
Abstract
Abstract
Background
An imbalance between oxidative damage and antioxidative protection in association with the pathophysiology of atherosclerosis has been suggested. The aim of this study was to test the parameters of antioxidative defence and to assess their association with hyperhomocysteinaemia and the severity of coronary heart disease (CHD) in Tunisian patients.
Methods
The study population included 100 patients with CHD and 120 healthy controls. The severity of CHD was expressed as the number of affected vessels. Superoxide dismutase (SOD) activity, glutathione peroxidase (GPx) activity and total antioxidant status (TAS) concentrations were measured using commercially available methods. Plasma total homocysteine (tHcy) concentration was determined by direct chemiluminescence assay. Serum zinc (Zn) was measured by a colorimetric method.
Results
Compared with healthy control subjects, patients with CHD had significantly lower activities of SOD (P < 0.01), GPx (P < 0.001), and serum Zn concentrations (P < 0.001) and significantly higher tHcy concentration (P < 0.001). However TAS concentrations were not significantly different between the groups. SOD and GPx activities were negatively correlated with tHcy concentration (P < 0.05, P < 0.001, respectively). Patients with hyperhomocysteinaemia showed a lower GPx and SOD activities than patients with normohomocysteinaemia. Antioxidant enzyme activities tended to be decreased in CHD patients presenting with 0- to 3-vessel stenosis.
Conclusions
This study indicates that low activity of GPx, SOD and Zn concentration are associated with CHD patients. We hypothesize that hyperhomocysteinaemia and low antioxidant enzyme activities may increase the extent of CHD.
Introduction
A dramatic increase in the incidence of coronary heart disease (CHD) has recently been observed in the Tunisian population. 1 This disease is associated with both genetic and environmental factors, including nutritional status, smoking and lack of physical activity. We reported in previous studies that hyperhomocysteinaemia is a risk factor for CHD. Hyperhomocysteinaemia with genetic factors such as methylenetetrahydrofolate reductase, endothelial nitric oxide synthase genes or with low paraoxonase activity led to increased risk of CHD severity. 2–4 Oxidative stress plays an important role in the pathogenesis of atherosclerosis and CHD. Reactive oxygen species (ROS) production is toxic via their effects on cellular components such as denaturing proteins, membrane lipids and DNA. Oxidative stress may be defined as an imbalance between the production and degradation of ROS such as superoxide anion, hydrogen peroxide, lipid peroxides and peroxynitrite. Enzymatic inactivation of ROS is achieved mainly by glutathione peroxidase (GPx), superoxide dismutase (SOD) and catalase. 5 GPx, the ubiquitous intracellular form and key antioxidant enzyme within most cells, including the endothelium, uses glutathione to reduce hydrogen peroxide to water and lipid peroxides to their respective alcohols, 6 and it also acts as a peroxynitrite reductase. 7 In mice, GPx deficiency results in abnormal vascular and cardiac function and structure. 8 Similarly, SOD is represented by three different ubiquitously expressed enzymes that convert superoxide anion to hydrogen peroxide: cytosolic copper- and zinc-containing SOD, mitochondrial manganese-containing SOD and extracellular SOD. Extracellular SOD is most active in the vessel wall and has been shown to regulate the availability of nitric oxide by scavenging superoxide anion. 9 Several methodologies for measuring the total antioxidant capacity of biological and natural products were developed in the 1980s and 1990s. The total peroxyl radical trapping parameter assay 10 and oxygen radical absorbance capacity assay 11 have been widely used for the measurement of antioxidant capacity in foods and biological materials. Rice-Evans et al. 12 developed the total antioxidant status (TAS) method, based on inhibition of the radical cation absorbance caused by antioxidants. Many antioxidant molecules such as albumin, uric acid, bilirubin and proteins which contain thiol or metal groups are found in the blood. 13 Individual antioxidants concentration or activity indicates the antioxidant characteristics of only one antioxidant, whereas TAS may represent the total antioxidant characteristics of all antioxidants found in the serum. The TAS method is a particularly simple and accurate method of estimating the total antioxidant capacity of plasma. Consequently, this method has been used in various clinical subjects, including patients with diabetes mellitus, and patients with hypertension or CHD. The TAS was shown to be significantly reduced in these patients compared with healthy subjects. 14–16 Experimental and clinical studies indicate that zinc (Zn) deficiency may predispose to diabetes mellitus, atherosclerosis and CHD. 17,18 Few studies have been undertaken to investigate the parameters of antioxidative defence and Zn concentration in the presence of CHD in the Tunisian population. In this study, we investigated the relationship between the parameters of antioxidative defence (GPx, SOD activities and TAS concentration), Zn concentration and severity of CHD, and their correlation with hyperhomocysteinaemia.
