
Abstract
Background
The purpose of this study was to develop an effective method of reducing metal artifacts in cochlear implant (CI) electrodes.
Methods
The temporal bones of 30 patients (34 ears) after CI were examined with 320-detector row computed tomography, which was evaluated by two senior radiologists using a double-blind method. Noise, artifact index, signal-to-noise ratio, and the subjective image quality score were compared before versus after using single-energy metal artifact reduction (SEMAR). The electrode position, single electrode visibility, and electrode count were evaluated using SEMAR combined with either multi-planar reconstruction (MPR) or maximum intensity projection.
Results
The two radiologists’ measurements had good consistency. SEMAR significantly reduced the image noise and artifacts index and significantly improved the signal-to-noise ratio and subjective image quality score (P < 0.01). The combination of SEMAR with MPR was conducive to accurate assessment of electrode position and single-electrode visibility. The combination of SEMAR with MIP facilitated accurate and intuitive matching of the assessed electrode count with the number of electrodes implanted during the operation (P = 0.062).
Conclusion
SEMAR significantly reduces metal artifacts generated by CI electrodes and improves the quality of computed tomography images. The combination of SEMAR with MPR and maximum intensity projection is beneficial for evaluating the position and number of CI electrodes.
Background
Cochlear implants (CIs) are currently the most effective treatment for patients with severe-to-profound sensorineural hearing loss, and they have been widely used worldwide. Hearing outcomes after CI have been the most important issue to patients and doctors because they can be affected by many factors. In addition to the cause, duration, and extent of hearing loss and the development of speech function before implantation, the electrode position in the cochlea can also play an essential role in the postoperative effects of CIs [1–3]. Because electrodes cannot be observed in the cochlea by naked eye after implantation, methods to evaluate the electrode position after CI are needed.
The main methods to perform such evaluation are currently X-ray, computed tomography (CT), and other imaging examinations. Among them, X-ray cannot show the structural relationship between the electrodes and the cochlea or their movement in the cochlea [4]. CT has good spatial resolution, contributing to its accuracy in evaluation of electrode implantation. However, CT has higher levels of metal artifacts, which significantly affect the image quality [5–7]. Therefore, methods to reduce or remove artifacts around metal implants are clinically important. Recently, the application of energy spectrum CT [8] and various post-processing technologies [9] after artifact removal has provided some solutions, but the results of such artifact removal remain unsatisfactory.
Single-energy metal artifact reduction (SEMAR) is a new method of metal artifact removal from CT that is time-saving, easy to operate, and reduces the radiation dose [10]. Evaluation of SEMAR has focused on artifacts generated by larger metal implants, such as hip joint, spine, and dental metal implants [11, 12]. However, the evaluation of SEMAR in cochlear implants has not been reported. We seek to determine how effective SEMAR is at improving metal artifacts produced by cochlear electrodes and how to apply SEMAR to electrode evaluation after CI.
In this study, we retrospectively analyzed CT examination results from patients after CI to evaluate the effects of SEMAR on electrode metal artifact removal. The position and number of electrodes were also displayed after SEMAR was combined with multi-planar reconstruction (MPR) and maximum intensity projection (MIP) to assess the methods’ potential application in electrode evaluation after CI.
Materials and methods
Patient population
We included patients who underwent routine 320-row CT (Aquilion ONE, Toshiba Medical Systems, Otawara, Japan) postoperative examination after CI at our institution between August 2018 and February 2019. All patients were included only once (i.e., repeated CT examinations were excluded). The patients underwent CT examination within 1–4 days after CI. During the examination, the patients were placed in supine position with bilateral symmetry. If the patient failed to cooperate with the examination, 10% chloral hydrate was taken orally, and the patient was scanned again after falling asleep.
