
Abstract
Abstract
We describe the case of a gentleman who initially presented with isolated cranial diabetes insipidus and has subsequently developed progressive anterior pituitary failure. In addition, he has been found to have evidence of mesenteric fibrosis and primary sclerosing cholangitis. We suggest that his pituitary disease may also be caused by progressive fibrosis and that these separate pathological entities may be linked by the unifying diagnosis of progressive multifocal fibrosclerosis, a rare fibro-inflammatory process involving multiple organ systems.
Case history
In October 1999, a 61-year-old gentleman was referred by his general practitioner to the medical outpatient clinic with a three-week history of sudden onset of polydipsia and polyuria. His urine output totalled more than 6 L in 24 h. His only medication at the time was cimetidine 400 mg daily, which had been prescribed following the diagnosis of a duodenal ulcer 10 years earlier. He had also previously suffered two episodes of meningitis many years earlier. At the age of eight the patient had developed meningitis and a brain abscess secondary to mastoiditis, which had necessitated neurosurgical intervention at that time. He had had a further episode of meningitis in his 20s, which had been attributed to non-paralytic poliomyelitis.
A water deprivation test was performed. Fluid restriction resulted in an increase in plasma osmolality. Immediately prior to the administration of desmopressin (DDAVP), plasma osmolality measured 308 mmol/kg, urine osmolality 273 mmol/kg and urine volumes measured in excess of 200 mL per hour. Following injection of DDAVP, the urine osmolality increased to 493 mmol/kg and the urine volumes reduced substantially. The results indicated a diagnosis of cranial diabetes insipidus. Assessment of anterior pituitary hormonal function was completely normal.
The precise cause of diabetes insipidus was unclear. A magnetic resonance imaging (MRI) scan of the pituitary gland showed no evidence of any mass lesion, however the scan was not normal. The pituitary enhanced uniformly with contrast and was noted to have a convex superior margin, and the pituitary infundibulum was enlarged. The appearances were suggestive of an inflammatory/infiltrative process (Figure 1). However, a chest X-ray showed no evidence of tuberculosis or sarcoidosis, the serum angiotensin converting enzyme (ACE) concentration was low and ferritin normal. Although the episodes of meningitis had occurred many years earlier, it was initially presumed that the development of cranial diabetes insipidus had occurred secondary to previous episodes of basal meningitis. He was commenced on DDAVP 100 µg four times daily, which resulted in complete resolution of his symptoms.
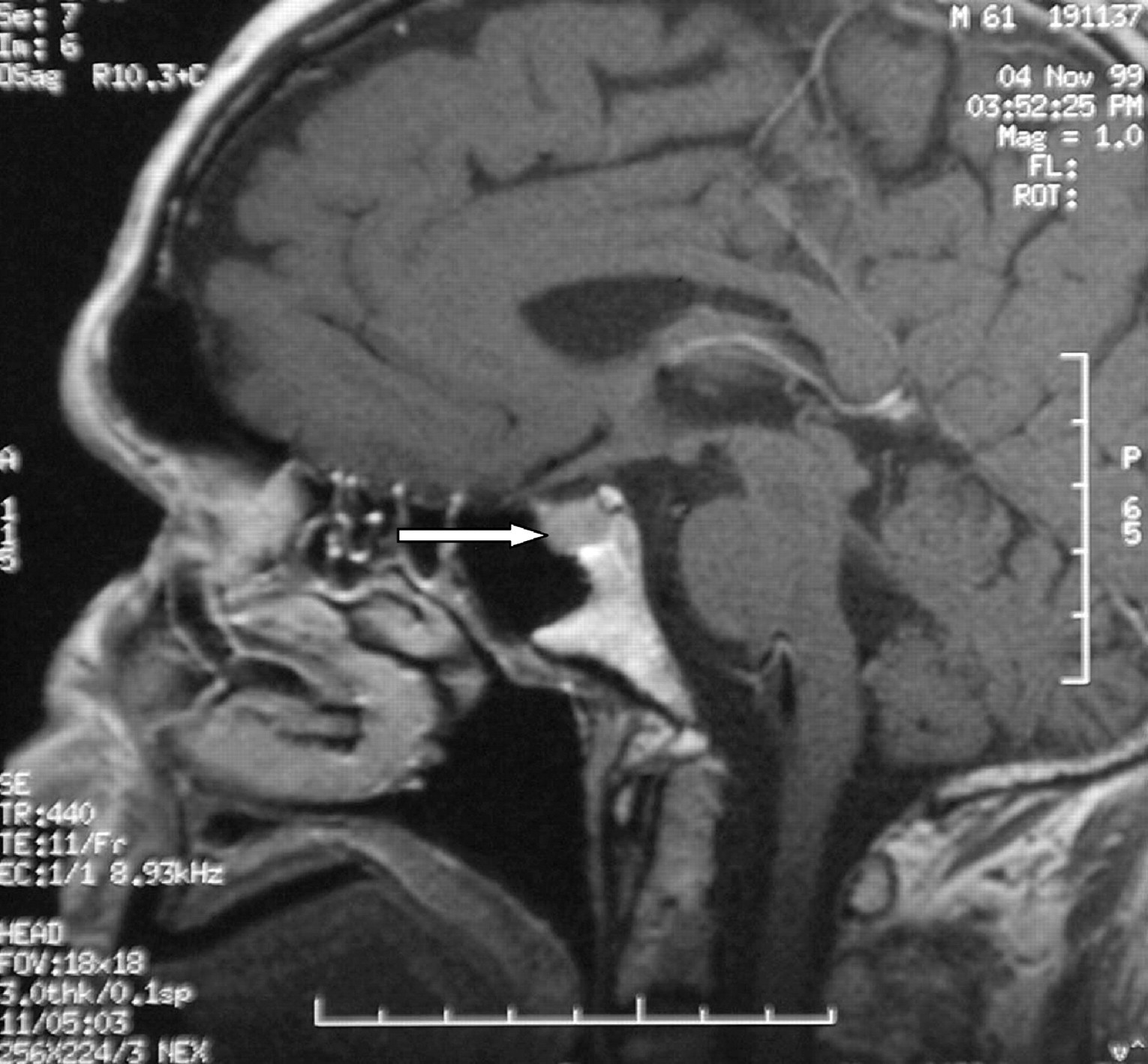
