
Abstract
Background
Inverted papilloma (IP) is an unusual type of benign tumor that has high recurrence rates and the potential to transform into squamous cell carcinomas (SCC). The mechanism of the transformation process from IP to IP-SCC is uncertain and there is no consensus regarding the best practice for IP-SCC detection. The goal of this study is to identify the best clinical methods to detect for IP-SCC.
Methods
An evidence-based review was performed using Medline and Ovid to obtain all articles up to October 10th, 2019 pertaining to identification of IP malignant transformation. All manuscripts discussing clinical methods or biomarkers were included.
Results
Based on clinical research studies, convoluted cerebriform pattern and apparent diffusion coefficient values on Magnetic Resonance Imaging (MRI) can help differentiate benign IP from SCC and increased SUVmax on PET/CT is associated with higher probability of malignancy although not as specific. No consensus about the best biomarker for IP-SCC has been reached among researchers and continues to be exploratory.
Conclusion
Endoscopy with biopsy is the gold standard practice to identify IP-SCC; however, MRI is the preferred imaging modality to recognize malignant transformation in cases where biopsy is difficult. Multiple biomarkers have shown positive results, but no single indicator with clinical significance for monitoring malignant transformation process has been found.
Keywords
Background
Inverting papilloma (IP) is a challenging condition to manage in the sinonasal cavity. A recent literature review has shown that the best surgical approach to the management of IP is endoscopic [1]. However, the challenge remains on how to best surveillance these patients postoperatively, especially if the recurrence converts to malignant transformation. To our knowledge, the most up to date IP recurrence rate is 13.72% with a malignant transformation potential of 7.6% [1–3]. Given that the recurrence and malignant transformation can happen more than 8 years after the preliminary surgery, follow-up of 3 years or greater is recommended [4, 5].
The reported incidence of malignancy in IP varies greatly in the literature, and has been reported as high as 27%, but most commonly is seen to be between 5 and 10% [2, 6–8]. The majority of the malignant cases are squamous cell carcinoma (SCC), it can form synchronously or metachronous from IP. In a meta-analysis in 2007, Mirza et al. found a risk of 7.1% of synchronous carcinomas and a risk of 3.6% of metachronous malignancies [8]. Re et al. identified a 9% overall rate of malignant transformation in 2017 [2]. No significant correlation was found between tumor stage and histologic differentiation in these IP-associated malignancies [9]. The survival rates for patients with malignant transformation are quite low, with the five-year post-surgery survival rate ranging from 39.6 to 65.7% and an average survival of 3.4 years [10, 11].
While the most common surveillance technique is endoscopy [1] followed by a biopsy if there is a concerning finding, surgeons struggle to check areas in the nose that cannot be easily visualized such as the lateral frontal sinus, the anterior medial maxillary sinus and sinus cavities that have stenosed due to post-surgical healing. Therefore, surgeons require other surveillance techniques to best identify incidents of IP recurrence but more importantly the transformation to SCC. Moreover, it would be beneficial to know a priori which IPs have a higher risk of transformation. There is growing understanding regarding the biology of IP transforming to SCC; it is therefore important to summarize this body of literature as it may provide surgeons with another way of determining whom to follow up more closely. Recommendations will be made based on levels of evidence while weighing benefits and risks. As recommendations may not apply to all IP patients, clinical judgement is required on a per case basis.
Methods
Surveillance options for IP malignant transformation

Defined grades of evidence and recommendations [AAP ref]

Results
After reviewing 249 papers, the results were summarized together under ‘clinical surveillance techniques’, ‘computed tomography’, ‘magnetic resonance imaging’, ‘PET-CT with FDG’, and ‘biological markers’.
Clinical surveillance techniques
General principles
Certain general demographics might influence how clinicians schedule surveillance plans for patients. Therefore, in order to guide clinical decisions, All studies that discussed the location, follow-up and clinical risk factors associated with IP-SCC were included in this review.