Materials and methods
Study population
The study population was of homogenous Tunisian Arab descent, was resident in Tunisia, and had no known negroid or mongoloid ancestry.
The control group consisted of 120 healthy volunteers (87 men and 33 women) with no history of coronary artery disease, diabetes mellitus or cerebrovascular diseases. Their median age was 50 (45–60) years.
One hundred consecutive patients with angiographically documented CHD were enrolled from the Cardiovascular Department, University Hospital Fattouma Bourguiba in Monastir (Tunisia). The median age of this group was 57 (49–63) years and consisted of 74 men and 26 women. The number of significantly stenosed (50% luminal stenosis) coronary arteries and lesions determined the severity of CHD. The angiograms were assessed by two cardiologists who were unaware that the patients were to be included in the study and allowed a patient subclassification as follows: Group G0 (10%) without stenosed vessels, group G1 (40%) with one stenosed vessel, group G2 (35%) with two stenosed vessels and group G3 (15%) who had severe CHD involving all the three major coronary arteries.
All participants were interviewed, and data on dyslipidemia, diabetes mellitus, hypertension, smoking habits were recorded. Informed written consent was obtained from each patient and healthy subject according to the guidelines of our ethics committee. For coronary risk factors, the following definitions were used: individuals were defined as hypertensive if their blood pressure was >140/90 mmHg or if they were receiving any antihypertensive treatment; individuals with a history of diabetes mellitus or those receiving any antidiabetic medication were considered to be diabetic; individuals were deemed dyslipidemic when their total cholesterol concentration was ≥5.68 mmol/L, or their triglyceride concentration was ≥2.28 mmol/L, or they were receiving lipid-lowering drugs. Smoking history was coded as never and current smoker (number of cigarettes smoked ranged from 15–40 cigarettes/day).
Measurements of lipids, total homocysteine, glutathione peroxidase, superoxide dismutase, total antioxidant status and zinc concentrations
Fasting blood samples were taken at 08:00–09:00 h, and serum separated by centrifugation at 1500
Glutathione peroxidase and SOD activities were determined in washed red cells prepared immediately after sampling from whole blood anticoagulated with EDTA. Cell lysates were stored frozen for up to one week; freezing does not lead to changes in enzyme activity. The intra-assay coefficients were 6.7% and 9.9%, respectively. Plasma TAS was measured with commercial kits (Randox Laboratories) on the RA 1000 auto analyser according to the method of Miller et al. 20 Zn was measured by direct colorimetric method. 21
Statistical analysis
Statistical analyses were performed using SPSS for Windows 10.0 (SPSS Inc, Chicago, IL, USA). Differences between the means of the two continuous variables were evaluated using the student's t-test. Comparisons between groups >2 were performed by one-way analysis of variance (ANOVA). Simple associations between variables were calculated as the Pearson correlation. Hyperhomocysteinaemia was defined as a mild increased tHcy (fasting tHcy >15 μmol/L). Results were expressed as the median and 25th and 75th percentiles, and P < 0.05 was considered statistically significant.
