
Abstract
Importance
Several feasible management options exist for indeterminate thyroid nodules (ITNs), which can lead to decisional conflict (DC) and uncertainty in patients.
Objective
To investigate patient and physician participation in shared decision-making (SDM) during the management of ITNs and the association of SDM with patient-perceived DC.
Study Design
Multi-institutional, cross-sectional, multiple methods study.
Setting
The Queen Elizabeth II Health Science Centre (Halifax, Nova Scotia) from October 2020 to June 2023 and The Ottawa Hospital (Ottawa, Ontario) from November 2022 to June 2023.
Intervention and Exposures
Patients with ITNs scheduled for an initial surgical consultation with an Otolaryngologist were included. Consultations were video-recorded using discreet cameras within clinic rooms at both sites. Management options discussed at both sites included repeat fine needle aspiration biopsy, ultrasound surveillance, surgery, and molecular testing.
Main Outcome Measures
Patient-perceived SDM was measured by the SDM Questionnaire-9 (SDM-Q-9) and perceived DC by the DC Scale (DCS). Surgeons’ perceptions of SDM were measured by the SDM-Q-Doc. Observer-determined SDM was reported using the multifocal approach to sharing in SDM (MAPPIN’SDM) instrument.
Results
Seventy-seven patients and 6 surgeons were included. Patient-perceived SDM was high [mean = 94.38, standard deviation (SD) = 7.61], while physician-perceived SDM was lower in comparison (mean = 83.21, SD = 9.14). Observer-determined SDM involvement of the patient (mean = 0.73, SD = 1.08), physician (mean = 1.71, SD = 1.33), and patient-physician dyad (mean = 1.75, SD = 1.27) was low. Clinically significant DC (DCS score ≥25) was reported by 13.2% of patients. There was a medium negative correlation between patient-perceived SDM involvement and DC (Pearson r = −0.311, P = 0.008). Patient-perceived SDM did not differ by clinicodemographic factors.
Conclusion
While patients and physicians perceived high levels of SDM, patients with ITNs are faced with difficult management decisions leading to DC.
Relevance
These findings highlight the need for developing decision-aids to support SDM and reduce DC in the management of ITNs.
Key Messages
Perceived shared decision-making (SDM) during initial consultations for indeterminate thyroid nodules (ITNs) is high; however, objective evidence for such remains low.
Despite high perceptions of SDM, clinically significant decisional conflict persists.
No decision-aids currently exist to support SDM during management discussions for ITNs.
Introduction
Thyroid nodules are common, present in over 60% of the population. 1 Despite thyroid carcinoma being the seventh most common cancer globally, 2 a large proportion of thyroid nodules are found incidentally in asymptomatic patients and represent benign disease.1,3,4 Determining which nodules are clinically relevant poses a challenge to both clinicians and their patients.
The Bethesda System for Reporting Thyroid Cytopathology classifies biopsy results into 1 of 6 cytopathologic categories, of which clear management algorithms exist for cytologically benign nodules, and those that are either suspicious for malignancy, or malignant. Conversely, nodules showing atypia of undetermined significance (AUS, Bethesda-III) or follicular neoplasm (FN, Bethesda-IV) are considered indeterminate in their risk for malignancy, with rates of 13% to 30% and 23% to 34%, respectively. 5 This suggests that most indeterminate nodules are benign.5,6
Due to the uncertain risk of malignancy in Bethesda-III/Bethesda-IV thyroid nodules, management guidelines released by the American Thyroid Association have allowed for repeat fine needle aspiration (FNA) biopsy, diagnostic hemithyroidectomy, ultrasonographic surveillance, or molecular diagnostic testing. 7 Physicians and patients are faced with a difficult decision following the diagnosis of AUS/FN, which has been shown to cause significant decisional conflict (DC) and uncertainty in patients. 8 Shared decision-making (SDM) is an approach that encourages patient and physician involvement in medical decision-making. 9 SDM is especially important in situations where multiple treatment options are feasible, such as with indeterminate thyroid nodules (ITNs). Patient-perceived SDM improves trust, satisfaction, and understanding while reducing DC. 8
Suboptimal involvement of patients and their physicians in discussions where there is clinical equipoise may generate further DC. Determining whether SDM is performed in the setting of ITNs may help identify the need for future interventions to support the decision-making process. The purpose of this study was to investigate perceived and objective SDM involvement in patients with ITNs during their initial consultation with an Otolaryngologist—Head and Neck Surgeon, and to evaluate the relationship between these outcomes and perceived DC.
