
Abstract
Right-sided infective endocarditis (IE) is rare, with most cases involving the tricuspid valve; isolated pulmonary valve endocarditis (PVE) is very rare. Due to the nonspecific clinical presentation, when there is a clinical suspicion of IE, heightened awareness of possible isolated PVE is necessary for timely diagnosis. This case study underscores the importance of a meticulous exploration of the pulmonary valve during transthoracic echocardiography (TTE), utilizing all possible imaging views to identify PVE. Transthoracic echocardiography plays a vital role in the diagnosis of IE by facilitating the identification of vegetations and complications.
Keywords
Introduction
The incidence of right heart valve endocarditis is less frequent than that of left heart valve endocarditis. Native pulmonic valve endocarditis (PVE) is very rare, with a reported incidence of isolated PVE of 1-2% of all cases of infective endocarditis (IE). 1 Risk factors for right-sided IE include intravenous drug use, prolonged use of central venous catheters, or cardiac implantable electronic devices, and the presence of an underlying right-sided cardiac anomaly. 2
Echocardiography is considered to provide primary imaging criteria to diagnose IE. According to the modified Duke criteria, echocardiographic evidence of IE includes the presence of a vegetation, valvular or leaflet perforation, valvular or leaflet aneurysm, abscess formation, pseudoaneurysm, or an intracardiac fistula. Significant new valvular regurgitation is also another diagnostic sign of IE. 3
Careful interrogation of all valves, with all possible imaging views, is the mainstay for detecting vegetations and complications. Due to the rare occurrence, along with the technical difficulty of imaging the pulmonary valve (PV) by transthoracic echocardiography (TTE) in the adult population, native PVE may go undetected. Transesophageal echocardiography (TEE) is more sensitive for dynamic visualization of PV vegetations. Doppler echocardiography also assists in the assessment of the extent of valve damage to help with the decision-making.
A patient case is presented of isolated native PVE in a 63-year-old man with Enterococcus faecalis bacteremia. The diagnosis was made by identifying two large vegetations on the pulmonary valve on TEE examination.
Case Report
A 63-year-old nonsmoker and nonalcoholic male presented to the emergency department (ED) with complaints of malaise, gait problems, dizziness, polyuria, polydipsia, chills, and fatigue for past several days. His past medical history was notable for Type 2 diabetes mellitus, gout, hypertension, hyperlipidemia, and benign prostatic hypertrophy. He had undergone nephrostomy tube placement with subsequent left ureteral stent placement for a left renal stone 2 months ago. He also had 3-4 recent courses of antibiotic therapy, the latest with ciprofloxacin for urinary tract infection. He was noncompliant with his diabetes medication regimen. The patient denied shortness of breath or cough. He did not report any fever.
Upon arrival at the ED, he had a pulse rate of 90/minute, blood pressure of 133/79 mm Hg, respiratory rate of 36/minute, and oxygen saturation of 96%. Notably, his average temperature recorded for 24 hours from the time of admission was normal at 99.1°F. General and systemic examination findings were unremarkable. Laboratory findings were notable for hyperglycemia with random blood sugar level of 534 mg/dL, bicarbonate level of 12 mEq/L, and serum β-hydroxybutyrate (BHB) levels of 5.3 mmol/L consistent with hyperosmolar hyperglycemic state (HHS). Serum creatinine and blood urea levels were 1.71 and 28 mg/dL, respectively, suggestive of acute kidney injury. His baseline electrocardiogram (ECG) showed sinus rhythm with occasional ventricular premature complexes and nonspecific intraventricular conduction delay. He was admitted for further management and repeat urine analysis and blood culture samples were sent. Although the initial blood cultures were sterile, repeat cultures revealed E faecalis bacteremia for which he was started on antibiotics.
Based on positive blood culture results, a TTE was performed to investigate for possible IE on the third day of hospitalization. This study did not reveal any significant valvular diseases (See Figure 1; QR code: Video 1, 2). Simpson’s biplane ejection fraction was measured as 59% and the right ventricular function was normal.
