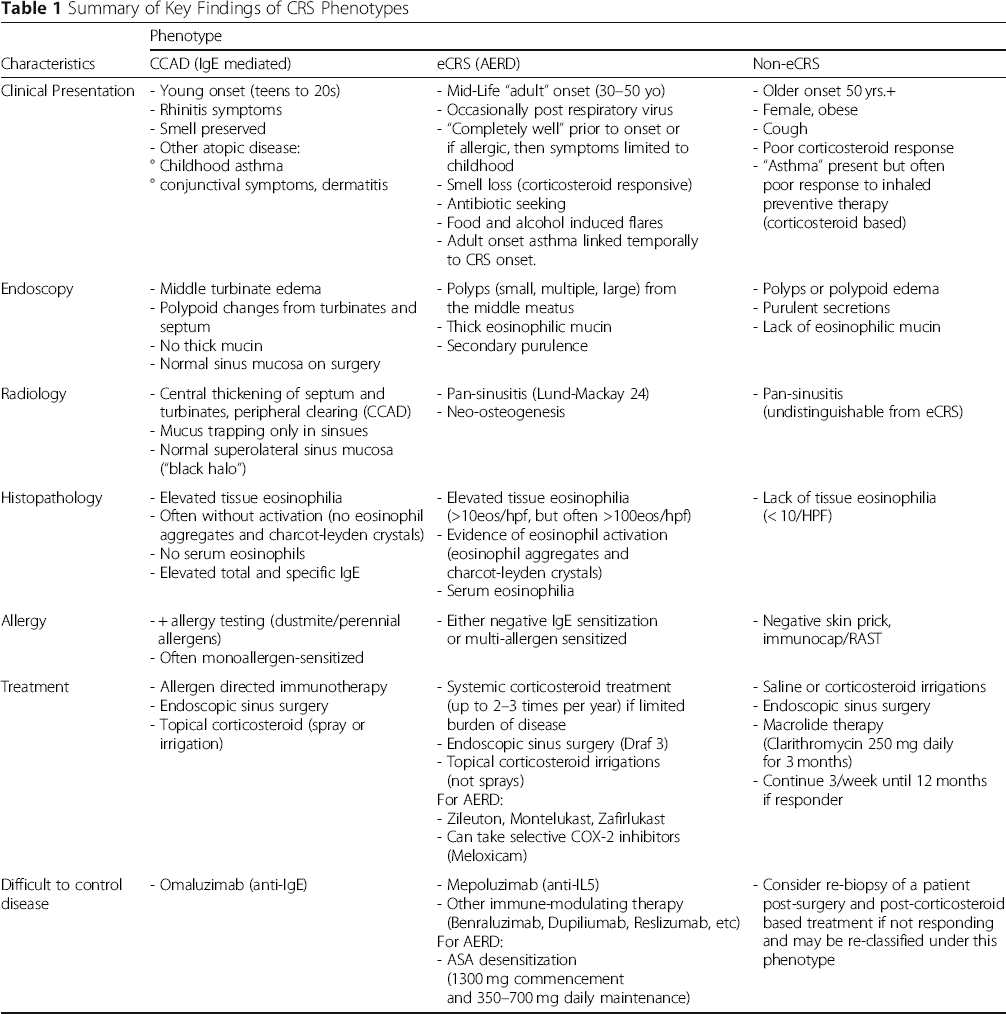
| Clinical Presentation |
- Young onset (teens to 20s)
- Rhinitis symptoms
- Smell preserved
- Other atopic disease:
° Childhood asthma
° conjunctival symptoms, dermatitis
|
- Mid-Life “adult” onset (30–50 yo)
- Occasionally post respiratory virus
- “Completely well” prior to onset or if allergic, then symptoms limited to childhood
- Smell loss (corticosteroid responsive)
- Antibiotic seeking
- Food and alcohol induced flares
- Adult onset asthma linked temporally to CRS onset.
|
- Older onset 50 yrs.+
- Female, obese
- Cough
- Poor corticosteroid response
- “Asthma” present but often poor response to inhaled preventive therapy (corticosteroid based)
|
| Endoscopy |
- Middle turbinate edema
- Polypoid changes from turbinates and septum
- No thick mucin
- Normal sinus mucosa on surgery
|
- Polyps (small, multiple, large) from the middle meatus
- Thick eosinophilic mucin
- Secondary purulence
|
- Polyps or polypoid edema
- Purulent secretions
- Lack of eosinophilic mucin
|
| Radiology |
- Central thickening of septum and turbinates, peripheral clearing (CCAD)
- Mucus trapping only in sinsues
- Normal superolateral sinus mucosa (“black halo”)
|
- Pan-sinusitis (Lund-Mackay 24)
- Neo-osteogenesis
|
- Pan-sinusitis (undistinguishable from eCRS) |
| Histopathology |
- Elevated tissue eosinophilia
- Often without activation (no eosinophil aggregates and charcot-leyden crystals)
- No serum eosinophils
- Elevated total and specific IgE
|
- Elevated tissue eosinophilia (>10eos/hpf, but often >100eos/hpf)
- Evidence of eosinophil activation (eosinophil aggregates and charcot-leyden crystals)
- Serum eosinophilia
|
- Lack of tissue eosinophilia (< 10/HPF) |
| Allergy |
- + allergy testing (dustmite/perennial allergens)
- Often monoallergen-sensitized
|
- Either negative IgE sensitization or multi-allergen sensitized |
- Negative skin prick, immunocap/RAST |
| Treatment |
- Allergen directed immunotherapy
- Endoscopic sinus surgery
- Topical corticosteroid (spray or irrigation)
|
- Systemic corticosteroid treatment (up to 2–3 times per year) if limited burden of disease
- Endoscopic sinus surgery (Draf 3)
- Topical corticosteroid irrigations (not sprays)
For AERD:
- Zileuton, Montelukast, Zafirlukast
- Can take selective COX-2 inhibitors (Meloxicam)
|
- Saline or corticosteroid irrigations
- Endoscopic sinus surgery
- Macrolide therapy (Clarithromycin 250 mg daily for 3 months)
- Continue 3/week until 12 months if responder
|
| Difficult to control disease |
- Omaluzimab (anti-IgE) |
- Mepoluzimab (anti-IL5)
- Other immune-modulating therapy (Benraluzimab, Dupiliumab, Reslizumab, etc)
For AERD:
- ASA desensitization (1300 mg commencement and 350–700 mg daily maintenance)
|
- Consider re-biopsy of a patient post-surgery and post-corticosteroid based treatment if not responding and may be re-classified under this phenotype |