Materials and Methods
Design
This was a multi-institutional, cross-sectional, multiple methods study. Ethics approval was obtained through the Nova Scotia Health Research Ethics Board (1025283) and the Ottawa Health Science Network Research Ethics Board (20220367-01H).
Participants
Adult patients (>18 years) with Bethesda-III or Bethesda-IV thyroid nodules scheduled for an initial surgical consultation with an Otolaryngologist—Head and Neck Surgeon at the Queen Elizabeth II Health Science Centre (Halifax, Nova Scotia) from October 2020 to June 2023 and The Ottawa Hospital (Ottawa, Ontario) from November 2022 to June 2023 were eligible to participate. Patients who had prior discussions with non-surgical specialists (eg, primary care practitioner, endocrinologist) regarding ITN management were included in the study. Patients were excluded if they had insufficient English language proficiency or previously resected ITNs. Clinicians fellowship-trained in head and neck surgical oncology were eligible to participate.
Study Procedure
A research associate outside of care obtained informed consent from study participants prior to consultations. Consultations were video-recorded using discreet cameras within clinic rooms at both sites. Management options discussed at both sites included repeat FNA biopsy, ultrasound surveillance, surgery, and molecular testing. Video equipment was positioned to ensure both video and audio capture of both the patient and the physician. Patients completed the SDM Questionnaire-9 (SDM-Q-9) and DC Scale (DCS) immediately following the consultation. Surgeons completed the SDM-Q-Doc after the consultation. Patient-physician interactions were analyzed using the multifocal approach to sharing in SDM (MAPPIN’SDM) instrument.
Outcomes
Primary outcomes
The primary outcomes of this study were to determine the degree to which SDM occurred during consultations for ITNs, and to explore clinicodemographic factors associated with SDM performance. SDM was defined by the SDM-Q-9 and SDM-Q-Doc.
Secondary outcomes
Secondary outcomes of this study were to assess observer-determined SDM and to examine the relationship between patient-reported perceptions of the SDM process and DC. As no observer-based instrument has previously been validated within this specific setting, we also sought to assess the psychometric properties of the MAPPIN’SDM instrument.
Measures
Demographics
Clinicodemographic information was reported by patients (Table 1). Participants were permitted to leave answers blank at their discretion (Supplemental Figure 1).
Patient Clinicodemographic Characteristics.

Abbreviation: SD, standard deviation.
One patient had both Bethesda III and IV nodules, therefore, was categorized as Bethesda IV.
SDM-Q-9—Patient
The SDM-Q-9 is a 9-item self-report questionnaire that assesses patient perceptions of SDM 10 and has demonstrated high internal reliability. 11 Items are rated on a 6-point Likert scale from “completely disagree” (0) to “completely agree” (5), with higher scores representing higher patient-perceived SDM involvement. Example of an item: “My doctor and I selected a treatment option together.”
SDM-Q-9-Doc—Physician
The SDM-Q-9-Doc is a 9-item self-report questionnaire that assesses physician perceptions of SDM 10 and is well-accepted and reliable. 12 Items are rated on a 6-point Likert scale from “completely disagree” (0) to “completely agree” (5), with higher scores representing higher physician-perceived SDM involvement. Example of an item: “My patient and I selected a treatment option together.”