Location (Table 3)
General location for IP malignant transformation surveillance

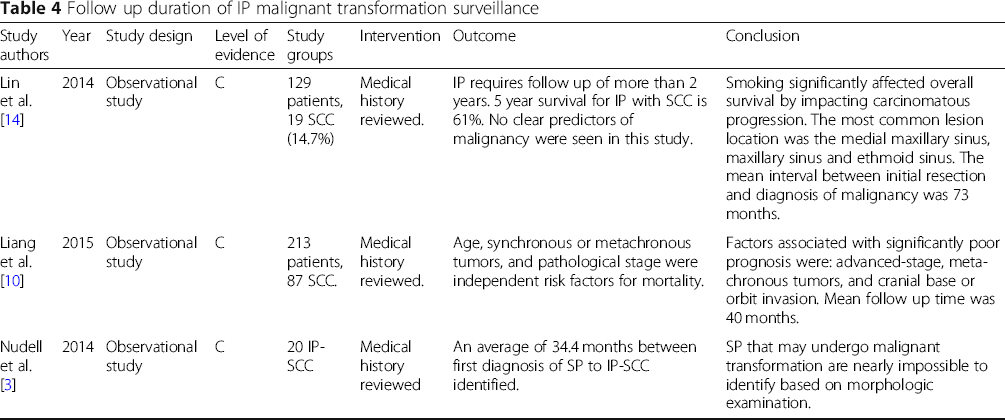
Follow-up (Table 4)
Follow up duration of IP malignant transformation surveillance
Clinical risk factors (Table 5)
Clinical risk factors of IP malignant transformation

Endoscopy
Clinical examination, particularly endoscopic exams, are crucial for surveillance. Currently the confirmation diagnosis of IP-SCC depends on histopathological results. Clinicians use endoscopic sinonasal examination to monitor for a recurrence of an IP. However, it is often difficult to detect a malignant transformation of a benign IP from visual inspection, particularly if the tumors are not easily visible by nasal endoscopy. Moreover, IP-SCC often do not involve the entire tumor, hence the biopsies can be non-representative and are not highly reliable [9].
Aggregate grade of evidence: NA Benefit: direct visual inspection, easily accessible, biopsy is the gold standard of confirming presence of IP-SCC. Harm: bleeding and infection risk, chance of missing the tumor. Cost: low Benefit harm assessment: Benefit outweighs harm. Value judgement: Endoscopy followed by a biopsy is the first line method for IP-SCC identification. Recommendation level: Recommended. Intervention: First line method for long term surveillance.
Computed tomography
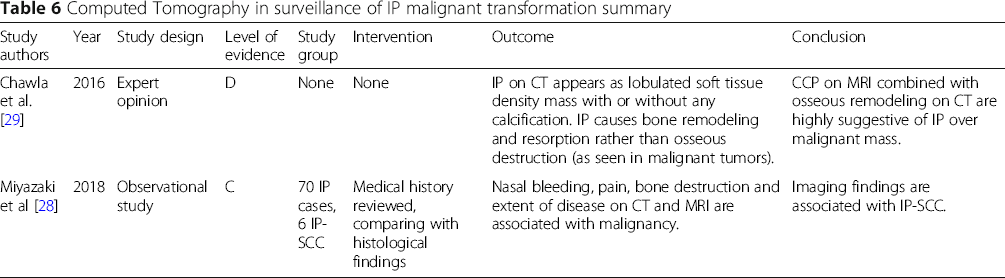
There are no studies that support the use of CT to identify the presence of IP-SCC (Table 6). A level 4 study by Chawla et al. indicated that IP on a CT scan can show bone remodeling and resorption rather than osseous destruction, which is more often seen in malignant tumors [29]. Miyazaki et al. found that bone destruction was significantly higher in IP-SCC with 3 out of 5 IP-SCC patients were found to have bone destruction [28]. The finding was quite nonspecific. The studies do not prove the efficacy of CT scans in differentiating IP from IP-SCC.