Results
Difference between patients versus controls
Clinical characteristics of CHD patients and control groups are shown in Table 1. There were no differences in the mean age, body mass index (BMI), and sex between the two groups, while the median of triglyceride, total cholesterol, LDL-cholesterol and tHcy were significantly higher in CHD group than in the control group. However the median HDL-cholesterol, GPx, SOD activities and Zn concentration were significantly lower in the CHD group than in the control group. Plasma TAS was not significantly different between the groups.
Clinical and biochemical features of cases and controls
Values are expressed as median (25th–75th percentile) or number (%)
NS, not significant; CAD, coronary artery disease; BMI, body mass index; SOD, superoxide dismutase; GPx, glutathione peroxidase; TAS, total antioxidant status
Homocysteine, glutathione peroxidase and superoxide dismutase activities and severity of coronary heart disease
Patients with CHD (n = 100) were subclassified into four subgroups (G0, G1, G2, and G3) according to the number of affected coronary arteries (Figure 1). Plasma tHcy tended to increase with more severe coronary atherosclerosis, while GPx and SOD activities tended to be decreased with CHD severity. GPx and SOD activities decreased markedly in patients with 3-vessel stenosis compared with patients with 0-vessel stenosis (P < 0.01). Patients with hyperhomocysteinaemia (48%) had lower GPx, SOD, and Zn concentrations than patients with normohomocysteinaemia (P < 0.01) (Table 2).
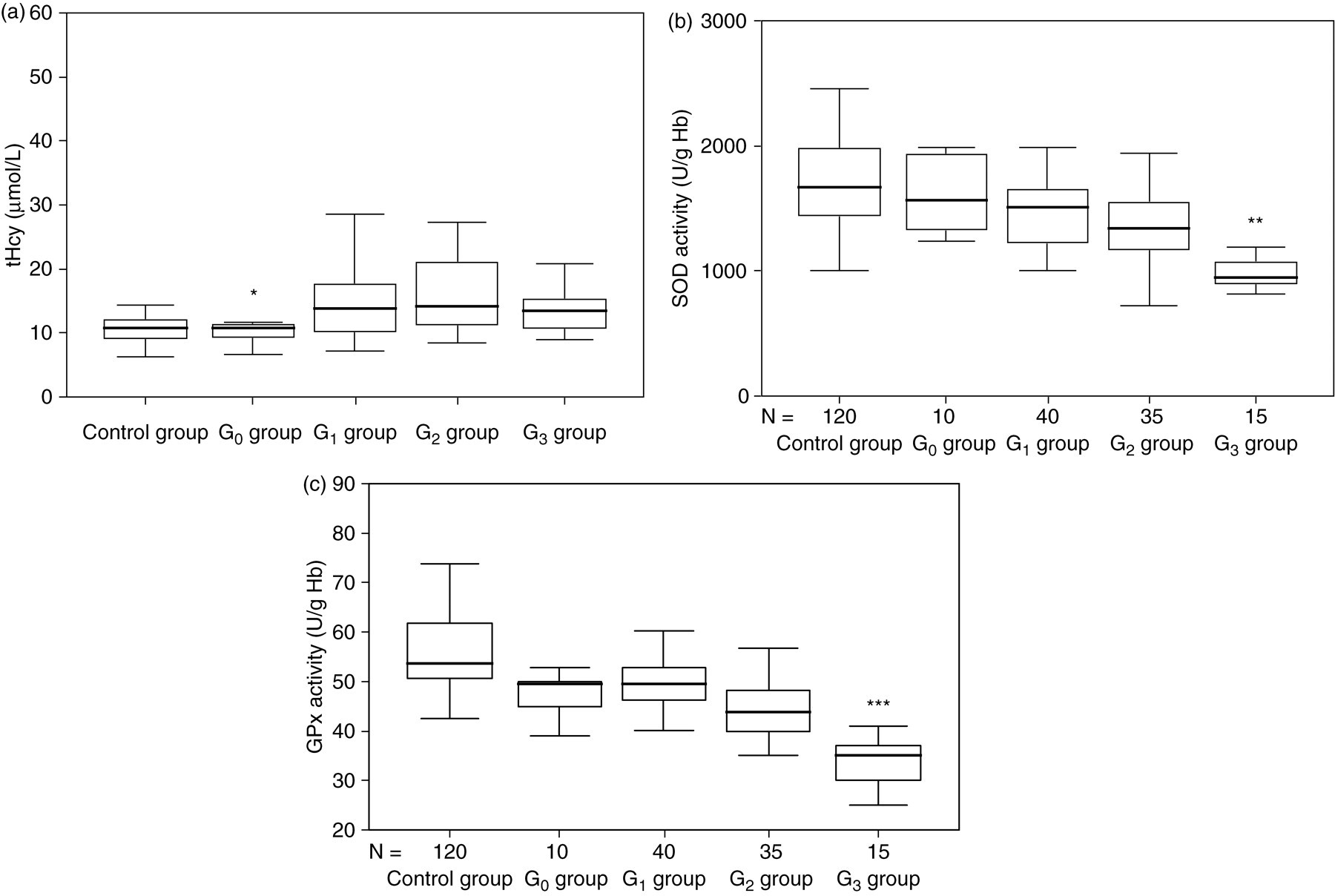
Comparison of the control group and patient subgroups (G0, G1, G2 and G3) according to the concentration of: (a) plasma total homocysteine (tHcy), (b) superoxide dismutase (SOD) activity or (c) glutathione peroxidase (GPx) activity. *P < 0.05 compared with G1, G2 and G3 groups. **P < 0.01 compared with G0 group and with G1 group. ***P < 0.001 compared with G0, G1 and with G2 groups
Glutathione peroxidase (GPx), superoxide dismutase (SOD) activities, total antioxidant status (TAS), zinc concentrations and coronary artery disease patients with normo- and hyperhomocysteinaemia