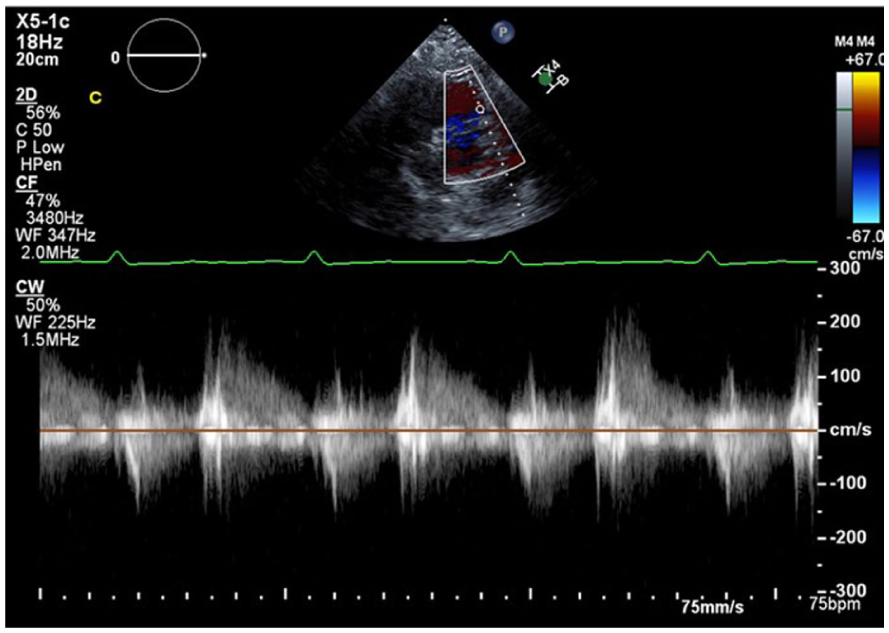
A continuous wave spectral Doppler of the pulmonary vein showed mild pulmonary regurgitation
A TEE was performed on the fifth day of hospitalization to further investigate for IE. Transthoracic echocardiography revealed 2 large mobile masses of 18 mm × 15 mm and 13 mm × 14 mm dimensions attached to the pulmonary valve with moderate-to-severe pulmonary regurgitation consistent with IE of the pulmonary valve (See Figure 2, QR code: Videos 3-8).
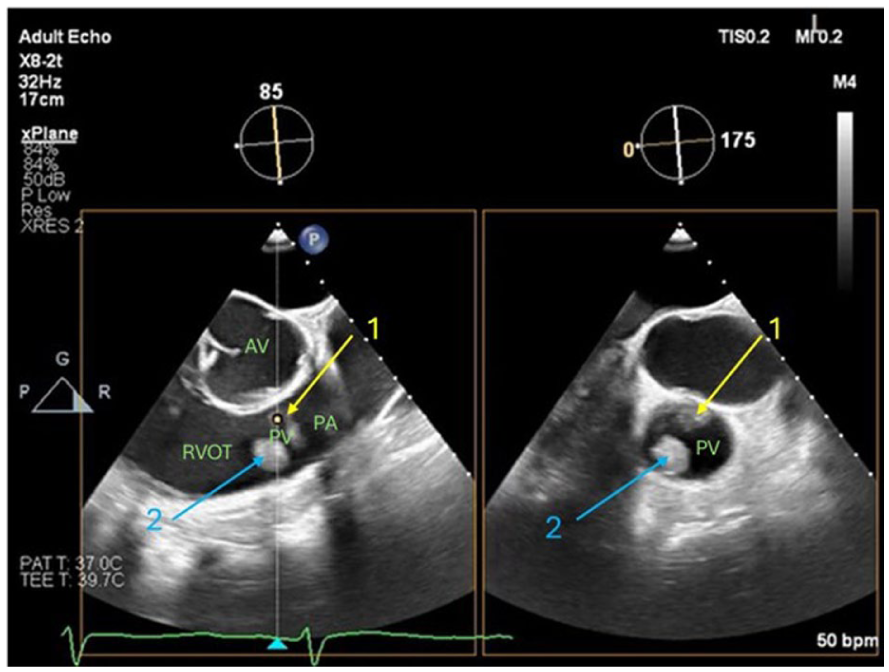
An X-plane TEE mid-esophageal short-axis set of images demonstrated two distinct masses (denoted by the yellow and blue arrows), which appear to be attached to the pulmonary valve (Note: AV – Aortic valve, RVOT – Right ventricular outflow tract, PA – Pulmonary artery, and PV – Pulmonary valve).
