
Abstract
Background
Acute exacerbations (AE) in chronic rhinosinusitis (CRS) have been increasingly recognized as an important clinical issue. The purpose of this study is to summarize the current definitions and evaluation parameters of AE and then identify and quantify the clinical and immunopathologic characteristics of AE in CRS.
Methods
A systematic review of the literature was performed on PubMed, Scopus, and Cochrane databases from January 1990 through August 2020 to identify studies relating to AE in CRS. Exclusion criteria included non-English and non-human studies, and case reports.
Results
The definitions of AE in CRS among all the studies were based on a description of short-term worsening sinonasal symptoms. Patient-reported sinus infection and exacerbation related medical treatment during the preceding 3 months to 1 year were used to evaluate the frequency of AE in CRS. The average decline in 22-item Sino-Nasal Outcome Test (SNOT-22) score during an exacerbation was 7.83 points relative to baseline. Comorbid asthma, SNOT-22 scores ≥24, allergic rhinitis, eosinophil count ≥150/μL and autoimmune disease were positively associated with an exacerbation-prone CRS phenotype. AE in chronic rhinosinusitis with nasal polyps (CRSwNP) was associated with increased expression of mucus cytokines including myeloperoxidase (percentage increase [PI] = 101%), IL-5 (PI = 125%), and IL-6 (PI = 162%) and could be predicted by the increasing mucus cystatin and periostin.
Conclusion
The definition of AE in CRS is largely driven by patient-reported symptoms and is associated with several risk factors. Quantitative changes in mucus cytokines associated with AE in CRSwNP and may be used to predict events. The development of a consistent definition of AE in CRS is critical to help define disease control and treatment efficacy.
Keywords
Introduction
Chronic rhinosinusitis (CRS) is often associated with a fluctuating disease course. Acute exacerbations (AE) in CRS have been shown to directly account for increasing healthcare costs [1, 2], annual physician visits [3], and significant decreases in workplace productivity [4, 5]. Recently, the frequency of AE has been identified as an independent predictor of quality of life [6]. Based on the current guidelines, an acute exacerbation is defined as an acute and transient worsening of preexisting symptoms in patients with CRS [7, 8]. However, there is no consensus definition of how to quantify AE due to multifactorial etiologies and inconsistency in endpoint reporting.
Prior attempts to report on AE have relied on empirical clinical criteria. For example, Rank et al. utilized diagnosis coding and at least one of the following: prescription for systemic antibiotics, systemic corticosteroids, plans for surgical intervention, emergency department or urgent care visit, or hospitalization for CRS [9]. Similarly, Sedaghat et al. used three metrics to assess the frequency of AE including patient-reported sinus infections, CRS-related antibiotic courses, and CRS-related oral corticosteroid courses, each over the preceding 3 months [6, 10, 11]. These direct treatment-related metrics of AE facilitate assessment on the AE in CRS but fail to correlate the AE in CRS with both degree of subjective changes in clinical symptoms and objective measures of inflammation.
The purpose of this study is to therefore utilize a systematic review of the literature to summarize the current definitions and evaluation parameters of AE and then quantify both the clinical and immunopathologic characteristics of AE in patients with CRS.
Methods
An evidence-based systematic review was performed utilizing the Preferred Reporting Items for Systematic Reviews and Meta-Analysis (PRISMA) guidelines. A comprehensive search of PubMed, Scopus, and Cochrane databases from January 1990 through August 2020 was conducted to identify studies relating to the AE in CRS. A combination of terms was used to maximize the probability of finding all relevant publications: acute exacerbation, exacerbation, chronic rhinosinusitis, rhinosinusitis, chronic sinusitis, nasal polyps and polyposis.
Study selection
Titles and abstracts of all the relevant studies were reviewed by 2 independent authors (DW and YW). Included studies addressed the etiology, characteristics, and diagnosis of AE in CRS. All included studies were downloaded and the full-text was reviewed by both authors. Studies were excluded if they were: non-English, non-human studies, case reports, or not related to the present study. Figure 1 outlines the search strategy and inclusion process used to find relevant studies.

Flow diagram of the study
Data extraction and analysis
Data included year of publication, study design, age range, diagnostic criteria, bacterial findings, immunohistologic findings, risk factors, and conclusions. After analysis of each article, summary tables were developed. The quality of included studies was determined from the Oxford Center for Evidence Based Medicine Levels of Evidence categorization, based on study design as well as clinical endpoints [12].