Objective assessment of image quality
To objectively evaluate image quality, the images acquired on a Toshiba 320-row multi-slice spiral CT were exported to a Vitreacore 6.9.87.1 (Minnetonka, MN, USA) post-processing workstation. A region of interest (ROI) was placed in the bottom of the cochlea, and we measured the number of Hounsfield Units (HU) and its standard deviation (SD) in that ROI. The measurement location and scope were consistent within the same patient and had an area of approximately 5–6 mm2. The SD of the signal within the ROI was set as the image noise. The HU value of the cochlear canal bone was measured when the electrode was rotated at the bottom of the cochlea. This measurement was taken three times, and the mean value was adopted. The CT and SD values of the same tissue with no artifact layer in the preoperative CT image were selected as reference. The artifacts index (AI) was calculated by the following formula: AI=
 [
[Subjective assessment of image quality
To evaluate the subjective image quality, two senior radiologists (with 20 and 27 years of experience) who were blinded to the patients’ identities and the image grouping independently evaluated the images both before and after artifact removal. We set the images without metal artifact removal as Group A and the images after metal artifact removal as Group B. To evaluate if there was any intra-observer variability, the two radiologists scored the images twice at different times. The image quality evaluation before and after artifact removal mainly focused on the display of the electrodes and cochlea. The rating of the MPR images focused on the electrodes’ specific placement, whereas evaluation of MIP images was geared towards observing the overall situation of the electrode. All of the evaluation standards were referenced three-point (0–2) scales, as described by Bartling et al. and Tobias Struffert et al. [14, 15]
The cochlea was rated on a three-point scale, where 0 = severely compromised by artifacts or blurred; 1 = slightly compromised by artifacts or blurred; and 2 = not compromised at all.
Artifacts (blurring, beam hardening) were rated as: 0 = images severely compromised; 1 = minimal artifacts, minimal blurring, but evaluation of inner ear structures and electrode is possible; 2 = without relevant artifacts.
The bony structures’ homogeneity was rated as: 0 = obvious noise; 1 = minimal noise; 2 = homogeneous bony structures, noise barely seen.
The position of the implant within the cochlea concerning the scala vestibuli and scala tympani was rated as: 0 = the electrode is within the cochlea, no other details can be seen; 1 = the position of the electrode relative to the modiolus can be suspected in some parts; 2 = the position of the electrode can be determined relative to the modiolus.
The visibility of single electrodes was evaluated as: 0 = not distinguishable; 1 = blurred, suspected single electrodes can be identified; 2 = single electrodes clearly visible.
Scanning method and related image-processing methods
The localization image was obtained using dual scan mode scanning, and the scanning range was adjusted according to the localization image to range from the tip of the mastoid to the upper edge of the implanted signal receiver. In S&V mode, one layer was swept within the scanning range, and two ROIs were set inside. The high-resolution reconstruction method was adopted, and the scanning parameters were as follows: 120 kVs, 250 mAs, 1-s rotation time, 0.5-mm reconstruction thickness, 0.1-mm reconstruction interval, 512 × 512 matrix, and 50-mm field of view. After the image was transferred to the workstation, two groups of diagrams were obtained for Group A (without metal artifacts removed) and Group B (after SEMAR-based metal artifact removal) (Fig. 1). Then, two reconstruction techniques were applied to Group B: MPR and MIP. The reconstruction method was as follows: transmit the overlapping magnified reconstruction image to a Vitreacore 6.9.87.1 workstation, import it in “Inspace” mode, select the threshold range of − 1000 to + 1000 HU to display the inner ear structure, and then add a threshold range of 2500–5000 HU to display the electrode.