DC Scale
The DCS is a 16-item self-report questionnaire that evaluates the construct of DC 13 and has demonstrated satisfactory reliability and validity.14 -16 Items are rated on a 5-point Likert scale from “strongly agree” (0) to “strongly disagree” (4), with higher scores representing higher levels of DC. DCS scores of ≥25 are considered clinically significant.17 -21 Example of an item: “I know which options are available to me.”
Multifocal approach to sharing in SDM
The MAPPIN’SDM is an 11-item instrument that assesses observer-determined SDM involvement of the patient, physician, and patient-physician dyad 22 and has demonstrated adequate reliability and validity in other settings. 23 Items are rated on a 5-point Likert scale from “the behavior is not observed” (0) to “the behavior is observed to an excellent standard” (4), with higher scores representing higher observed SDM. Three variations of each item exist to account for the 3 individual subdomains (patient, physician, and patient-physician dyad). Example of 1 item (physician subdomain): “The clinician draws attention to an identified problem as one that requires a decision-making process.” The MAPPIN’SDM was scored by V.T., trained in SDM. Considering the subjectivity of assessing SDM, a subset of 15 video-recorded consultations were independently scored by a second coder trained in SDM (C.H.) to assess inter-rater reliability.
Observing Patient Involvement Instrument-5
Convergent validity requires a comparative gold standard. While no such standard exists for SDM, the Observing Patient Involvement Instrument-5 (OPTION-5) measures a similar construct to physician involvement as assessed by the MAPPIN’SDM and was therefore utilized to assess convergent validity. The OPTION-5 is a 5-item instrument that assesses SDM during patient-physician encounters24,25 and has demonstrated acceptable reliability and validity. 24 Items are rated on a 5-point Likert scale from “no effort” (0) to “exemplary effort” (4), with higher scores representing higher observed SDM. Example of an item: “The clinician gives information or checks understanding about the options.” The OPTION-5 was scored by V.T. on a subset of recorded interactions.
Data Analysis
Data analysis was performed using SPSS Version 28 (IBM Corp., Armonk, NY). Demographics were analyzed using univariate descriptive statistics. Age and nodule size were continuous variables. The remaining demographic variables were categorical. Ethnicity was operationalized as White and non-White. Descriptive statistics including mean and standard deviation (SD) of SDM-Q-9, SDM-Q-9-Doc, DCS, MAPPIN’SDM, and OPTION-5 were calculated. Missing data was infrequent and excluded from analysis.
To explore the associations between clinicodemographic factors and patient-perceived SDM involvement, a generalized linear multivariable model was developed. Assumptions were verified, including absence of multicollinearity and overspecification.
Previous research has demonstrated that a difference of 0.5 SDs in health measurement scales represents clinically significant change, and SD differences of 15 points are expected for SDM-Q-9/SDM-Q-Doc scores.26,27 Therefore, a sample of at least 148 (74 patients, 74 clinician encounters) is required to provide a 2-sample 2-sided t-test with 80% power at alpha = .05 to detect a difference of a half SD between the 2 groups, assuming a SD of 15.
Psychometric Evaluation
Reliability
Inter-rater and intra-rater reliability were assessed. The time period between intra-rater reliability was 9 months. Fifteen of 74 videos were scored for assessment of both intra-rater and inter-rater reliability. The inter-rater reliability was determined by comparing MAPPIN’SDM scored by C.H. to its scoring by V.T.
Intra-rater and inter-rater reliability of the MAPPIN’SDM were analyzed using intraclass correlations (ICC) with a 2-way mixed effects model with absolute agreement and a 2-way random effects model with consistency agreement, respectively. 28 ICC were calculated separately using mean values across the 9 items of the individual MAPPIN’SDM scales (patient, clinician, dyad) as well as collectively using mean values of the individual scale totals. 28
Validity
Multiple forms of validity were assessed for the MAPPIN’SDM in our setting. Construct validity has previously been assessed during the original development process of the MAPPIN’SDM. We therefore utilized similar hypotheses; there would be (1) limited congruence between measurement perspectives, (2) a positive correlation between physician and patient SDM activity, (3) a reduced correlation between physician and dyad with higher patient activity, and (4) high within-party correlations for the items equipoise (item-2), communication of risks (item-3b), and agreeing on a decision (item-5). Mean scores were used to evaluate correlations between physician and patient SDM activity. Mean and median scores were used to assess correlations between physician and dyad with higher patient activity. A median score of ≥1 and 0 were used to define high and low patient activity, respectively. Spearman’s rank correlation coefficients were obtained. MAPPIN’SDM clinician means were used to assess convergent validity between the OPTION-5 and MAPPIN’SDM.