Aggregate grade of evidence: NA (only 1 Level 4 study) Benefit: No evidence differentiating IP from IP-SCC on CT scan. Harm: Concerns regarding radiation exposure. Cost: Moderate Benefit harm assessment: No benefit for IP-SCC identification. Value judgement: Require more research Recommendation level: No recommendation Intervention: None. Computed Tomography in surveillance of IP malignant transformation summary
Magnetic resonance imaging
Five studies were included in the review (Table 7). Convoluted cerebriform pattern (CCP), alternating hypointense and hyperintense bands on T2 weighted and contrast enhanced T1 weighted images have been reported as a reliable MRI features of IPs [30]. CCP has been found in all IP cases as well as in some malignant tumors [29, 32]. In IP, CCP is generally diffuse. A focal loss of CCP pattern maybe indicative of a malignancy [35]. A recent study showed that loss of CCP and low apparent diffusion coefficient (ADC) values on MRI with diffusion-weighted imaging can help differentiate IP-SCC from IP with 100% specificity (grade B evidence) [30]. Bone destruction with or without sinonasal extension could be used as an indication of IP-SCC(grade C evidence) [34]. Because IP causes bone remodeling and resorption rather than osseous destruction, Zhang et al. suggested that diffused CCP on MRI combined with bone remodeling on CT may be highly suggestive of IP over IP-SCC [36].
Aggregate grade of evidence: Level 2: 2 studies; Level 3: 3 studies; Benefit: MRI imaging feature can help differentiate IP from IP-SCC. Harm: Repeated exposure to gadolinium, claustrophobia, and heating/dislodgement of implanted metal. Cost: Moderate/High. Benefit harm assessment: Benefit outweighs harm. Value judgement: Require more research. Recommendation level: Recommended. Intervention: Using CCP and ADC value, MRI has capacity to identify IP-SCC. MRI is recommended if biopsy is not achievable or there are concerns of the accessible part of the tumor to biopsy inaccurately representing the entirety of the tumor. MRI in surveillance of IP malignant transformation summary

Positron-emission tomography with 18F-fluoro-deoxyglucose (PET-CT with FDG)
PET-CT studies have shown that IP patients have higher SUV max than non IP patients, and IP-SCC patients have higher SUVs than IP patients (Table 8) [37]. However, Joen et al. found that SUVs for IPs can at times be high leading to a false diagnosis of IP-SCC [35]. Allegra et al. reported a case where PET-CT failed to identify the primary malignant site because there was no SUV increase in the IP-SCC site [38]. Consequently, PET-CT with FDG can be used as an adjunct tool but cannot be solely relied upon making the diagnosis of IP-SCC.
Aggregate grade of evidence: Level 2: 2 studies; Level 3: 2 studies; Level 4: 2 studies. Benefit: SUV max can increase suspicion of IP-SCC. Harm: Radiation exposure. Cost: High. Benefit harm assessment: Equal balance of benefit to harm. Value judgement: Challenging to recommend PET-CT use in the identification of IP-SCC due to contradicted research results and costs. Recommendation level: None. PET/CT in surveillance of IP malignant transformation summary

Biological markers
Genetic factors
Multiple genetic factors have been identified as potential malignant transformation markers for IP.
P53 is a transcription factor controlling cellular proliferation and apoptosis via the regulation of genes involved in cell-cycle arrest, DNA repair, and apoptosis [39]. Ten retrospective studies investigating the association between P53 levels and IP malignant transformation were found,. Four studies support a positive association of mutant P53 level and malignant transformation [40–43], three studies reported no relation between level of mutant P53 and transformation rate [39, 44, 45] and the remaining studies were inconclusive [46, 47]. No conclusion can be drawn about whether P53 is involved in the malignant transformation process.
P21 cyclin-dependent kinase inhibitor is a cell cycle progression control factor. It promotes cell cycle arrest in response to a variety of stimuli. The inhibitory effect of P21 on cell cycle progression correlates with its nuclear localization. P21 can be induced by both p53-dependent and p53-independent mechanisms [40, 41]. Two out of four reviews supported P21 to play a role in malignant transformation and to be a pathological marker for malignant transformation [42, 46], and two studies reported no association of P21 levels with malignant transformation [39, 47]. Both used immunohistochemical staining to make retrospective comparisons of pathological specimens from IP, IP with dysplasia, and SCC.
Muscle segment homeobox gene MSX2 is implicated in cellular differentiation and survival. Zhang et al. [48] noted significantly higher levels of MSX2 mRNA in IP-SCC than in controls and Wu et al. observed expression of MSX2 in 100% of IP-SCC and significantly greater expression in IP with severe dysplasia than in IP and control [49]. These studies support the potential use of MSX2 as a target for monitoring malignant transformation.
