
Abstract
Background
Thyroid nodules are stratified through fine-needle aspiration (FNA) and are often categorized using The Bethesda System for Reporting Thyroid Cytopathology, which estimates the risk of malignancy for six cytopathological categories. The atypia of undetermined significance (AUS) and follicular lesion of undetermined significance (FLUS) categories have varying malignancy rates reported in the literature which can range from 6 to 72.9%. Due to this heterogeneity, we assessed the malignancy rate and effectiveness of repeat FNA (rFNA) for AUS/FLUS thyroid cytopathology at our institution.
Methods
Electronic health records of patients with AUS/FLUS thyroid cytopathology on FNA at our center since the implementation of the Bethesda System on May 1, 2014–December 31, 2019 were retrospectively reviewed. Patient demographics, treatment pathway, and pathology results were collected. The treatment pathway of the nodules, the rFNA results, and the malignant histopathology results were reported. Malignancy rates were calculated as an upper and lower limit estimate.
Results
This study described 182 AUS/FLUS thyroid nodules from 177 patients. In total, 24 thyroid nodules were deemed malignant upon histopathology, yielding a final malignancy rate of 13.2–25.3%. All of the malignancies were variants of papillary thyroid carcinoma. The malignancy rate of the nodules which underwent resection without rFNA (21.5%) was lower than the malignancy rate of the nodules which underwent resection after rFNA (43.8%). 45.5% of the rFNA results were re-classified into more definitive categories.
Conclusion
The malignancy rate of AUS/FLUS thyroid cytopathology at our center is in line with the risk of malignancy stated by the 2017 Bethesda System. However, our malignancy rate is lower than some other Canadian centers and approximately half of our rFNAs were re-classified, highlighting the importance of establishing center-specific malignancy and rFNA re-classification rates to guide treatment decisions.
Background
The incidence of thyroid cancer continues to increase in Canada and globally [1–4]. Palpation can detect a thyroid nodule in approximately 4% of the general population [1, 5], however ultrasonography can detect nodules in 19–67.6% of the population [1, 6–8]. Thyroid nodules have been reported in up to 64.6% of autopsies [1, 9]. The more frequent usage of advanced medical imaging has resulted in an increased number of thyroid nodules found incidentally, which is hypothesized to partially account for the increased incidence of thyroid cancer [1–4]. Despite this increased incidence, the prognosis of thyroid cancer remains highly favorable, with an overall five-year survival rate of 98% in Canada [2, 3].
Fine-needle aspiration (FNA) is a safe, accurate and cost-effective procedure used to assess thyroid cytopathology and risk of malignancy (ROM) [10]. The Bethesda System for Reporting Thyroid Cytopathology has reduced ambiguity surrounding thyroid FNA results, subsequently decreasing the rate of unnecessary thyroidectomies [11, 12]. The Bethesda System separates thyroid cytopathology into six categories and for each category, the “usual management” and ROM is provided [11]. The management of the atypia of undetermined significance/follicular lesion of undetermined significance (AUS/FLUS) category has been challenging due to its indeterminant nature and heterogeneous reports of malignancy rates [13, 14]. The original Bethesda System states a ROM of ∼ 5–15% for this category, and repeat FNA (rFNA) is recommended [11]. However, various institutions have reported widely ranging malignancy rates from 6 to 72.9% [13–16].
In 2016, histopathology of non-invasive encapsulated follicular variant of papillary thyroid carcinoma (NEFV-PTC) was re-classified as non-invasive follicular thyroid neoplasm with papillary-like nuclear features (NIFTP) to represent its indolent nature [17]. The updated 2017 Bethesda System states a 6–18% ROM for the AUS/FLUS category when NIFTP is not considered malignant, and a ∼ 10–30% ROM when NIFTP is considered malignant [18]. The 2017 Bethesda System recommends rFNA, molecular testing, or lobectomy for AUS/FLUS nodules [18].