Results
Participant Demographics
In total, 77 patients were enrolled in the study (Table 1). The mean age of participants was 55.7 years (SD = 15.9), and most patients were female (59.7%). Bethesda-III nodules were more common (92.2%) compared to Bethesda-IV nodules (7.8%). Twenty-nine (36.6%) patients decided on surgery, 35 (45.5%) for surveillance, 10 (13.0%) for repeat FNA biopsy, and none (0%) decided on molecular testing. Among the 6 participants with Bethesda-IV thyroid nodules, 5 (83.3%) decided on surgery, and 1 (16.7%) for repeat biopsy. Overall, 6 clinicians (4 = Halifax site, 2 = Ottawa site) were included in the study. Most clinicians were male (83.3%), and 1 was female (16.7%).
Primary Outcome
Patient- and physician-perceived shared decision-making
Patient-perceived participation in SDM was high, with a mean SDM-Q-9 score of 94.38 (SD = 7.61) and 38 (51.4%) patients reporting maximum scores. Physician-perceived participation in SDM was lower in comparison but overall remained high, with a mean SDM-Q-Doc score of 83.21 (SD = 9.13) and physicians reported maximum scores for only 8 (10.8%) patient interactions (Table 2).
Outcomes of Shared Decision-Making and Decisional Conflict.
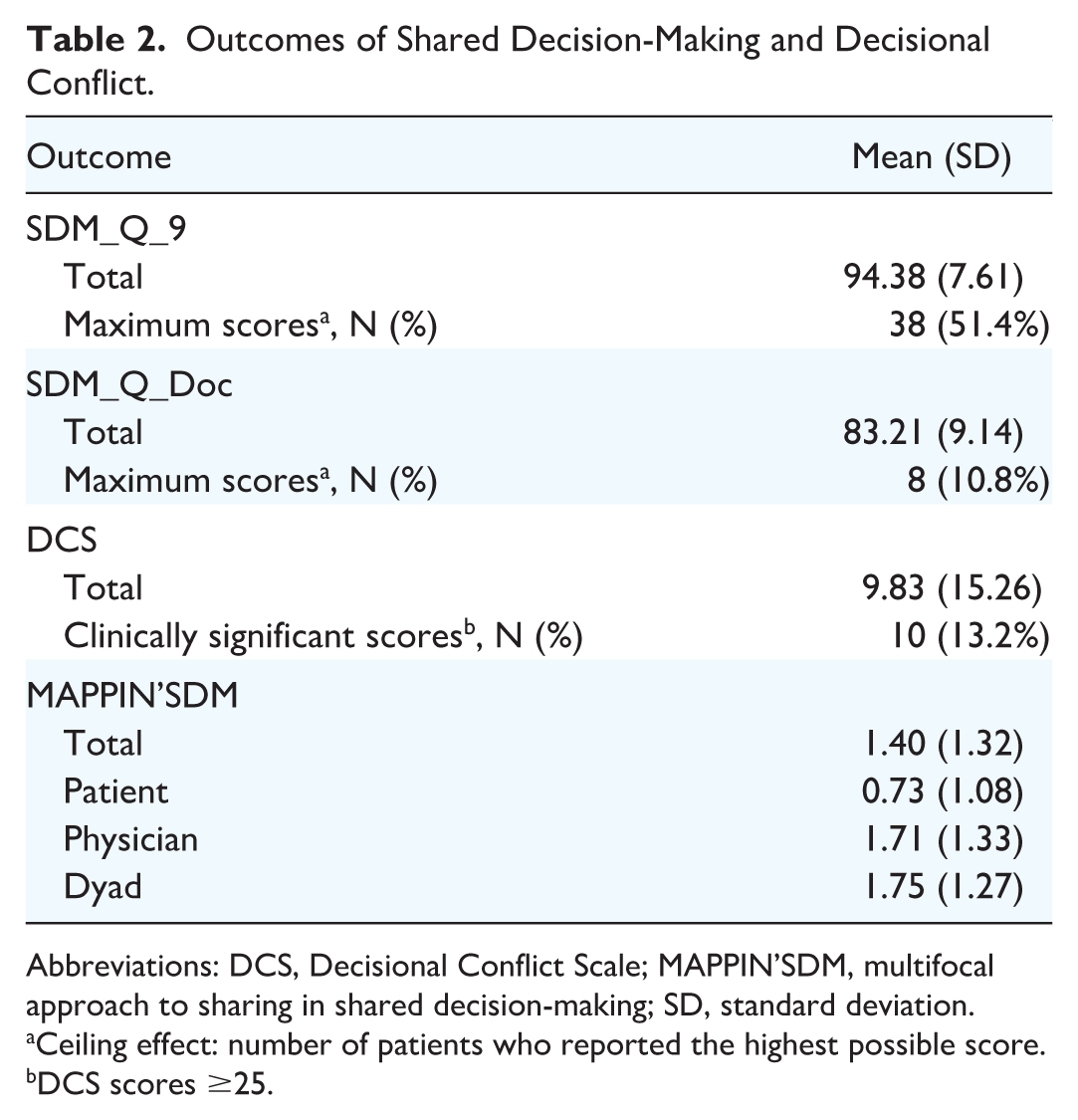
Abbreviations: DCS, Decisional Conflict Scale; MAPPIN’SDM, multifocal approach to sharing in shared decision-making; SD, standard deviation.
Ceiling effect: number of patients who reported the highest possible score.
DCS scores ≥25.
Factors associated with perceptions of SDM