Results
Included studies
The initial database search identified 255 articles (Fig. 1). Duplicates, non-full text, non-English, and data not extractable articles were excluded (n = 239). A total of 19 articles underwent a full-text assessment for eligibility and met the final inclusion criteria for systematic review. Nine studies explored the clinical characteristics of AE in CRS including the clinical metrics and risk factors of AE in CRS. Another seven articles focused on the in vivo immunologic characteristics associated with AE in CRSwNP.
Diagnosis of AE in adult patients with CRS
Descriptive diagnosis of acute exacerbations in adult patients with CRS

CRS Chronic rhinosinusitis, CF Cystic fibrosis, AE Acute exacerbation, ICAR: RS International Consensus Statement on Allergy and Rhinology: Rhinosinusitis, EPOS European position paper on rhinosinusitis and nasal polyps, ARS Acute rhinosinusitis
Quantitative clinical metrics of AE in CRS
Quantifiable metrics of acute exacerbations in CRS

CRS Chronic rhinosinusitis, AE Acute exacerbation, QOL Quality of life, SNOT-22 The 22-item Sino- Nasal Outcome Test

Clinical characteristics of acute exacerbations in adult patients with CRS.
Clinical risk factors for AE in CRS
Clinical risk factors for acute exacerbations in CRS

CRSwNP Chronic rhinosinusitis with nasal polyps, CRS Chronic rhinosinusitis, NSS Nasal and sinus symptoms, SNOT-22 The 22-item Sino- Nasal Outcome Test, ACT Asthma control test, AE Acute exacerbation, ESS Endoscopic sinus surgery
In vivo immunologic characteristics of AE in CRS
Immunologic characteristics of acute exacerbations in CRSwNP
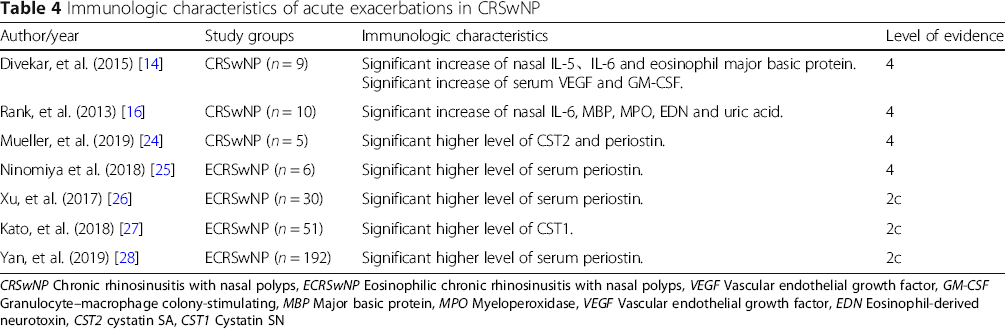
CRSwNP Chronic rhinosinusitis with nasal polyps, ECRSwNP Eosinophilic chronic rhinosinusitis with nasal polyps, VEGF Vascular endothelial growth factor, GM-CSF Granulocyte–macrophage colony-stimulating, MBP Major basic protein, MPO Myeloperoxidase, VEGF Vascular endothelial growth factor, EDN Eosinophil-derived neurotoxin, CST2 cystatin SA, CST1 Cystatin SN
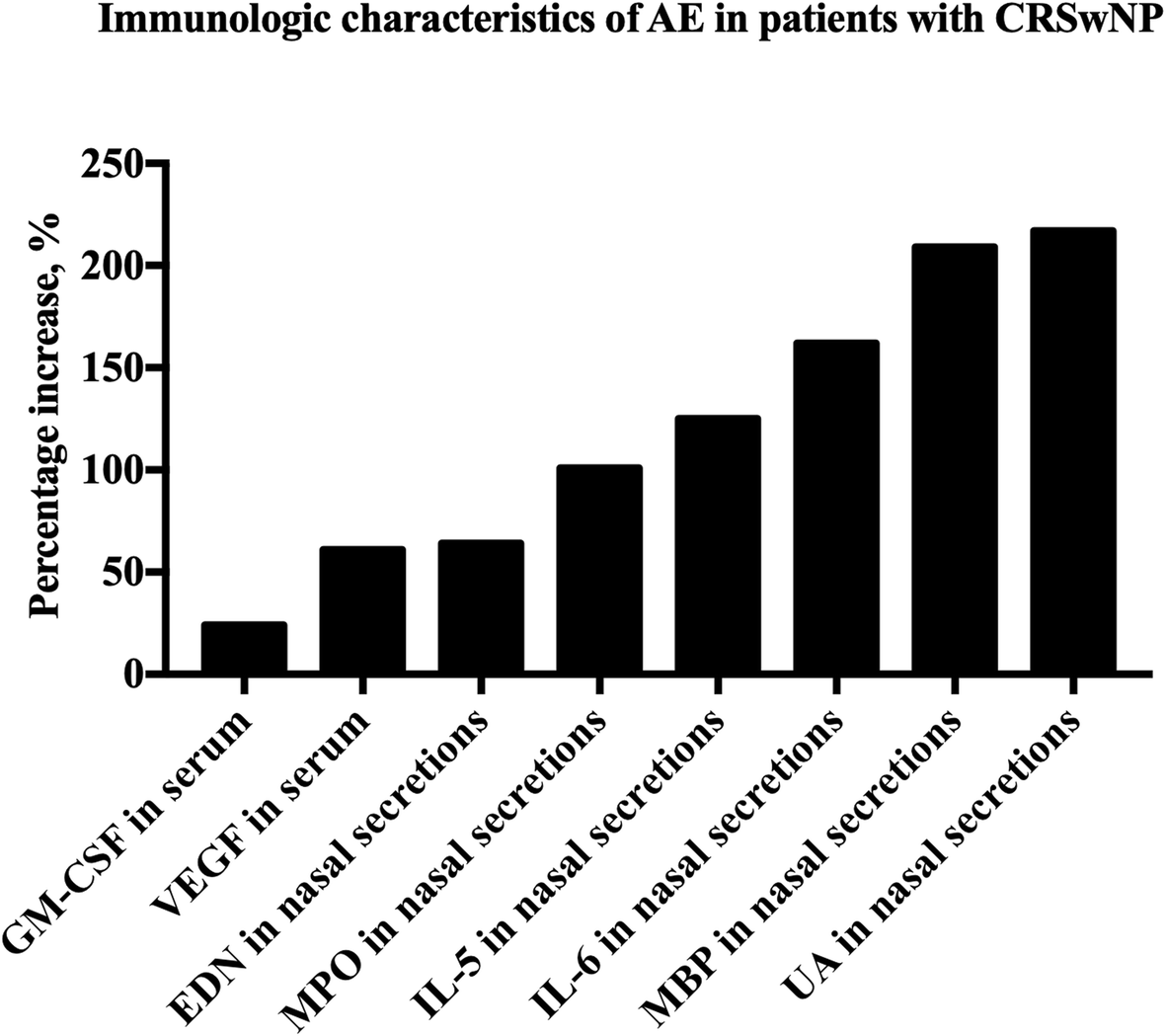
Immunologic characteristics of acute exacerbations in adult patients with CRS. AE, acute exacerbations; CRSwNP, chronic rhinosinusitis with nasal polyps; GM-CSF, granulocyte–macrophage colony-stimulating; VEGF, vascular endothelial growth factor; EDN, eosinophil-derived neurotoxin; MPO, myeloperoxidase; MBP, major basic protein; UA, uric acid
Discussion