Despite this update, there is heterogeneity in malignancy rates amongst Canadian centers and between centers in Canada and the United States [19–22]. Due to this lack of consensus, it is important to determine malignancy rates specific to populations of interest [19, 22, 23].
This study assesses the institution-specific malignancy rate and the effectiveness of rFNA for thyroid nodules with AUS/FLUS cytopathology at the Saint John Regional Hospital in Saint John, New Brunswick, the province's largest tertiary care centre with a catchment area serving a population of ∼ 170,000 [24, 25]. To the best of our knowledge this is the first study outlining AUS/FLUS thyroid cytopathology malignancy rate and treatment in New Brunswick, Canada. The results from our center add to the variable literature surrounding AUS/FLUS thyroid cytopathology and are discussed in relation to reported malignancy rates, specifically in a Canadian context.
Methods
Approval for retrospective data collection was obtained from the Horizon Health Network Research Ethics Board. All thyroid FNA results since the implementation of the Bethesda System in May 1, 2014–December 31, 2019 were screened, and all patients during this period who were ≥ 18 years old at the time of FNA and had AUS/FLUS thyroid cytopathology were included in the study.
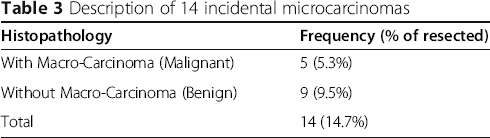
Electronic health records were retrospectively reviewed. The patients’ biological sex, age at the time of first AUS/FLUS cytopathology result, treatment pathway, and pathology results were collected. A nodule was deemed malignant or benign based on surgical histopathology only. Histopathology was correlated to the nodule targeted by FNA by associating the location and size of the nodule. A sub-centimeter microcarcinoma not targeted by the FNA and not found within a larger nodule targeted by FNA was defined as incidental. The presence of an incidental microcarcinoma was noted but deemed benign for the purpose of this study. NIFTP/NEFV-PTC histopathology was considered malignant in this study as the inclusion period pre-dated the 2016 nomenclature and classification adjustment [17].
FNA cytopathology and surgical histopathology were reviewed by in-house pathologists. A specialist in Head and Neck pathology external to our institution was consulted in challenging cases. Final treatment decision making was in collaboration between the patient and the treating physicians. Unless more concerning features were present, AUS/FLUS surgical patients were referred for lobectomy, and if a thyroid carcinoma was identified, contralateral completion thyroidectomy was recommended.
Data analysis
The proportion of all thyroid FNAs which were classified as AUS/FLUS was calculated. The treatment pathway of the AUS/FLUS thyroid nodules and the distribution of rFNA results were described as percentages. If multiple rFNAs were performed for the same nodule, the most definitive rFNA result was reported. The malignancy rate was calculated for the nodules which underwent immediate resection and those which underwent resection after rFNA. Finally, the distribution of malignant histopathology was calculated.
The final malignancy rate was calculated as an upper limit estimate (ULE) and a lower limit estimate (LLE), as described by Ho et al. [23]. The ULE was the malignancy rate of the resected nodules. The LLE was calculated under the assumption that all the unresected nodules were benign, and therefore was a malignancy rate of all AUS/FLUS cytopathology results.
Results
During our inclusion period 1130 thyroid FNAs were performed at our center, of which 205 (18.1%) yielded AUS/FLUS cytopathology, 23 of which were rFNA results of previously categorized AUS/FLUS nodules and thus were not included as separate nodules. A total of 182 thyroid nodules with AUS/FLUS cytopathology from 177 patients were included in this study. The patients had a mean age of 58.5 +/− 15.5 years at the time of the AUS/FLUS cytopathology result. The majority of the patients (74.6%, or n = 132) were female. 25.4% (n = 45) were male.