Patient-perceived SDM did not differ by demographic-related variables, including age (Pearson r = −0.208, P = 0.861), sex (mean difference = 0.720, P = 0.70), education (F(3,67) = 0.512, P = 0.675), ethnicity (mean difference = 0.684, P = 0.81), or income (F(7,63) = 0.896, P = 0.515). Similarly, system-level variables did not affect the perception of SDM involvement by patients, including surgeon (F(5,65) = 1.417, P = 0.230) or site (mean difference = 1.92, P = 0.531). There was a small negative correlation between nodule size and SDM-Q-9 score (Pearson r = −0.264, P = 0.026). These results were similar during exploratory multivariable analysis, with no demographic- or system-level variables showing an association with SDM-Q-9 scores. That is, the model itself did not offer additional predictive value over univariate statistics (Omnibus test >0.05).
Secondary Outcomes
Observer-determined SDM
In total, 74 participants consented to the video-recorded portion of the study. Observer-determined SDM involvement of the patient (mean = 0.73, SD = 1.08), physician (mean = 1.71, SD = 1.33), and patient-physician dyad (mean = 1.75, SD = 1.27) was low (Table 2). Patients scored highest on item-4 (expectations and worries) and lowest on item-1 (defining the problem). Physicians and patient-physician dyads both scored highest on item-1 and lowest on item-7 (preferred communication approach).
Decisional conflict
DCS mean was 9.83 (SD = 15.26; Table 2) and clinically significant DC (DCS scores ≥25) was reported by 10 (13.2%) patients. There was a medium negative correlation between patient-perceived SDM involvement and reported DC (Pearson r = −0.311, P = 0.008).