Defining acute exacerbations of CRS with quantifiable clinical and immunologic metrics has remained a challenge due to the complex etiology of acute exacerbation and the inconsistency in endpoint reporting. Current guidelines regarding treatment of AE in CRS continue to recommend blanket medical intervention including short-course antibiotic treatment [7, 8]. Thus, an improved method of clinically defining AE in CRS and its risk factors is critical to facilitate individualized treatment as well as more effective preventions aimed improving overall quality of life.
We first reviewed the current diagnostic criteria of AE in CRS and found certain discrepancies between studies. The definitions of AE in CRS rely largely on descriptive changes in sinonasal symptoms that occurred in an acute fluctuation pattern (Table 1) [7, 8, 13–15, 17, 29]. Consequently, we sought to identify more specific quantitative metrics which could be used to provide a common definition between studies. Patient-reported number of sinus infections and treatments-related metrics were available in several studies (Fig. 1) [6, 9, 10]. An exacerbation-prone CRS phenotype was defined as more than 3 times of exacerbations in the last 12 months [18]. Previous studies showed that asthma, elevated SNOT-22 scores, allergic rhinitis, eosinophil count of at least 150 cells per microliter, and autoimmune disease were positively associated with an exacerbation-prone CRS phenotype [18, 22]. However, the presence of nasal polyps was negatively associated an exacerbation-prone CRS phenotype [18]. This is similar to a previous study that found that CRSwNP are less likely to use antibiotics, which could serve as a proxy for an exacerbation, relative to other phenotypes of CRS patients [30]. SNOT-22 scores during active and inactive exacerbation were also characterized. A high average of SNOT-22 scores of 37.55 ± 21.06 was calculated from six studies indicating a high subjective burden of disease among exacerbation prone patients [6, 11, 14, 18–20]. In addition, average change in SNOT-22 score during an exacerbation was 7.83 points higher as compared with routine visits [13, 14]. The established minimal clinically important difference (MCID) for SNOT-22 is 9 to 12 based on two previous studies [23, 31]. While the SNOT-22 change during exacerbation appears slightly below this accepted MCID, this may be due to smaller sample size or the fact that the MCID was validated against therapeutic interventions, not spontaneous exacerbations of chronic disease.