There was no evidence of vegetations, significant stenosis, or regurgitation of the other three cardiac valves (See QR Code: Videos 9-11). Both right and left ventricular systolic functions were reported as normal.
A computed tomographic (CT) examination of the chest was performed, which was unremarkable but had mild calcified aortic plaque, mild bibasilar atelectasis, and small effusions.
The case was discussed with a cardiac surgeon for possible surgical intervention.
The patient was further diagnosed with multi-vessel coronary artery disease after the left heart catheterization was done as part of the pre-operative workup for pulmonary valve debridement.
The patient underwent double coronary bypass surgery (i.e., left internal mammary artery to left anterior descending coronary artery and saphenous venous graft to ramus), PV debridement, and excision. Intraoperatively, the PV was found to be highly infected with large vegetations, and the decision was made not to replace the valve. Postoperatively, the patient developed hypotension and hypoxemia requiring emergent reopening. Patient was placed on veno-arterial extracorporeal membrane oxygenation (VA-ECMO) device due to persisting hemodynamic instability. A repeated TTE performed 2 days later revealed a visually estimated left ventricular ejection fraction (LVEF) of 40-45% and absent PV (See Figure 3) with significant turbulence by color Doppler in the right ventricular outflow tract (RVOT) (See Figure 4).
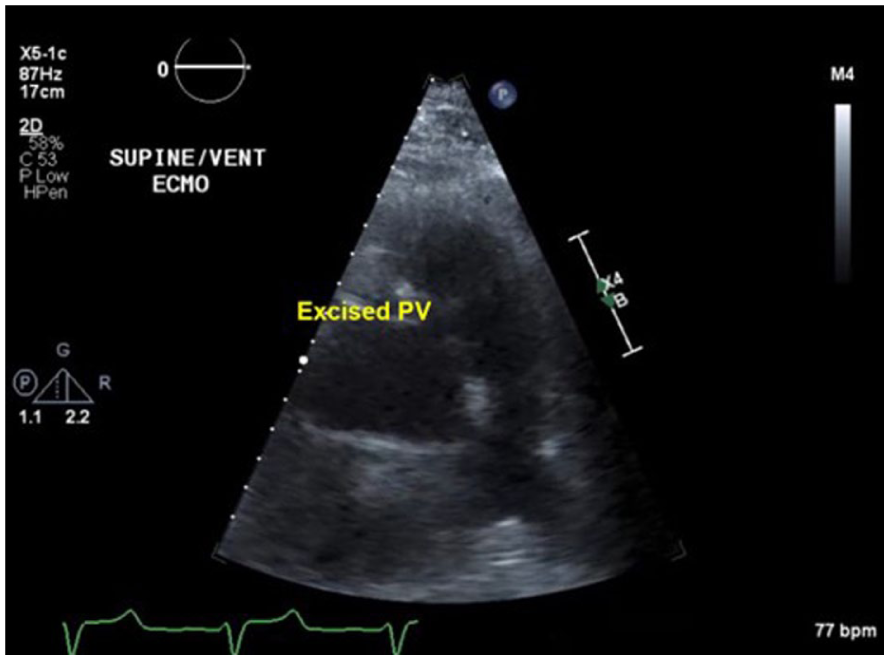
A TTE parasternal short-axis view, at the aortic valve level, showed the right ventricular outflow tract and main pulmonary artery with absent/excised pulmonary valve (PV).