Psychometrics
Reliability
Intra-rater reliability of the MAPPIN’SDM as a whole was excellent (ICC = 0.974, 95% CI = 0.926-0.991). Inter-rater reliability of the MAPPIN’SDM was moderate but ranged from poor to excellent (ICC = 0.7, 95% CI = 0.073-0.900). Individual subdomain (patient, clinician, and dyad) intra-rater reliability was excellent, while inter-rater reliability was poor to excellent (Supplemental Table 1). Internal consistency of the MAPPIN’SDM was adequate with Cronbach’s alpha for clinician, patient, and dyad subscales of 0.780, 0.751, and 0.781, respectively (Table 3).
Frequencies of MAPPIN’SDM Patient, Physician, and Dyad Item Scores.
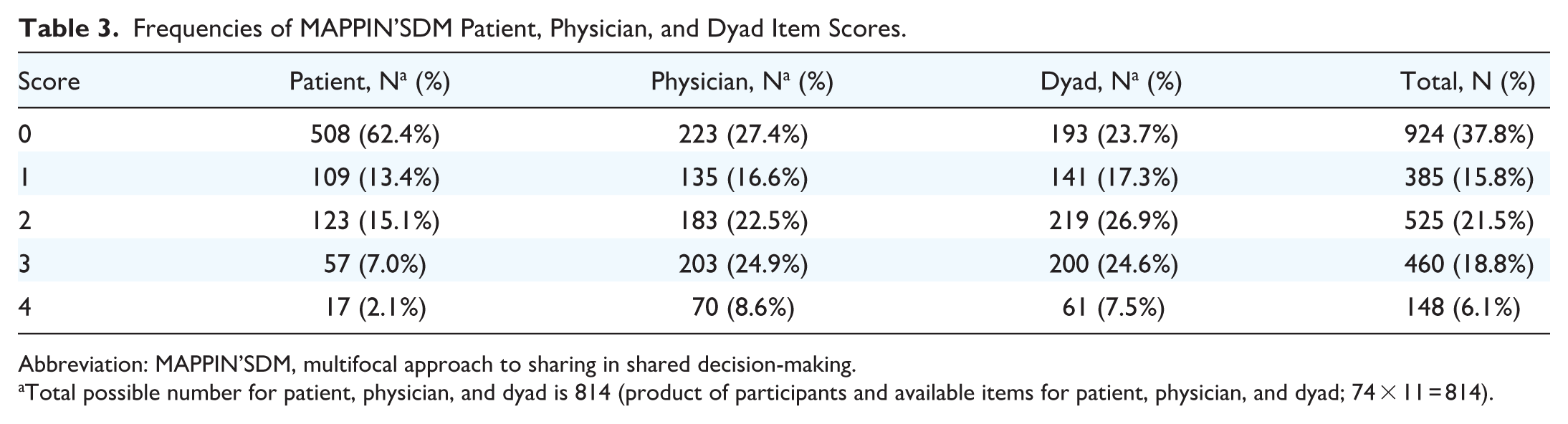
Abbreviation: MAPPIN’SDM, multifocal approach to sharing in shared decision-making.
Total possible number for patient, physician, and dyad is 814 (product of participants and available items for patient, physician, and dyad; 74 × 11 = 814).
Construct validity
Limited congruence was noted between measurement perspectives (patient, physician, and dyad). The correlation between physician and patient SDM activity was positive and of moderate strength (r = 0.479, P < .001). When patient activity was low (median score = 0), the correlation between clinician median and dyad median was strong (r = 0.815, P < .001). When patient activity was high (median score ≥1), the correlation between clinician median and dyad median was reduced (r = 0.725, P = 0.18). There were low within-party correlations for equipoise, communication of risks, and agreeing on a decision. Therefore, of our 4 a priori hypotheses—(1) limited congruence between measurement perspectives; (2) positive correlation between physician and patient SDM; (3) reduced correlation between physician and dyad with higher patient activity; and (4) high within-party correlations for items 2, 3b, and 5—3 were found to be true (1-3).