T1 weighted MRI scan of the pituitary gland following gadolinium contrast. The pituitary enhanced uniformly with contrast and was noted to have a convex superior margin, and the pituitary infundibulum was enlarged. The appearances were suggestive of an inflammatory/infiltrative process
In February 2001, he developed symptoms of episodic sweating and hot flushes. He also complained of erectile dysfunction, increased daytime somnolence and increased emotional lability. An early morning serum testosterone concentration was low (2.6 nmol/L). Although gonadotrophin concentrations were within the reference range, they were inappropriately low for the concentration of circulating testosterone (LH 2.0 U/L and FSH 4.0 U/L), giving a diagnosis of hypogonadotrophic hypogonadism. The rest of his anterior pituitary function remained normal, including thyroid function, serum IGF-1 concentration and response to a short synacthen test. Testosterone replacement therapy was commenced in the form of Sustanon injections every three weeks and, although some of his symptoms were not typical of hypoandrogenaemia, his symptoms generally improved. A repeat MRI scan of the pituitary gland remained unchanged from previously.
At the clinic review four months later, he continued to complain of increased lethargy and he had also gained 5 kg in weight. Thyroid function tests at that time showed a slightly low TSH (0.8 mU/L) and a reduced free thyroxine concentration (7 pmol/L). The total T3 concentration was within normal limits (2.2 nmol/L). The results suggested that he was developing secondary hypothyroidism and he was commenced on thyroxine replacement at a dose of 100
When reviewed in May 2004 he complained of malaise, nausea and anorexia, had lost 12 kg in weight in the preceding three months and was passing pale stools and dark urine. He was markedly icteric. Liver function tests showed an obstructive pattern with a bilirubin of 172
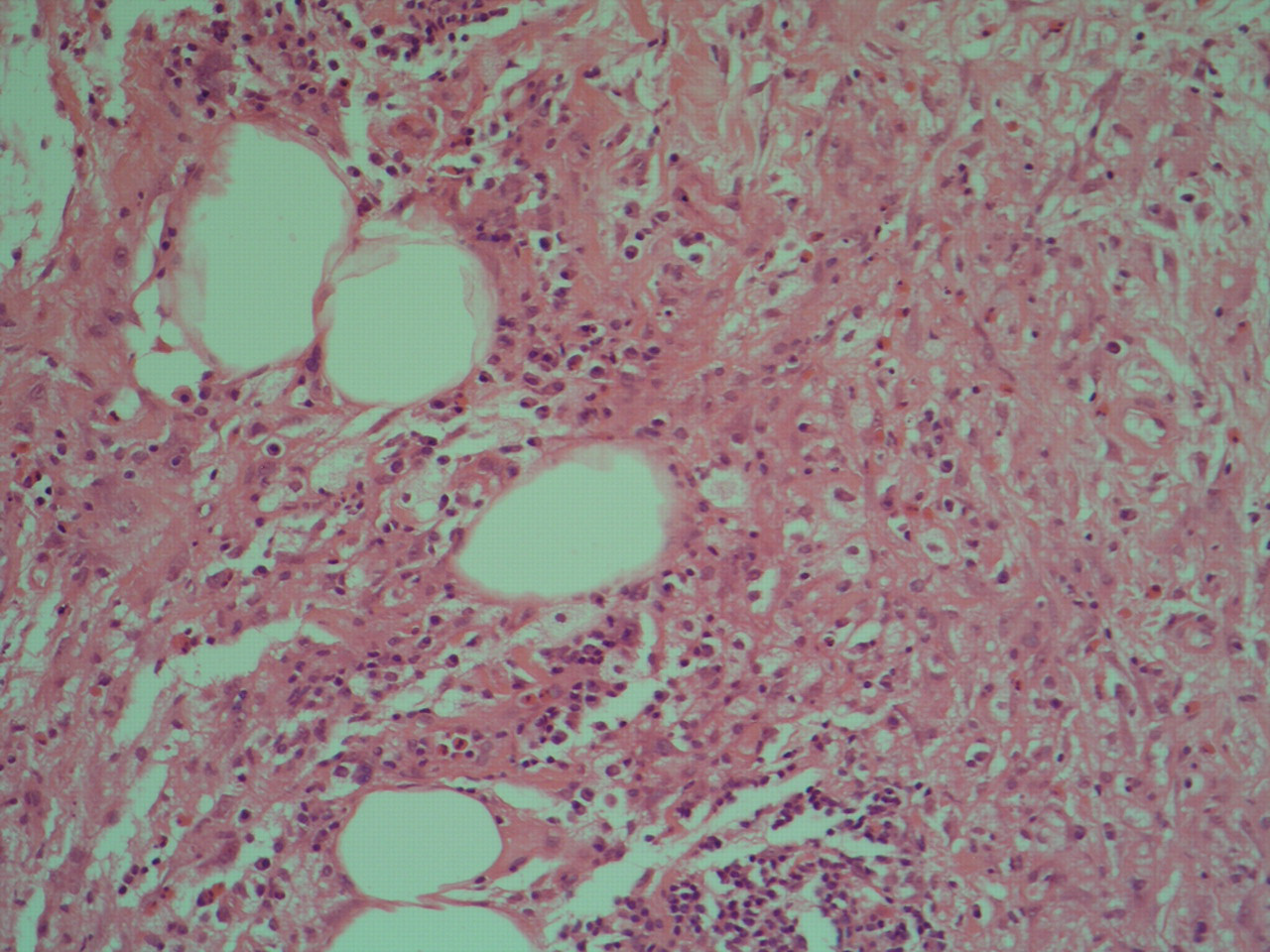
Peritoneal core biopsy showing fibrosis replacing peritoneal adipose tissue. Haematoxylin and eosin stain. ×40 magnification
In conjunction with the MRI appearances and the inability to identify any other cause of progressive pituitary dysfunction, it was presumed that the pituitary disease was the result of a progressive infiltrative/fibrotic process. The presence of fibrosis within other sites, in the form of primary sclerosing cholangitis and mesenteric fibrosis, suggests a unifying diagnosis of multifocal fibrosclerosis.
Discussion
Multifocal fibrosclerosis is a rare syndrome of unknown aetiology characterized by fibrosis involving multiple organ sites. The term multifocal fibrosclerosis was first described in 1967 by Comings