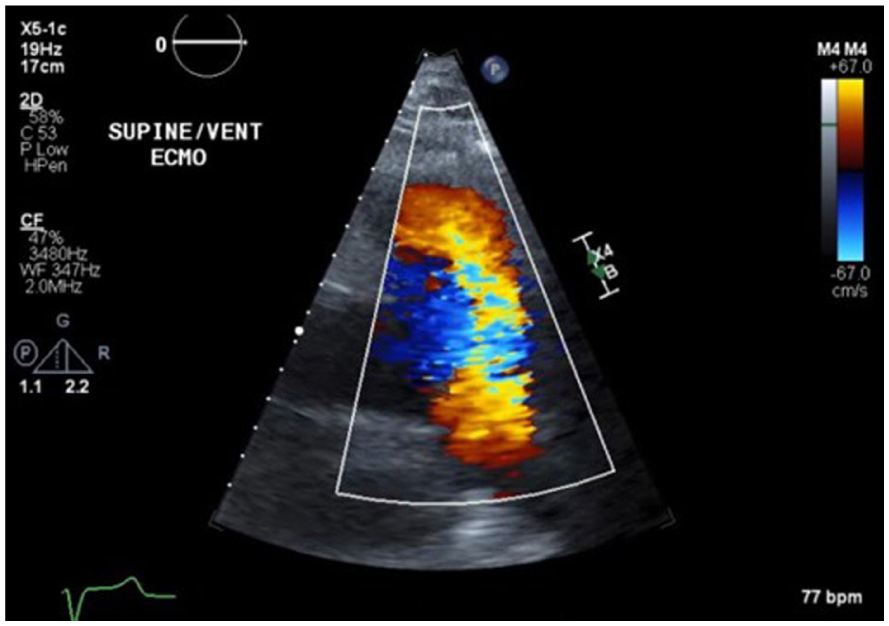
A TTE parasternal short-axis view, at the aortic level, showed color Doppler of right ventricular outflow tract/Pulmonary artery in diastole, which indicated severe pulmonary regurgitation.
Continuous wave Doppler across the RVOT showed free pulmonary regurgitation with steep deceleration (i.e., short pressure half-time) of the PR signal, indicating severe PR (See Figure 5). The patient’s RV showed mild dilation and septal bowing.
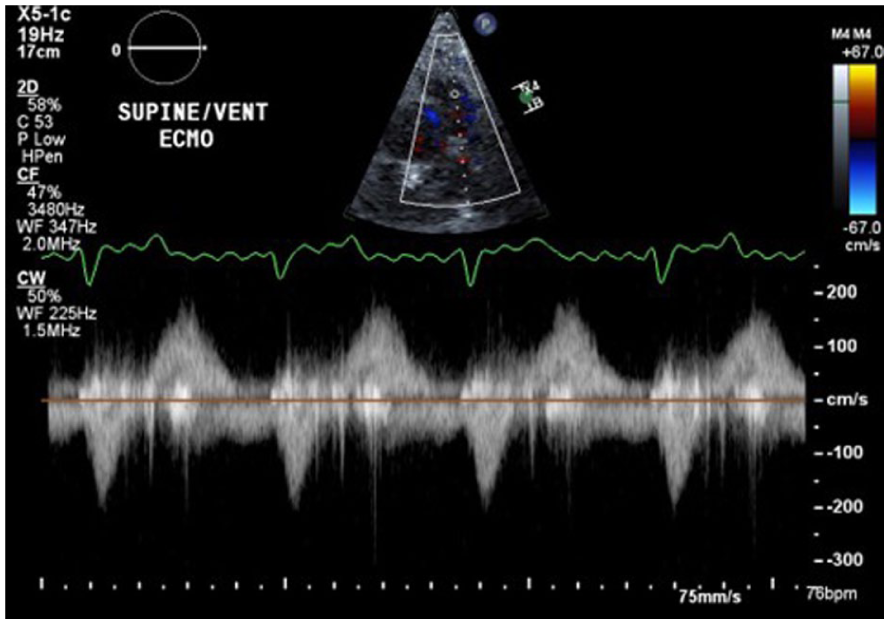
A continuous wave spectral Doppler, across right ventricular outflow tract, showed pulmonary regurgitation with rapid equalization.