Convergent validity
Moderate convergence was noted between measurement instruments used to assess physician involvement in SDM. The correlation between the OPTION-5 and MAPPIN’SDM was r = 0.588 (P = .021), when using MAPPIN’SDM clinician mean values (Supplemental Table 2).
Discussion
Several feasible management options exist for ITNs. Clinical equipoise in these scenarios results in challenging decisions for patients and their physicians. 29 This is the first study to investigate both perceived and objective SDM involvement for ITNs and to validate the MAPPIN’SDM as an observer-based tool in this context. Perceived SDM was high for both patients and physicians, yet objective SDM was low. Despite overall low levels of DC experienced by patients, there is a subset of patients that still struggle.
Although self-reported measures (SDM-Q-9/SDM-Q-Doc) capture satisfaction with the SDM process, they may not reflect the overall quality of SDM behaviors during healthcare interactions30,31—an area targetable for future improvement. While patient satisfaction is important, high self-report scores may not adequately reflect the complexity of SDM, including whether important information required for informed decision-making was discussed. Future researchers may therefore consider integrating both subjective and objective data for a more accurate evaluation of SDM.
Perceptions of SDM were higher in patients compared to physicians, likely due to better clinician knowledge on judging SDM performance. These findings are consistent with the literature. For example, a recent study involving 42 patients with non-cutaneous head and neck cancers found that both patients and surgeons reported relatively high perceived SDM scores, while observer-based scores were moderate in comparison. 32 In our study, post hoc analyses found no associations between DC and physician-perceived nor observer-determined SDM, suggesting that patient-experienced DC is more dependent on patient-perceived SDM. No associations were found between perceptions of SDM and age, sex, education level, ethnicity, income, or attending surgeon. There is, however, evidence in the literature that significant variations in management decisions exist for ITNs, including as a function of individual surgeons. 33 This may not be represented in our study considering interactions were video-recorded. Video-recorded interactions increase understanding about communication during clinical encounters;34,35 however, the awareness of being recorded may modify patient and physician behavior during clinical interactions (Hawthorne effect). 36 Importantly, analyses of associations were exploratory in nature; therefore, larger studies are required for validation.
In this study, 13% of patients experienced clinically significant DC. In a study involving 35 patients, one-third experienced clinically significant DC when deciding between management options for ITNs. 8 Similarly, the current study found that higher levels of perceived SDM involvement are associated with lower levels of DC, suggesting that patients who feel actively engaged in their healthcare decisions experience less uncertainty about their treatment decision. 37 Importantly, to encourage patient participation in decision-making, an effective physician-patient relationship is required. 38 This exemplifies the need to optimize SDM when multiple feasible treatment options exist, including ITNs.
This is the first study to validate the MAPPIN’SDM in the context of ITNs. The MAPPIN’SDM demonstrated adequate reliability and validity, showing its appropriate use in this setting and future research, while further adding to the evidence collected from other clinical scenarios. 23 This is one of few studies that has assessed both intra- and inter-rater reliability, which were found to be excellent and moderate, respectively. Although the MAPPIN’SDM requires training with a standardized manual, scoring may still differ between coders due to differences in interpretation of communication behaviors or variability in clinical experience with decision-making in this context. The results of this study could be strengthened with more trained observers.
The MAPPIN’SDM demonstrated that physicians and patient-physician dyads both scored highest on “defining the problem”; conversely, patients scored lowest on this item. This is understandable considering patients are often unaware of their diagnosis prior to the initial surgical consultation, and management discussions are ultimately guided by FNA biopsy results that have not yet been disclosed. Patients scored highest on “describing expectations and concerns,” which may reflect the high levels of patient-reported DC. Physicians and patient-physician dyads both scored lowest on “choosing a preferred communication approach—visual aids, written information, or involving another family member in the discussion.” This may reflect physician time constraints or simply the lack of decisional tools that exist for patients in the context of ITNs.