Values are expressed as median (25th–75th percentile)
*P < 0.05 compared with normohomocysteinaemia
**P < 0.01 compared with normohomocysteinaemia
Results of Pearson correlation
We studied the Pearson correlation between the GPx and SOD activities, and some variables in CHD patients. We found that GPx activity showed a negative correlation with smoking (r = −0.270, P = 0.017) and a negative correlation with hypertension (r = −0.275, P = 0.017). GPx and SOD activities showed a negative correlation with homocysteine (Figure 2) (r = −0.42, P < 0.001; r = −0.20, P = 0.014, respectively).
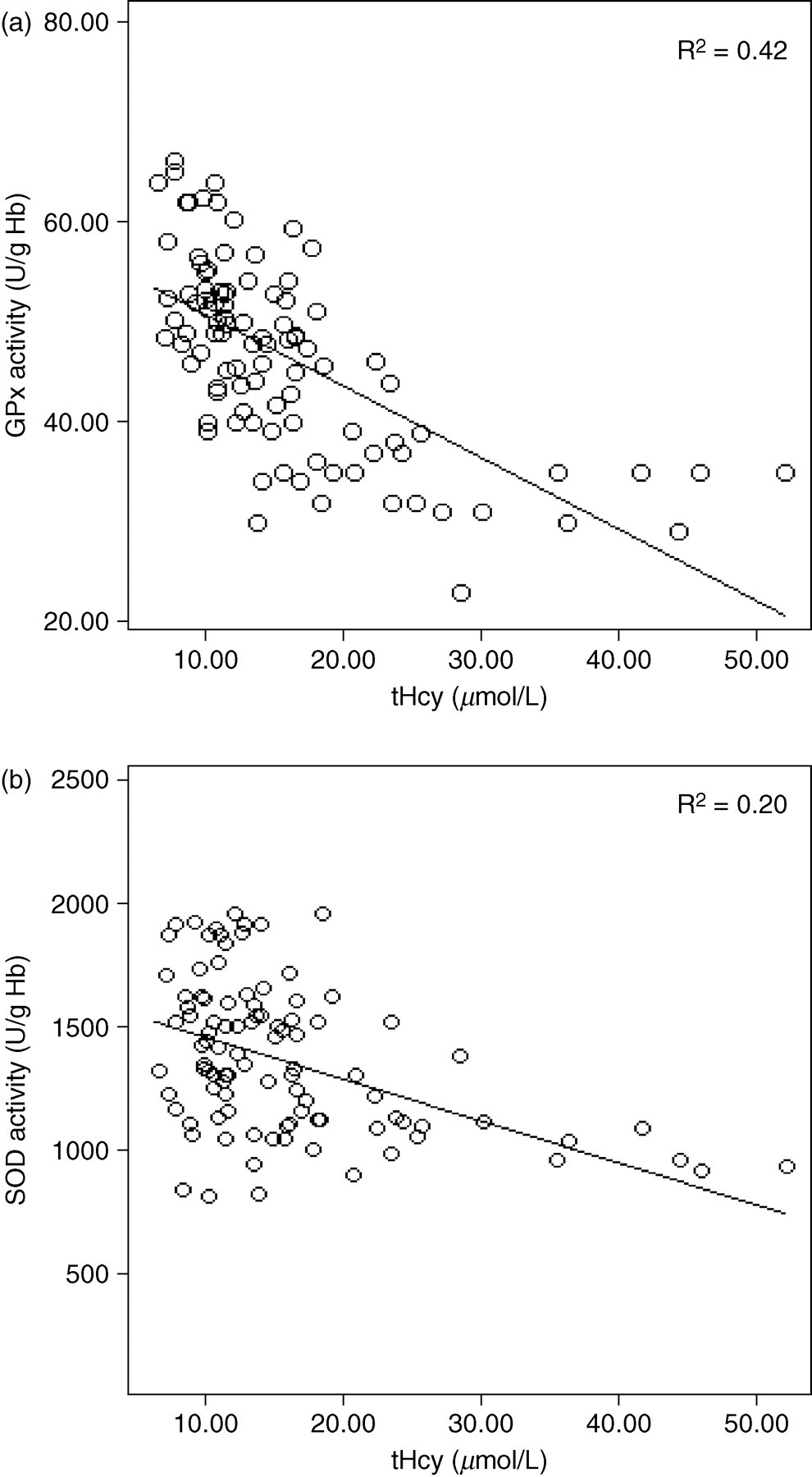
Correlation of plasma concentration of homocysteine with (a) glutathione peroxidase (GPx) activity and (b) superoxide dismutase (SOD) activity
Discussion
Several clinical studies have investigated antioxidative defence and shown that deficiency leads to CHD progression. 5,8,15,16 This study aimed to investigate the relationships between the antioxidative defence and the presence and severity of CHD. Our data revealed GPx, SOD activities and Zn concentrations in CHD patients to be significantly lower than those of control subjects. Patients with 3-vessel stenosis showed lower GPx, SOD activities than patients without stenosis (with 0-vessel stenosis). Whereas Nojiri et al. 15 reported that TAS decreased in CHD patients and it was significantly associated with the number of diseased vessels, we showed that there is no difference in TAS concentrations between CHD patients and healthy subjects, which is consistent with other studies. 22–25 Albumin, uric acid and bilirubin are known as major antioxidant components of plasma 26,27 and their concentrations are influenced by age, diet, heavy exercise, renal failure and some metabolic diseases. 26 Furthermore, Yegin et al. 28 revealed that there was a decrease in both the activity of GPx and erythrocyte selenium concentrations in parallel to the increase in the severity of CHD. Hyperhomocysteinaemia is associated with increased oxidative stress as well as decreased folate intake. Kerkeni et al. 2 have previously shown that homocysteine concentrations are related to folate with the more severe CHD patients having a reduced dietary intake and hence higher tHcy. The thiol group of homocysteine is readily oxidized in plasma to form ROS, suggesting a mechanism involving oxidative damage. 