Statistics
Statistical analysis was performed with SPSS (version 25.0). Two independent-samples t tests were used for inter-group comparison. Enumeration data were compared using χ2 tests. Differences were deemed statistically significant at P < 0.05.
Results
Patient
Patient and electrode characteristics

aBoth types of cochlear implants are made of platinum and iridium
Subjective assessment of SEMAR images
To explore the application of SEMAR to electrode evaluation after CI, two radiologists subjectively graded the cochlea, electrode artifacts, and bone structure uniformity on CT images. We found that before and after the application of SEMAR, intra-observer reliability between different times was high (Fig. 2, Tables 2 and 3), and no significant difference was found between the two radiologists’ scores for the cochlea, electrode artifacts, or bone structure uniformity, indicating good inter-observer consistency (Fig. 2). The Group A images were greatly affected by electrode artifacts: part of the cochlea was obscured by the artifacts, and the visibility of the electrode conditions was poor. However, electrode artifacts were reduced in Group B images, which allowed clear observation of the conditions of the cochlea and electrodes (Fig. 3). The scores for cochlea, electrode artifacts, and bone structure uniformity were significantly improved in Group B (P < 0.01), suggesting that SEMAR improves CT image quality after CI (Fig. 2).

Consistency analysis and scoring results of the subjective scoring before and after artifact processing.
The analysis of intra-observer reliability with non-SEMAR. (n = 34 each) (x ± s)

The analysis of intra-observer reliability after the application of SEMAR. (n = 34 each) (x ± s)


CT images of cochlear implants before and after using SEMAR. The image is greatly affected by electrode artifacts before using SEMAR, as part of the cochlea is obscured by the artifacts, and the electrode condition is displayed unsatisfactorily (
Quantitative assessment of SEMAR images
Objective analysis of the two groups’ image quality (n = 34 each) (x ± s)

HU Hounsfield Units, AI Artifacts index, SNR Signal-to-noise ratio, SEMAR Single energy metal artifact reduction
Evaluation of images processed by SEMAR combined with MPR or MIP
To further evaluate the accuracy of electrode positioning in the cochlea, we performed MPR on the CT images after the SEMAR-based artifact removal. Furthermore, to count the number of electrodes in the cochlea, we combined MIP with SEMAR. The scores for electrode position, single-electrode visibility, and electrode count were consistent between the two radiologists (Fig. 4). We found that images processed with SEMAR combined with MPR clearly elucidated the inner ear's fine structure, which is conducive to accurate assessment of the electrode position in the cochlea and its effect on the modiolus and bone spiral plate (Fig. 5). Furthermore, SEMAR combined with MIP clearly showed the overall electrode condition. Additionally, the electrodes could be counted accurately: the count matched the number of electrodes implanted during the operation (P = 0.062) (Fig. 6).
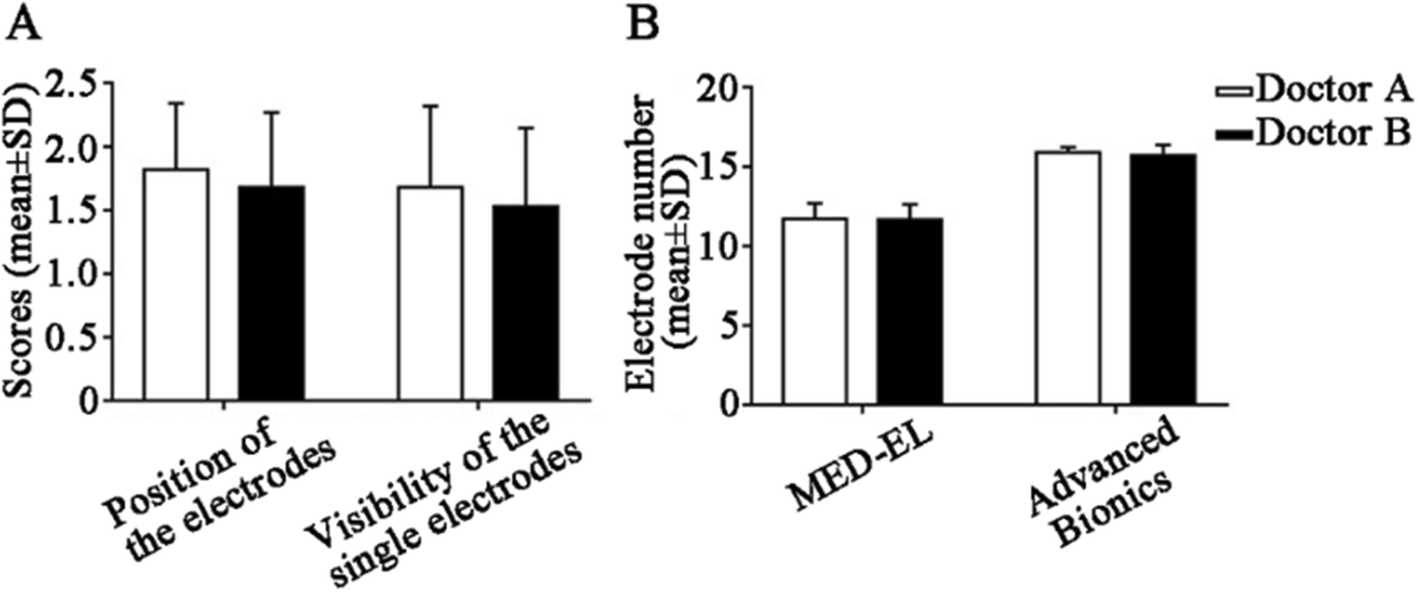
Consistency between two radiologists on scores of images processed by MPR and MIP.