PDCD4 is a tumor suppressor gene that has been previously implicated in the progression of many types of tumours. Compared to controls, Wang et al. noted a significant decrease in PDCD4 expression in IP [50]. Furthermore, altered expression of the gene was correlated with dysplastic features, indicating that it may be used to predict IP progression and malignant transformation.
Targeted amplicon sequencing by Yasukawa et al. identified significant genetic mutation of the KRAS gene in SCC-associated and dysplastic IP as compared with nondysplastic IP [51]. The use of KRAS mutation to predict malignant transformation had a sensitivity of 85%, a specificity of 90%, a positive predictive value 91% and a negative predictive value of 75%, indicating its effectiveness as a marker.
Phosphatase and tensin homologue, PTEN, is a tumor suppressor gene. Zhang et al. found that decreased expression of PTEN was associated with both IP dysplasia and malignant transformation [52]. While Kakizaki et al. found no significant difference in expression between non-dysplastic and dysplastic IPs, they similarly noted decreased PTEN in SCCs as compared to IPs, validating its use as a biomarker of carcinogenesis [52, 53].
Proteins
Squamous cell carcinoma antigen (SCCa) is one of the most reliable tumor markers for squamous cell carcinoma. Three studies associated a high level of serum SCCa with IP progression, growth, and recurrence [54–56]. This might help the surgeon in the postoperative setting by identifying high-risk patients and planning follow-up strategy tailored to the individual patient.
Fascin is an actin cross-link binding protein required for the formation of actin-based cell-surface protrusions and cell motility. Fascin up-regulation in lung, gastric, breast and hepatobiliary carcinomas correlates with aggressiveness and decreased survival. Two retrospective studies examined the association between fascin and IP-SCC by using immunohistochemical staining of specimens taken from different groups: IP, IP with high dysplasia, IP with SCC and normal control tissue. It was found that fascin expression increased gradually and significantly with the progression and severity of dysplasia [57–59].
Survivin, an inhibitor of apoptosis, is also found to be potentially correlated with SCC. Nuclear survivin expression was significantly higher in SCCs than in IPs in one study [60].
Two studies found that increased expression of COX-2, a rate-limiting enzyme in prostaglandin synthesis, might be linked with malignant transformation [51, 61, 62]. The osteopontin-VEGF (vascular endothelial growth factor) axis has been implicated in tumor progression and angiogenesis. Liu et al. and Wu et al. found significantly greater immunohistochemical staining and mRNA expression of OPN and VEGF in higher-stage IP specimens than in lower-stage tissues [63, 64].
E-cadherin and β-catenin are cell adhesion molecules commonly used to mark the epithelial to mesenchymal transition [65]. Correspondingly, an immunohistochemical analysis by Koo et al. demonstrated lower levels of E-cadherin and β-catenin in IP-SCC than in IPs [66], and Stasikowska-Kanicka et al. found the immunoexpression of E-cadherin to be decreased in SCC as compared to IP [65].
Ki-67 is a marker of cell proliferation, in immunohistochemical studies of protein expression, Tsou et al. observed significantly greater Ki-67 staining in IP-SCC as compared with non-recurrent IP [67]. Ki-67 was considered a signal of poor prognosis and malignant transformation [67].
Sahnane et al. identified that occupation exposure increases LINE-1 hypomethylation which might be an epigenetic marker [68].
Viral
Because IP shares certain clinical characteristics with recurrent respiratory papillomatosis, namely high recurrence, confined aggressiveness, and malignant transformation potential, Jalilvand et al. contend that IP likely also has an infectious etiology [69]. Identifying such an agent would prove invaluable in predicting tumor progression and developing future therapies. Human papillomavirus (HPV) has long been suggested and investigated as a potential driving agent. HPV is a DNA virus that shows tropism for epithelium, leading to epidermal and mucosal infections wherein the virus is integrated into the host DNA.
