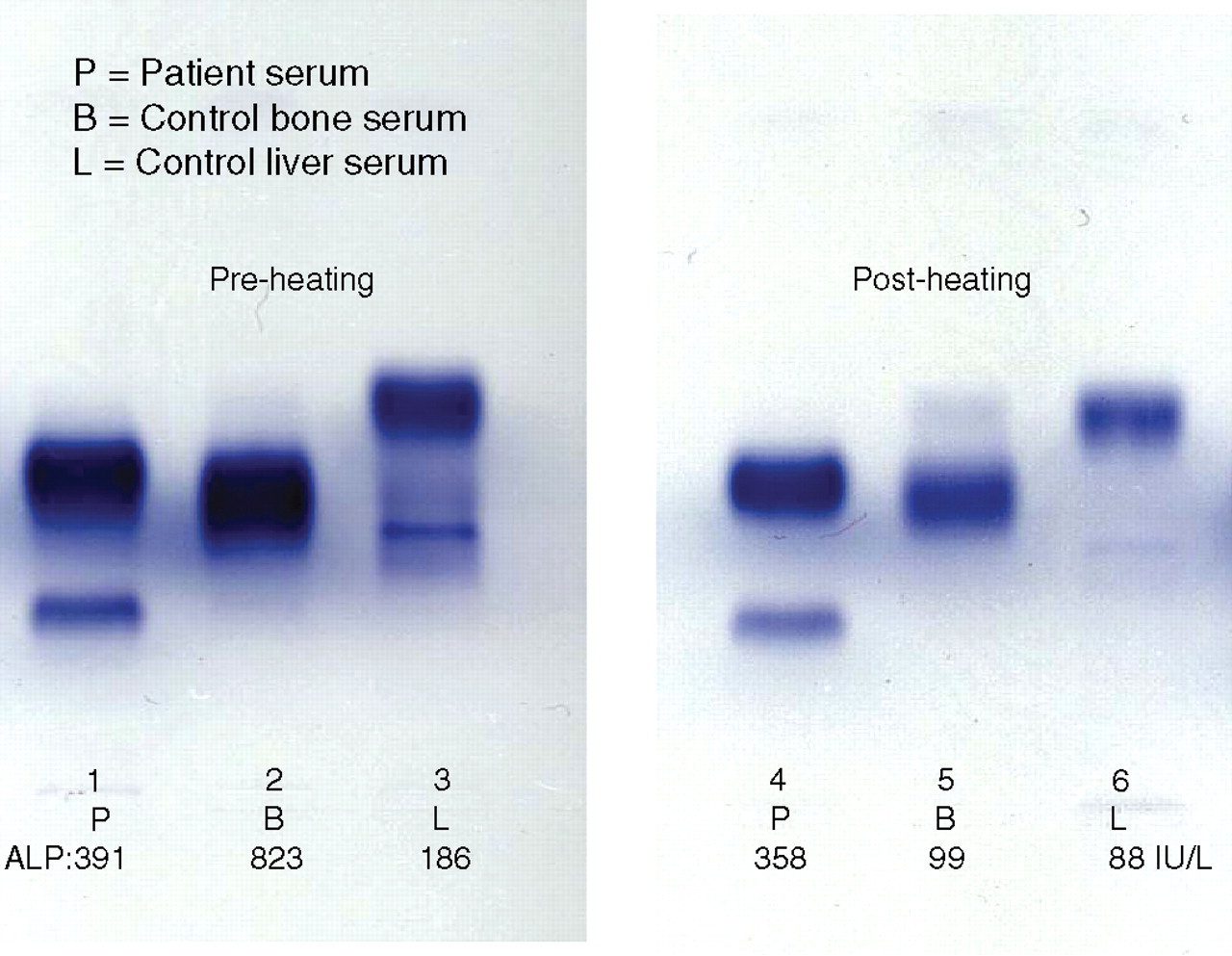
Electrophoresis of alkaline phosphatase (ALP). Tracks 1 to 6 show serum electrophoresis of ALP isoenzymes prior to and following heating to 56ºC
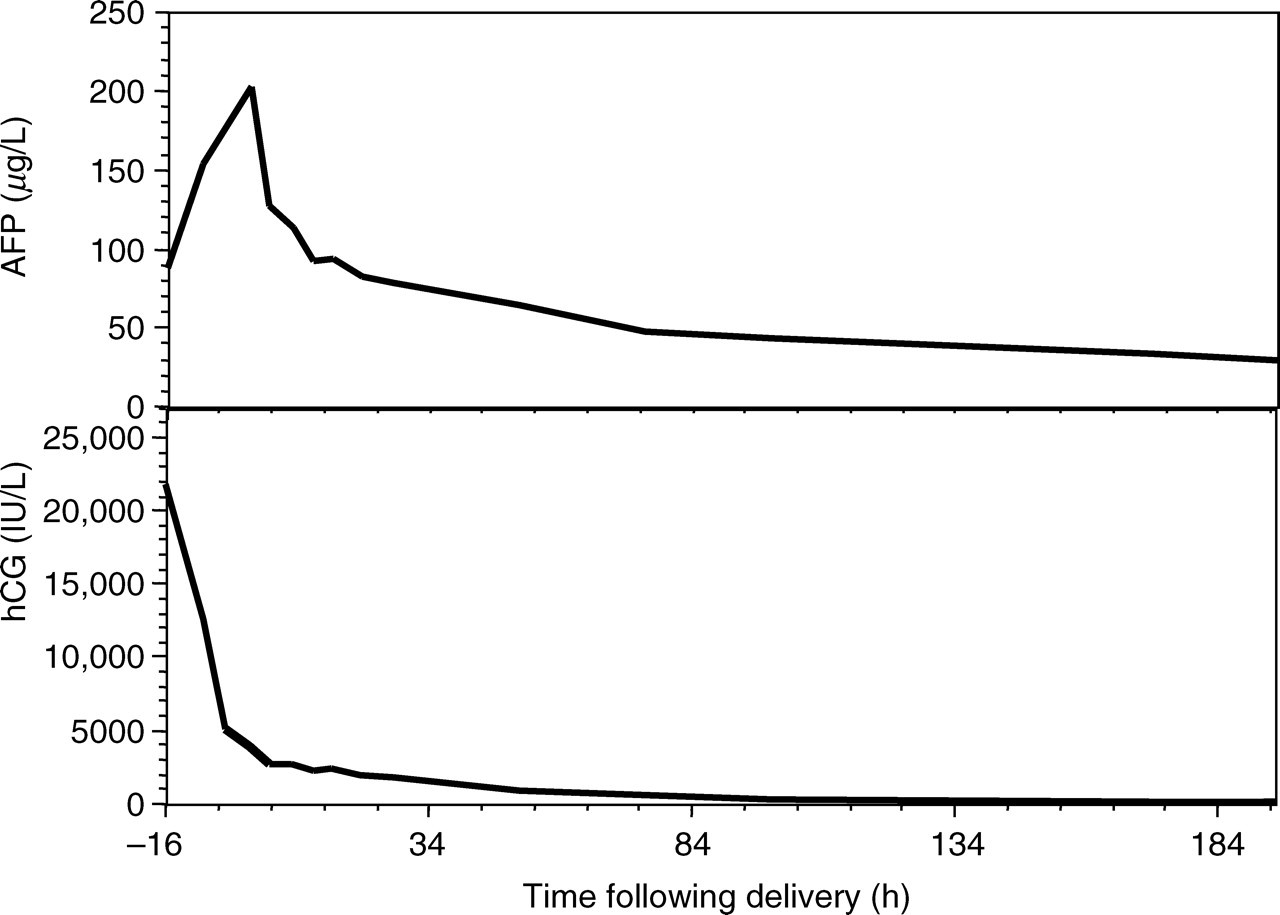
Profile of change in plasma human chorionic gonadotropin (hCG) and alpha-fetoprotein (AFP)
Histological examination of placenta: Macroscopically, the oval discoid-shaped placenta weighed 535 g and measured 26 × 16 × 2 cm. The cord was eccentric in insertion and was 30 cm long and 1.2 to 1.5 cm in diameter. On cut section a relatively large ill-defined area of established infarction with foci of thrombosis and haemorrhage on the maternal surface was seen. On microscopy, sections showed villous architecture consistent with term pregnancy. The majority of the sections showed extensive ill-defined and partly confluent infarctions of various age. The remaining villi showed features of accelerated maturation. In conclusion, histology of the placenta showed multiple old and new infarctions.
Discussion
The ALP at admission was low normal with approximately 40% heat-stable fraction (HS-ALP) and rose rapidly to a peak 16 h later when delivery of fetus and placenta occurred. The HS-ALP comprised almost 100% of the ALP activity at 16 h suggesting that the placenta was not acutely damaged at admission, but soon after this. HS-ALP, a tetramer with a molecular weight (MW) of 300,000, is synthesized in the placenta by the cells of the syncytiotrophoblast and is the product of a unique gene. 4 Specific activity of ALP, in IU per gram of wet tissue, is highest in the placenta and the specific activities in the various organs are: placenta 3214, intestine 2524, kidney 619, bone 571 and liver 100. 5 Damage to cardiac muscle leads to release of tissue proteins and enzymes such as myoglobin, troponins, creatine kinase, alanine and aspartate transaminases into the circulation and their measurement continues to be used in the diagnosis of myocardial infarction. It is therefore not difficult to see how damage to the placenta can likewise lead to release of ALP and other proteins into the circulation.