29 Some studies revealed that GPx expression and activity are impaired in cultured vascular endothelial cells treated with tHcy, which suggest that hyperhomocysteinaemia inhibits the antioxidant potentials of cells. 30–32 Hyperhomocysteinaemia increases vascular dysfunction in GPx deficient mice 33 and over-expression of GPx attenuates tHcy induced endothelial dysfunction. 34 Extracellular SOD has been reported to be a major antioxidant enzyme system of the arterial wall, located strategically between endothelium and vascular smooth muscle cells. The SOD concentration within the arterial wall is high enough to suppress pathological effects of superoxide anions such as reaction with nitric oxide (NO) leading to formation of deleterious peroxynitrite. Inhibition of vascular SOD resulted in impairment of endothelium dependent dilatation in bovine coronary arteries in vitro, suggesting that SOD concentrations are critical for the ability of NO to modulate vascular tone. 35 This concept finds further support from the in vivo observation that SOD deficiency impaired endothelium-dependent dilatation as the result of increased inactivation of NO. 36 Nihei et al. 37 reported that homocysteine may aggravate coronary atherosclerosis through its action on SOD enzyme. Homocysteine is involved in the significant release of extracellular SOD from the endothelium into the blood. We consider this to be one of the mechanisms by which oxidative stress could be increased by homocysteine, because extracellular SOD effectively removes superoxide near the endothelium by binding it to the endothelium. It has been established in animal 38,39 and human studies 40 that for effective functioning, SOD needs to be attached to the endothelium through its heparin-binding domain. We speculate that in vivo, hyperhomocysteinaemia may affect SOD activity. Yamamoto et al. 41 suggested that homocysteine decreased the binding of extracellular SOD to the vascular endothelial cell surface by degrading endothelial heparin sulphate proteoglycan and that the high concentration of tHcy decreased the production of SOD. Nonako et al. 42 also reported that homocysteine reduced the expression of SOD mRNA and protein concentrations in cultured rat smooth muscle cells.