The treatment pathway of the AUS/FLUS thyroid nodules is described in Fig. 1. Of the 182 nodules, 44 (24.2%) underwent rFNA, 79 (43.4%) underwent resection, and 59 (32.4%) were followed clinically and had no further pathology results available. 16/44 (36.4%) of the nodules which underwent rFNA were resected, and 7/16 (43.8%) of these were malignant. In contrast, 17/79 (21.5%) of the nodules which were resected without rFNA were malignant. The majority of AUS/FLUS surgical patients (84.4%) underwent initial lobectomy.

Treatment pathway of the thyroid nodules with AUS/FLUS cytopathology at our center. Abbreviations: FNA – fine needle aspiration; AUS/FLUS – atypia of undetermined significance/follicular lesion of undetermined significance
In total 95/182 (52.2%) of the AUS/FLUS nodules were eventually resected, with 24/95 (25.3%) of these nodules yielding malignant histopathology, representing the ULE malignancy rate. 24/182 (13.2%), represents the LLE malignancy rate.
Results of the 44 rFNAs after initial AUS/FLUS cytopathology result

Abbreviations: AUS/FLUS atypia of undetermined significance/follicular lesion of undetermined significance, FN/SFN follicular neoplasm/suspicious for follicular neoplasm, SFM suspicious for malignancy
aPercent of frequency
bPercent of resected
Histopathology of 24 malignancies from thyroid nodules with AUS/FLUS cytopathology
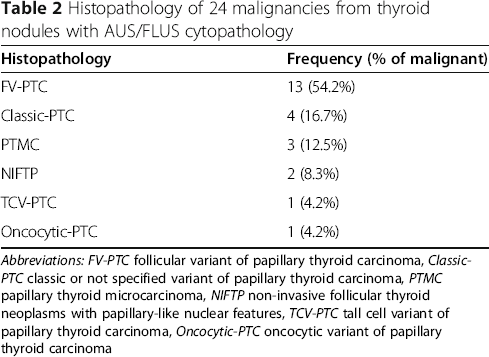
Abbreviations: FV-PTC follicular variant of papillary thyroid carcinoma, Classic-PTC classic or not specified variant of papillary thyroid carcinoma, PTMC papillary thyroid microcarcinoma, NIFTP non-invasive follicular thyroid neoplasms with papillary-like nuclear features, TCV-PTC tall cell variant of papillary thyroid carcinoma, Oncocytic-PTC oncocytic variant of papillary thyroid carcinoma
Description of 14 incidental microcarcinomas
Discussion
The Bethesda System for Reporting Thyroid Cytopathology effectively standardizes categorization of thyroid FNA results [12, 18]. However, the indeterminate nature of AUS/FLUS cytopathology has resulted in heterogeneous reports of malignancy rates for this category [13, 14]. The malignancy rate of AUS/FLUS thyroid cytopathology at our center is 13.2–25.3%.
Malignancy rate of AUS/FLUS thyroid cytopathology reported at various centers

Abbreviations: AUS/FLUS atypia of undetermined significance/follicular lesion of undetermined significance, LLE lower limit estimate, ULE upper limit estimate
aIncludes malignant/benign diagnosis based on histopathology, core needle biopsy, or rFNA
In terms of Canadian data, the malignancy rate seems to vary geographically. The largest Canadian series of AUS/FLUS thyroid cytopathology was conducted in an Ontario center and yielded a 37–46% malignancy rate [19], which is noticeably higher than our center. A study in Newfoundland also reported a higher LLE malignancy rate of 29.8% [20]. However, centers in Western Canada [21] and Nova Scotia [22] reported ULE malignancy rates of 32 and 24.7% respectively, which are similar to our study. Overall, our malignancy rate is within the lower end of those reported in the literature (Table 4).