A limited TEE performed 4 days postsurgery, during the VA-ECMO wean trial, showed normal left ventricular function and a moderately dilated right ventricle with mildly reduced RV function. Two-dimensional imaging of PV showed status post PV excision with a remnant of the PV tissue in the right ventricular outflow tract and wide-open pulmonary insufficiency with rapid equalization on color flow Doppler (See QR Code: Videos 14, 15). The patient tolerated TEE with ramping down well. Two days later, he underwent PV replacement using a 29.0-mm Inspiris Resilia (Edwards Lifesciences Corp, Irvine, CA) aortic valve along with right ventricular outflow tract augmentation using a supple Peri-Guard patch. ECMO was explanted on the same day.
The patient showed steady improvement in the postoperative period and was discharged to a rehabilitation center in a stable state 12 days after the pulmonary valve replacement.
Discussion
Infective endocarditis is the blood-borne microbial infection of the endothelial surface of the heart that predominantly affects heart valves but can affect the endocardial lining of the heart and great vessels and the intracardiac devices and prostheses. The characteristic lesion of IE is vegetation, which will appear on echocardiogram as a mobile echogenic mass attached to the valve. Left-sided heart valves are most affected. Right-sided IE is rare and comprises about 12% of all IE patient cases. 4 Most often, right-sided IE affects the tricuspid valve, and isolated involvement of native PV is extremely rare. This is more often seen in intravenous (IV) drug users. 5 Congenital or acquired heart valve lesions, long-dwelling central venous catheters, and intracardiac devices are other important risk factors for right-sided endocarditis. 6 Chronic alcoholism and immunodeficiency states are other predisposing factors.
Staphylococcus aureus is the most common causative organism of IE in IV drug users, the other organisms being coagulase-negative Staphylococcus, group B Streptococcus, and Enterococcus species. In non-IV drug users, the predominant organism causing IE is Streptococcus viridans. 7 E faecalis has been reported in patients undergoing invasive procedures to an increased extent; hence, such procedures are coming up as a risk factor. 8
Native PVE is a very rare entity, constituting only 1-2% of all the valves. A high index of clinical suspicion is necessary for early diagnosis and treatment. The scarce occurrence of PVE is attributed to the lower oxygen content and the lower pressure gradients on the right side of the heart, making it less favorable for the development of IE. Comparatively, a lower frequency of congenital or acquired valvular abnormalities of PV also contributes to the lower prevalence of PVE.9,10 Pulmonary valve vegetations are usually larger in size compared to left-sided endocarditis. Vegetations on the valve leaflets will lead to valvular dysfunction, which usually manifests as a new valvular regurgitation or as an increase in the severity of the existing regurgitation with or without stenosis. 2
Untreated PVE can lead to complications such as abscess formation, septic pulmonary thromboembolism, pulmonary infarction, and acute respiratory failure. Timely detection of endocarditis is crucial to preserve valve function and avoid mortality. 7
Owing to the scarcity of PVE, diagnosis can be challenging unless there is a high index of clinical suspicion, especially in cases of unexplained bacteremia. Clinically, patients present with generalized symptoms like fever, chills, respiratory symptoms, and fatigue. Right-sided cardiac murmurs are missed more often than usual. Patients may also present symptoms associated with complications such as embolic phenomena, presenting with lower lobe pneumonia.2,9 Serial blood cultures are the cornerstone in the diagnosis of IE. Both transthoracic and transesophageal echocardiography play a pivotal role in the diagnosis by enabling direct visualization and characterization of vegetations, to assess the degree of valvular dysfunction and in the detection of complications like abscess. 2
Although TTE is a valuable tool for diagnosis, the pulmonary valve is not always well visualized in adults by TTE. Therefore, a vigilant screening of PV in the short-axis view at aortic level is cardinal in detecting PVE. Sliding the ultrasound probe up one rib space with slight clockwise rotation of the probe, angling its face more anterior toward the PV enables better visualization of the PV leaflets than the standard aortic level short-axis view. Imaging the PV leaflets can also be achieved from the right ventricular tract outflow view, the apical and subcostal 4-chamber views with extreme anterior tilting, and from the subcostal short axis view. M-mode of PV also provides information on the presence of PV mass as irregular, shaggy echoes on the PV leaflets. Additionally, if available, biplane imaging (also known as X-plane) allows simultaneous interrogation of the valve in two orthogonal planes that may provide a better view of the valve leaflets. Continuous wave Doppler interrogation of PV will show significant pulmonary regurgitation (PR) with a strong/dense signal and a short pressure half-time with early termination of the PR signal.