ALP is released into the circulation by the placenta in healthy pregnancy. 6 The highest HS-ALP is found in labour when presumably physiological placental damage is most likely. 1 The first blood sample obtained at admission showed ALP concentrations that were non-elevated and were in fact in the low-normal non-pregnant reference range. Low ALP in pregnancy has been shown to predict IUGR of the fetus and a high-risk pregnancy, 3 and the low ALP during pregnancy probably reflects a reduced mass of viable placental tissue. In the present case the baby was 3.28 kg and it would appear that development of the fetus in utero was not significantly compromised. There may be a reserve capacity of the placenta that may have to be compromised before it results in an adverse fetal outcome. Since the histological examination of the placenta showed old and new infarcts, the possibility that placental function was damaged earlier in pregnancy, but not to a critical level, as reflected by the low ALP at admission, cannot be excluded.
The half-life of ALP is highly variable and depends upon the type of isoenzyme. Previous studies have indicated that the placental type has the longest half-life of around four to seven days. 5 The terminal half-life of the HS-ALP was 102 h in the present report and is consistent with earlier studies. The implication of the relatively long half-life is that it makes it more likely that a random blood test screen in pregnancy may identify the increase.
It is suggested based on previous studies and our own experience with this case that both a low ALP and a high ALP (preferably an acutely rising ALP) in pregnancy may each predict a high-risk pregnancy although the mechanisms underlying the diametrically opposite changes may be similar but seen at different points in their evolution.
Circulating hCG in the patient described here decreased rapidly to very low concentrations during the first 16 h followed by a more gradual decline over the subsequent days (Figure 3). hCG is a dimeric glycoprotein consisting of non-identical α and β subunits, with a MW of 37,900 daltons. 7 It is synthesized and secreted by the syncytiotrophoblast of the placenta and is an important hormone for the maintenance of pregnancy. 8 Following delivery, hCG concentrations in the circulation decrease due to the absence of the placenta. Since the hCG in the circulation is heterogeneous in terms of glycosylation and other properties, clearance from the circulation is variable. 9 An initial rapid half-life between 0 and 48 h and a late half-life of two to seven days have been reported as was also observed in this case. 10
Plasma AFP rose sharply by 2.3-fold to peak at 16 h (at delivery) followed by a steady decline over the next several days. The terminal half-life of AFP in the maternal circulation was 94.8 h in our patient and compares reasonably with that reported in the literature of 5–6 days. 10 AFP is a glycoprotein with a MW of 70,000 daltons and is produced initially by the yolk sac and then by the fetal liver. 7 Some investigators have suggested a role for the placenta in synthesis of AFP 11 although others have not confirmed this. 12 The presence of AFP in the maternal circulation may reflect diffusion down a concentration gradient in healthy pregnancy. 11 If the feto–maternal barrier is disrupted, fetal blood enters the maternal circulation leading to a rapid and acute rise in AFP, as was seen in the patient described in the present report.
The acute rise in total and HS-ALP as well as AFP may indicate the release of these stored proteins following damage from the placenta. Figure 5 shows a diagrammatic representation of ALP, AFP and hCG in relation to placenta and the fetal and maternal circulations. The fall in hCG is also consistent with the placental damage being acute, critical and catastrophic. We describe a potentially simple and inexpensive way to monitor pregnancies for placental damage or infarction by serial plasma monitoring of ALP and other proteins.