These higher malignancy rates may suggest the need for further adjustment of the ROM stated in the 2017 Bethesda System. However, it is also possible that there is no generalizable ROM for this cytopathology [34]. Rather, center and population specific factors may account for the variability of malignancy rates [19, 22, 23]. For example, Ho et al., [23] noted their higher malignancy rate (26.6–37.8%) may be attributed to their high volume cancer center setting, potentially resulting in a referral bias of more concerning nodules. Conversely, Cavalheiro et al. [26] reported a 15.7% malignancy rate from a center where all AUS/FLUS thyroid nodules were surgically resected and Wu et al. [15] reported a 6% malignancy rate for FNAs from community practice settings. As shown in these studies, there is a wide variability in the malignancy rate for this cytological diagnosis, and this illustrates the importance and value of identifying the malignancy rate at ones’ own institution.
Our center had a high rate of AUS/FLUS diagnosis (18.1%) compared to the Bethesda recommendation of ≤10% [18]. The common “overuse” of the category and the greater inter−/intra-observer variability of AUS/FLUS diagnosis has been noted [13]. The other Canadian center with a similar malignancy rate to this study also reported a high AUS/FLUS rate (18.8%) [22], whereas the two Canadian centers with higher malignancy rates had lower AUS/FLUS rates (5.5 and 12.0% respectively) [19, 20]. This relationship is observed in many studies cited in Table 4, and it is likely that lower AUS/FLUS rates correspond to higher malignancy rates. It has been hypothesized that higher AUS/FLUS rates (> 15%) result in more benign or non-diagnostic cases categorized as AUS/FLUS, whereas lower rates (< 5%) are associated with reduced sensitivity [13, 35], which is important knowledge for clinical decision making.
The Bethesda System recommends lobectomy, rFNA, or molecular testing for AUS/FLUS cytopathology [18]. At our center, the malignancy rate of nodules resected after rFNA (43.8%) was noticeably higher than those proceeding directly to surgery (21.5%). This can likely be attributed to nodules re-classified in more concerning categories (FN/SFN and SFM) representing 43.8% of the resections after rFNA. In contrast, the majority of nodules re-classified by rFNA yielded benign cytopathology (25.0%) and only one was resected. This is in line with previous studies [31, 36], and demonstrates the potential for rFNA to facilitate management of nodules originally classified as AUS/FLUS. However, varying rFNA re-classification rates are reported amongst Canadian centers [36, 37], suggesting value in determining the institutional rFNA re-classification rates.
This study has some limitations. Due to its retrospective nature, 52.2% of the thyroid nodules with AUS/FLUS cytopathology underwent surgical resection, while the remaining nodules lacked histopathology results and were not definitively classified as benign or malignant. They were assumed to be benign when calculating the LLE malignancy rate, however it is possible they contained an indolent, malignant neoplasm. Also, the number of rFNAs which underwent resection is small and a larger sample size would be required to provide stronger conclusions for this sub-group. Finally, this study considered NIFTP/NEFV-PTC histopathology as malignant due to the inclusion period pre-dating our institution's implementation of the 2016 nomenclature change [17]. A future study comparing the malignancy rate pre and post implementation of NIFTP nomenclature at our center would be of interest.
Conclusion
The malignancy rate of thyroid nodules with AUS/FLUS cytopathology at our center is 13.2–25.3%. Our malignancy rate is in line with the ROM stated by the Bethesda System (∼ 10–30%) [18]. Repeat FNA was helpful in re-classifying nearly 50% of the nodules that were biopsied and remains a useful technique in triaging these nodules. This study highlights the importance of establishing center-specific malignancy and rFNA re-classification rates to guide treatment decisions.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
KH completed data collection and drafted the manuscript. TR, VM, and CJC designed the study, assisted in interpreting the results, and helped prepare and revise the manuscript. VN and AS facilitated data collection and helped revise the manuscript. All authors read and approved the final manuscript.
Funding
No funding was received for this study.
Availability of data and materials
The datasets used and analysed during the current study are available from the corresponding author upon reasonable request and approval from the Horizon Health Network Privacy Officer.
Declarations
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.