The decreased antioxidant enzyme activities in this study may be due to a possible lowering of coenzyme Q10 in patients treated with statins. Statins (3-hydroxy-3-methylglutaryl coenzyme A reduced inhibitors) are widely used for treatment of hypercholesterolemia and CHD and for the prevention of stroke. Inhibition of cholesterol biosynthesis also inhibits the synthesis of coenzyme Q10, a ubiquitous fat-soluble, vitamin-like compound that functions as an electron carrier in the mitochondrial respiratory chain, as well as serving as an important intracellular antioxidant that protects phospholipids and mitochondrial membrane proteins from peroxidation, and protects DNA against the oxidative damage that accompanies lipid peroxidation. 43,44 Previous studies have shown that statins decreased coenzyme Q10. 45–47 Farswan et al. 46 found that administration of simvastatin and gemfibrozil produced significant decrease in the concentration of reduced glutathione, SOD, catalase and an increase in the concentration of lipid peroxidation.
Clinical studies indicate that Zn deficiency may predispose patients to diabetes mellitus, atherosclerosis and CHD. 18,48,49 In this study, we examined the association of Zn status with risk of CHD. We found decreased Zn concentrations in CHD patients compared with control subjects and Zn status therefore appears to be a risk factor for CHD.
In conclusion, the results of this study indicate that in CHD there is evidence of reduced activities of GPx, SOD, Zn concentration and increased tHcy which may be involved in the pathophysiology of this disease.
Footnotes
ACKNOWLEDGEMENTS
We thank Professor M Ben Farhat and his colleagues of the Cardiovascular Department at University Hospital Fattouma Bourguiba in Monastir (Tunisia) for providing samples and Dr S Yacoub and Dr M Zaier of the regional blood transfusion centre in Sousse (Tunisia) for recruiting the healthy subjects.