In this patient case, the initial TTE was technically challenging due to poor acoustic windows, which did not reveal any significant abnormalities. Color Doppler was suboptimal and continuous wave Doppler was not impressive. Moreover, PV was interrogated from the parasternal short-axis view only. Later, TEE identified two large mobile masses on the PV, which in the clinical context were highly suggestive of IE.
When TTE is technically difficult and valvular morphology cannot be well visualized, or if the TTE is negative in a patient with high index of clinical suspicion of IE, TEE should be considered. TEE is more sensitive in detecting vegetations on PV. 5 However, Doppler assessment of pulmonary regurgitation by TEE can be challenging due to the more anterior location of PV. 11
Cardiovascular magnetic resonance imaging (CMR) is another useful imaging technique to visualize, evaluate, and assess PVE complications like pulmonary embolism. Computed Tomography Pulmonary Angiogram (CTPA) is the imaging technique of choice for diagnosing septic pulmonary thromboembolism, a common complication of PVE.
The differential diagnoses in lieu of PVE are thrombus, malignancy, and papillary fibroelastoma. In the patient case, the surgical photos or histology results were not available.
Management of PVE encompasses appropriate prolonged antibiotic therapy as gauged by blood culture sensitivities. 12 The literature notes large vegetations of 20 mm in diameter or more, persistent bacteremia, other complications like valve ring abscess, or perforation may warrant surgical excision of vegetation or debridement, valve repair or replacement, depending on the level of valve compromise.2,12
Prognosis of PVE is better than that of left-sided infections. However, prompt and precise diagnosis is vital in preventing serious complications and thereby decreasing morbidity and mortality. 2
In this case, the patient eventually underwent pulmonary valve replacement, following TEE identification of two relatively large mobile pulmonary vegetations involving PV. The patient was asymptomatic at the time of discharge to the rehabilitation center.
Conclusion
Isolated pulmonary valve endocarditis is a rare entity, and meticulous evaluation during echocardiography is crucial to identify PV vegetations. The chances of missing this important diagnosis in a suboptimal TTE can be reduced by obtaining unconventional views during TTE and M-mode of PV. TEE is more sensitive in detecting vegetations and should be performed when there is a high clinical suspicion of IE and TTE is negative.
Timely detection and management of PVE will reduce morbidity and mortality from complications like septic pulmonary embolization and acute respiratory failure. This case demonstrates the importance of thorough echocardiographic interrogation of PV from all possible views, even when the other valves show normal morphology, when there is a strong clinical concern of IE. It also emphasizes the significance of TEE to uncover IE vegetation that may be missed by TTE.
Supplemental Material
sj-pdf-1-jdm-10.1177_87564793261448896 – Supplemental material for A Case Study of Isolated Native Pulmonary Valve Infective Endocarditis
Supplemental material, sj-pdf-1-jdm-10.1177_87564793261448896 for A Case Study of Isolated Native Pulmonary Valve Infective Endocarditis by Rema Vinod, Stanley Ort and Beena Vaidya in Journal of Diagnostic Medical Sonography
Footnotes
Acknowledgements
The authors acknowledge the technical expertise of Mohammed Gibreal, MD, and Ambreen Fatima Ali, MD, in obtaining the TEE images and videos used in this case report. We thank them for graciously allowing us to include these visuals in the article.
Ethical Considerations
Ethical approval was not sought for the present study all patient data was deidentified.
Consent to Participate
Verbal informed consent (verbal assent) was obtained from the subject before the release of the report for review.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.