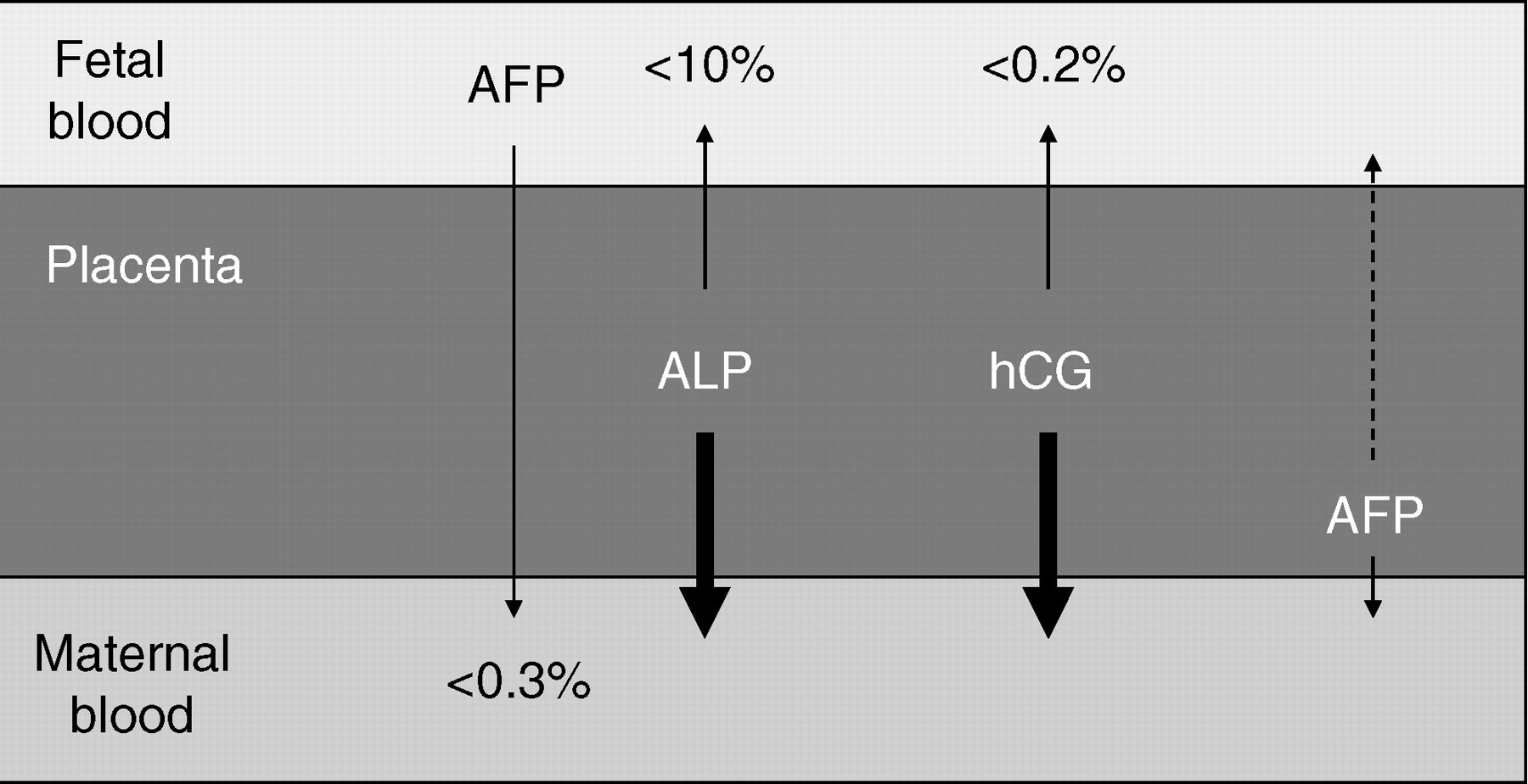
Placental localization of alkaline phosphatase (ALP)/human chorionic gonadotropin (hCG)/alpha-fetoprotein (AFP)
There are a number of published reports both in the second trimester and at other times during a pregnancy when elevated AFP has been recognized. These unexpected elevations have been associated with increased risk of premature births, 13 low birth weight and IUGR. 14 It has been suggested that the combination of elevated ALP and AFP may further improve the detection of a high-risk pregnancy. 14 Other studies have suggested that unexplained elevations of AFP and hCG may be associated with intrauterine death, antepartum haemorrhage and pre-term delivery. 15 High maternal AFP and placental sonolucencies have been linked to pregnancy complications and attributed to placental damage. 16 Most of these associations of elevated AFP and hCG have been attributed to ischaemia and damage to placenta. A histological study of placentas in those with unexplained elevations of AFP concluded that ischaemia of the placenta was responsible for complications of pregnancy and fetal growth restriction. 17
The present study revealed the profile of circulating proteins typical of damage to an organ, in this case the placenta. Although earlier recognition of such a change may not have affected the outcome in the present case, this may provide a valuable tool to monitor high-risk pregnancies with opportunities for earlier intervention to save the pregnancy. As far as we are aware this is the first description of changes in circulating proteins reflecting placental damage. We suggest that ALP is a cheap and routinely performed assay that can be utilized in the monitoring of pregnancy.