This study has several limitations. Patient-perceived SDM measurements endured ceiling effects, which made differentiation challenging and may explain the limited small association found between higher perceived SDM and lower DC. Physician-patient interactions occasionally preceded discussions with other healthcare team members (eg, surgical resident/fellow), potentially introducing variation into the healthcare experience. Additionally, patient-physician consultation lengths varied between clinicians, ranging from 5 to 30 minutes; longer interactions may permit more comprehensive management discussions. Importantly, although offered to all patients, molecular testing is not publicly funded in Canada, which may reflect its poor uptake in this study.
Elective surgeries were postponed at both sites during the COVID-19 pandemic, resulting in longer wait times for diagnostic hemithyroidectomies. This may have influenced participants’ decisions, considering surgeons were often able to see patients sooner with ultrasound surveillance compared to surgery. One study found that during the pandemic there was a significant reduction in surgeries for ITNs, along with an increased occurrence of aggressive thyroid tumors. 39 Although most ITNs are benign, this suggests there may be a malignant transformational potential not accounted for.
A recent study by Scappaticcio et al highlights the complexity of decision-making in the setting of ITNs, emphasizing the incorporation of patient-specific factors, individual preferences, and nodal size in the SDM process. 40 Several barriers to incorporating SDM into clinical practice exist.41,42 Decision-aids may support SDM during medical decisions, as they have been shown to decrease DC and increase patient-perceived involvement in decision-making. 43 Currently, no decision-aids exist specifically for the management of ITNs. However, decision tools have proven to be helpful in the setting of thyroid nodules, prior to a cytological diagnosis. A pilot study evaluating the use of a web-based conversation aid to support SDM between patients with thyroid nodules and their physicians found significant improvements in observed SDM, and the decision tool was well-accepted.44 -46 Decision-aids also exist for the management of low-risk thyroid cancer, and have been found to increase patient involvement and clinical satisfaction, decrease DC, and improve medical knowledge.47,48
Conclusion
Patients and physicians perceive themselves to be highly involved in the SDM process for the management of ITNs. However, many patients continue to experience clinically significant DC. To optimize SDM and alleviate DC for patients with ITNs, there is a need for decisional tools to assist during the decision-making process. This study creates a path for further exploration of patient and physician needs where clinical equipoise exists.
Supplemental Material
sj-docx-1-ohn-10.1177_19160216251407670 – Supplemental material for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules
Supplemental material, sj-docx-1-ohn-10.1177_19160216251407670 for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules by Victoria Taylor, Travis Pickett, Brooke Turner, Claire Hermiston, Tara Azad, David P. Goldstein, Matthew H. Rigby, Stephanie Johnson-Obaseki, Martin Corsten and David Forner in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-docx-2-ohn-10.1177_19160216251407670 – Supplemental material for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules
Supplemental material, sj-docx-2-ohn-10.1177_19160216251407670 for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules by Victoria Taylor, Travis Pickett, Brooke Turner, Claire Hermiston, Tara Azad, David P. Goldstein, Matthew H. Rigby, Stephanie Johnson-Obaseki, Martin Corsten and David Forner in Journal of Otolaryngology - Head & Neck Surgery
Supplemental Material
sj-docx-3-ohn-10.1177_19160216251407670 – Supplemental material for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules
Supplemental material, sj-docx-3-ohn-10.1177_19160216251407670 for Shared Decision-Making During Surgical Consultations for Indeterminate Thyroid Nodules by Victoria Taylor, Travis Pickett, Brooke Turner, Claire Hermiston, Tara Azad, David P. Goldstein, Matthew H. Rigby, Stephanie Johnson-Obaseki, Martin Corsten and David Forner in Journal of Otolaryngology - Head & Neck Surgery
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical Considerations
Ethics approval was obtained through the Nova Scotia Health Research Ethics Board (#1025283) and the Ottawa Health Science Network Research Ethics Board (#20220367-01H).
Consent to Participate
Written informed consent was obtained from all participating patients and surgeons prior to study enrolment.
Data Availability Statement
Data is available upon reasonable request.
Supplemental Material
Additional supporting information is available in the online version of the article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.