CT image of cochlea after using SEMAR combined with MPR. In the SEMAR CT image, the electrode is clearly located in the cochlea, it is difficult to evaluate whether the electrode is located in the scala tympani (

CT image of cochlea after using SEMAR combined with MIP. Counting electrodes using the SEMAR CT image requires superimposition of electrodes from different layers to count the electrodes in the cochlea, which requires complex operations (
Discussion
Postoperative imaging evaluation of CI has great value for clinical evaluation of the number, depth, and position of implanted electrodes [16]. Although the depth and number of implanted electrodes can be measured and counted during the operation, the possibility of rear electrode displacement cannot be excluded. The study of Rivaset and Fayad showed that it is optimal to observe the displacement of implanted electrodes in the first week after CI [17, 18]. This is because no fiber sheath or fixation cover grows within 1 week after the surgery. Therefore, complications such as shedding and twisting may occur, but generally, this does not degrade electrode performance or cause clinically visible discomfort. Postoperative imaging examination of CI is one of the main methods to determine electrode condition, especially among patients with poor hearing after CI. Therefore, comprehensive evaluation needs to be done to rule out problems with the cochlear electrodes after the operation.
Previous studies have indicated that high-resolution CT can facilitate identification of the inner ear's fine structure and evaluation of the specific situation of electrodes in the cochlea after CI [19]. However, the artifacts caused by metal electrodes make the evaluation of postoperative complications and electrodes difficult. In this study, applying SEMAR significantly reduced image noise and AI and significantly improved the subjective scores of SNR and image quality, suggesting that SEMAR reduces metal artifacts of cochlear electrodes and improves image quality. However, SEMAR had no significant effect on the CT value of the bone cochlear canal bone (P > 0.05), which was different from the method's results in other fields [11, 12]. Bamberg believed that the size of metal artifacts mainly depends on the thickness and material of the metal [20]. The soft tissues around the implant, such as muscle and fat, are the most disturbed by the artifacts. Previous research has mainly focused on the effects of SEMAR on the removal of artifacts of larger metal implants in the human body, and those studies measured the CT values of the soft tissues around the implants. Therefore, we consider that SEMAR may have a small effect on CT values of the inner ear because of the small volumes of the cochlear electrodes and the bone around them.
The inner ear's structure is fine, with dimensions mostly on the millimeter scale, and therefore the choice of observation level greatly impacts the examination results. The conventional axial and sagittal orientations are not observed along the axis of the inner ear structure, which may introduce misinterpretation [21]. The structural identification of the inner ear used high-resolution CT, but conventional CT images can be adjusted to any level using MPR. Previous literature reported that double oblique MPR can fully display the temporal bone structure. Compared with axial and coronal images, the post-MPR images presented the inner ear structure more clearly and intuitively. At the same time, compared with the three-dimensional reconstruction method, the MPR method is more objective, less susceptible to human factors, and simpler to operate [22]. Some scholars believe that MPR can improve the detection rate and accuracy of inner ear deformities [23, 24]. In this study, we combined MPR with SEMAR and successfully showed that the electrodes in the investigated cases were all located in the cochlea (i.e., without incorrect implantation).
In post-processing of CT images, MIP is a method of projecting three-dimensional spatial data onto the visual plane [25]. We used MIP to project high-density electrodes onto the CT image plane, and this showed the overall electrode conditions clearly, so that the electrodes could be counted directly in a single image. The resulting count was consistent with the number of electrodes actually implanted during the operation (P = 0.062). Because the CIs used in our center are MED-EL and Advanced Bionics (12 and 16 electrodes respectively), there is a certain distance between the electrodes, and single electrodes are less affected by metal artifacts. Subsequent studies should include more types of implants to evaluate SEMAR combined with MPR/MIP using more electrodes and less electrode spacing.
Conclusions
In summary, SEMAR can significantly reduce metal artifacts generated by CI electrodes and improve CT image quality. SEMAR combined with MPR and MIP can clearly, intuitively, and accurately display the shape, position, and number of electrodes in the cochlea, which is worthy of clinical application.
Footnotes
Acknowledgements
Authors’ contributions
All of the authors were involved in the conception and design of the study, the analysis and interpretation of data, and the revision of the manuscript and have approved the final manuscript.
Funding
The study was supported by grants from the Natural Science Foundation of China (81902753), Guangdong Basic and Applied Basic Research Foundation (2019A1515010620) and Guangzhou Science and Technology Program (201803010033).
Availability of data and materials
All data are available upon request from the authors.
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Fanqin Wei and Jiahui Li contributed equally to this work.