There is no definitive test to confirm the diagnosis. However, as well as multiple areas of disseminated fibrosis, common clinical findings include an elevated erythrocyte sedimentation rate (ESR), an increased white cell count with, in particular, an eosinophilia. Autoantibodies, such as rheumatoid factor, antinuclear antibody and antithyroid antibodies, are often present in high titre. Histology of the fibrotic lesion reveals fibrosclerosis with prominent hyalinizing collagen bundles and proliferation of myofibroblastic cells. 2 A lymphocytic infiltration and appearances of a vasculitis are also frequently present. CT and ultrasound scans reveal non-specific areas of fibrosis, and on T2 weighted MRI scanning, areas of multifocal fibrosclerosis appear as high signal intensity lesions, which enhance with gadolinium contrast on T1 weighted scans. Areas of multifocal fibrosclerosis can be clearly identified on F-18 fluorodeoxyglucose positron emission tomography, 3 with increased activity seen within lesions as a result of increased lymphocyte, plasma cell and fibroblast proliferation. In this particular case, T1 weighted MRI of the pituitary demonstrated uniform enhancement of the pituitary gland with gadolinium contrast, which is typical of the appearances seen in multifocal fibrosclerosis. Unfortunately, no attempt was made to obtain histological confirmation of the diagnosis by pituitary biopsy. We acknowledge that a definitive conclusion that the pituitary pathology was fibrosclerosis cannot be made without this.
Although the aetiology of multifocal fibrosclerosis is unknown, one theory of pathogenesis postulates that it results from an autoimmune process. This is supported by the pathological features of cellular infiltration, including lymphocytes and plasma cells, the frequent presence of focal vasculitis on pathological examination, and the favourable response of some patients with multifocal fibrosclerosis to treatment with systemic corticosteroids. The morbidity and mortality of multifocal fibrosclerosis is most frequently related to local extension and compression.
A variety of different treatment regimens are reported in the literature. Treatment with radiotherapy, surgery, cyclophosphamide and colchicine have all been recorded, often with limited success. Glucocorticoids are the current treatment of choice although the response to treatment is variable.
We report the case of a 61-year-old man with multifocal fibrosclerosis presenting with the combination of sclerosing cholangitis, mesenteric fibrosis, hypogonadotrophic hypogonadism and central diabetes insipidus. There are only two other cases in the literature of multifocal fibrosclerosis causing anterior pituitary insufficiency 4,5 and only one other case of multifocal fibrosclerosis causing central diabetes insipidus. 5 It is important that this diagnosis should be considered in any patient presenting with evidence of unexplained pituitary insufficiency and an infiltrative process involving other organs.