In IP specimens, HPV positivity ranged between 9 and 60%. Comparatively, controls ranged between 0 and 7.6% [7, 69–77]. The most common HPV strains observed in IP were HPV-6 and HPV-11. Significantly higher HPV positivity was found in cases with moderate to severe dysplasia as compared cases with low grade dysplasia [74, 78]. There is good evidence that HPV infection is implicated in the tumorigenesis of IP. Regarding malignant transformation, HPV positivity in SCC tissues has been recorded as between 0 and 100% [69–73, 75–77, 79]. Inconsistencies in reported numbers have been attributed to small sample sizes, degradation of DNA in paraffin-embedded tissues, use of inferior techniques of detection, and geographic factors. Udager et al. found that EGFR mutations and HPV infection may represent alternative oncogenic mechanisms for IPSCC [80]. The most common HPV strains observed in SCC were the high-risk strains HPV-16 and HPV-18. SCCs have been associated with significantly higher viral loads than IPs and controls. Yamashita et al. found in a study that all 5 SCC and 16 IP-SCC patients with HPV-16 infection showed mixed type integration, whereas the majority of IPs and controls have demonstrated HPV in its benign episomal form [72, 77]. Rooper et al. reported that transcriptionally active high-risk HPV does not play a common role in its malignant transformation into IP-SCC based on a study of 59 tumors [81].
Although the relationship of HPV infection to malignant transformation remains somewhat controversial [68, 82], a recent meta-analysis by Zhao et al. found a close association between HPV infection and malignancy, with a pooled odds ratio of 2.16 [83]. Furthermore, high-risk subtypes HPV-16, HPV-18, and HPV-16/18 coinfection had even stronger correlations, with odds ratios of 8.8, 8.04, and 18.57 respectively. In order to rule out incidental infection due to increased susceptibility of malignant tissues, further studies elucidating the molecular mechanisms of anti-apoptotic derangements and tumorigenesis are required [84].
Discussion
Using evidence-based and systematic scientific review methods, this study aimed to elucidate the usefulness of numerous clinical investigative options for characterising IP-SCC. IP-SCC can either be found at the initial presentation, or during follow-ups when recurrences are identified. The literature does not provide findings that differentiate between the two scenarios. The senior authors recommend that the endoscopic exam followed by a biopsy be the gold standard in identifying IP-SCC. However, there are clinical scenarios where the endoscopic exam may not be possible, or concern that the biopsies are non-representative. We recommend clinicians follow patients with MRI. Given the high recurrence rate in the first 2 years following the original resection, and the mean interval between first resection and malignancy is about 40 months, our clinical practice is to do serial MRI scans for 3 years and then a repeat MRI at 5 years when the endoscopic exam may not be possible, or concern that the biopsies are non-representative. Also, in these scenarios, a complete head and neck examination is recommended on a yearly basis due to the sporadic sites of IP-SCC can be found.
The senior authors do not use CT in elucidating the presence of IP-SCC due to lack of strong evidence. While there is evidence to support the use of PET-CT, the senior authors do not use PET-CT to determine the presence of IP-SCC due to costs and access. If the MRI is suspicious, the authors will take the patient to the operating room to get a frozen section biopsy. If it is positive for SCC, a PET-CT is done post-operatively to determine if there is metastatic spread of the tumor.
The future of surveillance will include biological markers. While this study clearly illustrates there is no utility in using biomarkers at the present time, there are several biological markers that have shown great potential as prognostic indicators. Genetic factors such as MSX2, PDCD4, KRAS, PTEN are thought to play an important role in malignant transformation. Several proteins, including SCCa, fascin, survivin, COX-2, cell adhesion molecules and Ki-67 are found in higher levels in IP-SCC than in IP. Further research in this area may allow for an accessible test for clinicians to use to help risk stratify IP patients.
Conclusion
Based on the evidence level of various methods to identify IP-SCC, while histological diagnosis is the gold standard for the diagnosis of malignant transformation, clinicians should keep in mind of the sampling error of endoscopic biopsy. MRI as a standalone technique is the preferred modality in recognizing malignant transformation of inverting papilloma. Further clinical trials are required to reinforce these findings. This study also identified a number of biological markers that may become key markers in the future for identifying patients that require close follow-up.
Footnotes
Acknowledgements
Not applicable.
Authors’ contributions
CL conducted preliminary literature review; reviewed and conducted the EBR for clinical investigative options. JB reviewed and analyzed genetic factors related literature, AH reviewed and analyzed proteins and viral factor related literature, JH participated in the preliminary literature review. AT oversaw the project and provided supervision and guidance throughout. All authors read and approved the final manuscript.
Funding
Not applicable.
Availability of data and materials
Data sharing is not applicable to this article as no datasets were generated or analysed during the current study.
Abbreviations
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.