We next summarized the clinical risk factors for AE in CRS. Winter season, hay fever, asthma, sinus surgery history, current long-term CRS status, and high body mass index were all independent risk factors which predicted AE in CRS [9, 15]. Furthermore, high baseline SNOT-22 scores and low ACT scores were highly associated with the frequency of AE in CRS in the preceding 3 months [6, 11]. Interestingly, a high positive bacterial culture rate of 90.9% was detected in patients during exacerbations [21]. These findings would facilitate preventive interventions on these risk factors to reduce exacerbation frequency.
Immunologic changes that occur during exacerbation offer a potential objective measure to confirm AE in CRS and perhaps even to predict it. The current literatures about the immunologic changes during exacerbation were all about patients with CRSwNP and studies about the immunologic changes of CRS without nasal polyps during exacerbation were lacking. From a systemic perspective, only GM-CSF and VEGF in patients with CRSwNP during exacerbation were significantly increased in serum samples when compared with controls [14]. Previous studies had shown that local production of both VEGF and GM-CSF in nasal polyps [32–34]. It is now understood that VEGF and GM-CSF play an important role in tissue remodeling and inflammatory responses. With respect to local nasal biomarkers, EDN, MPO, IL-5, IL-6, MBP, and UA within nasal secretions were all significantly increased when compared with controls [14, 22]. Previous studies have shown that EDN, IL-5 and MBP are involved in type 2 immune responses and eosinophilic inflammation [35]. MPO is a biomarker of the neutrophil activation and high levels of MPO represent increased neutrophilic inflammation [36]. Increased IL-6 response has been associated with onset of the viral upper respiratory tract infection in healthy individuals or virus-induced asthma exacerbations [37, 38]. High serum uric acid is an indicator of oxidative stress [39] and it has proved to be a marker of the severity of asthma exacerbations [40]. These studies thereby indirectly support the role of type 2 immune responses, neutrophilic inflammation and anti-viral activity in the pathogenesis of AE in CRSwNP. Interestingly, upregulation of these serum and nasal mucus biomarkers corresponded well with subjective patient-reported worsening of symptoms suggesting that these cytokines may indeed be a reliable measure of AE in CRSwNP.
Recent transcriptomic and proteomic studies exploring the pathogenesis of CRS have revealed a variety of upstream targets which appear to contribute to inflammation in CRSwNP [41, 42]. As these biomarkers may be non-invasively sampled in a prospective and serial manner, Mueller et al. demonstrated that mucus cystatin 2 and periostin levels were capable of predicting worsening SNOT-22 scores, a proxy for AE in CRSwNP, and even the need for revision surgery among patients with CRSwNP months in advance [24].
Conclusions
AE in CRS has gained increasing attention due to its significant influence on patients’ quality of life and healthcare costs. The definition of acute exacerbation in patients with CRS to date has been generally descriptive. Our review of the literature suggests that AE in CRS is associated with an average of a 7.83-point decline in SNOT-22 and that patients with hay fever, asthma, sinus surgery history, current long-term CRS status, high body mass index, and during winter season as risk factors are at greatest risk of AE in CRS. Furthermore, AE in CRSwNP appears to be associated with significant increases in serum levels of GM-CSF and VEGF, as well as multiple nasal mucus cytokines including IL-5, IL-6, and MPO. Finally, recent studies suggest that upstream mucus biomarkers of Type 2 inflammation including Cystatin and Periostin may be used to predict an impending AE in CRSwNP. More studies are needed to build a consensus of the certain definition of AE in CRS which is based on the combination of the subjective and objective parameters.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
DW analyzed the data and drafted the manuscript. BSB designed the study, read, and revised the manuscript. YW designed the study and revised the manuscript. All authors have read, edited, and approved the final manuscript.
Funding
This study was supported by the Natural Science Foundation of China (81670903), Capital Health Research and Development of Special Fund (2018–2-2065), Beijing Science and Technology Nova Program (Z201100006820086), and Beijing Hospitals Authority Youth Programme (QML20190617).
Availability of data and materials
All data gathered for the systematic review was gathered from articles cited in the paper and listed in the reference section.
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.