
Abstract
Dialysis-associated steal syndrome (DASS) is an uncommon disease that can be detected with careful and precise sonographic techniques. Arteriovenous (AV) access surgery is performed for patients with end-stage renal disease (ESRD) requiring regular hemodialysis. DASS is defined as retrograde flow in the native artery, distal to the AV access anastomosis. The blood direction reverses and re-routes flow from the distal extremity into the proximal, surgically created AV access vein or graft. Without detection and treatment, tissue loss to the extremity can occur. A wrist brachial index (WBI) and digital brachial index (DBI) evaluation utilizing photoplethysmography (PPG) is useful to confirm suspected DASS and determine the stage or severity of the steal. Sonographers familiar with WBI will notice a change in protocol when evaluating a patient for steal syndrome. This advanced Doppler technique is demonstrated in the case of a patient with a brachiocephalic fistula and symptoms of DASS. A deeper understanding of steal syndrome and how to perform this uncommon examination could improve outcomes for patients with DASS.
Keywords
Dialysis-associated steal syndrome (DASS), also known as hemodialysis access-induced distal ischemia (HAIDI), affects between 1% and 8% of patients with arteriovenous (AV) access.1,2 Retrograde flow in the native artery, distal to the AV access anastomosis, is an uncommon adverse outcome of an AV access surgical procedure (See Figure 1). Prolonged effects lead to morbidities including tissue or limb loss from necrosis. 2 While the AV fistula (AVF) is the first choice among vascular surgeons, careful consideration is taken when selecting AV access candidacy to reduce the risk of the development of DASS. 3 Risk factors include diabetes, female, and age greater than 60 years. 2 There is also an increased incidence of DASS with a more proximal AVF creation site. 2 The incidence of a brachiocephalic AVF developing into a steal syndrome is 1%–8%, while that of a radiocephalic AVF is 1%–2%. 3 Vascular surgeons will also consider the patient’s history, the presence of atherosclerosis, and the use of defibrillators or pacemakers. 4 They also review the patient’s vein sizes and location when making this decision. In this pre-surgical stage, the surgeon will likely order a vein mapping sonographic study to determine if a vein is suitable for AV access creation. For a successful AVF creation, it is suggested to use a cephalic vein between 2.0 and 2.5 mm for radiocephalic AVFs or at least 3.0 mm in AP diameter for brachiocephalic AVFs. 5 It is suggested to use basilic vein at least 2.5 mm in AP diameter for brachiobasilic AVFs. 6
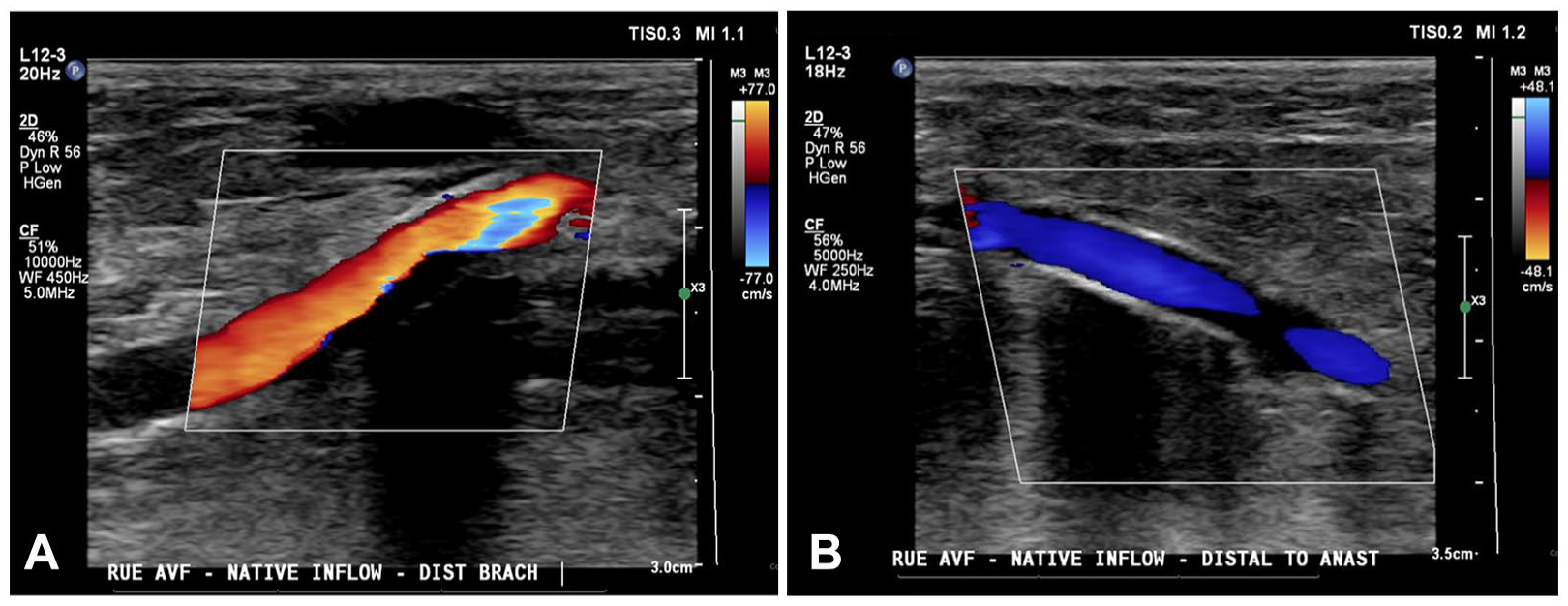
(A) Color Doppler imaging of antegrade flow seen in the native artery proximal to the patient’s anastomosis. (B) Color Doppler imaging of retrograde flow seen in the native artery distal to anastomosis is suggestive of steal syndrome.
Most patients with DASS are asymptomatic likely due to dilation of adjacent arteries compensating for the lack of perfusion; however, those with symptoms may experience pain, numbness, coldness, and rest pain in the hand and the arm distal to the AVF.3,7 Symptoms are often more noticeable during dialysis due to the reduction in venous return and cardiac output, which then reduces pressure in the outflow artery and causes hand ischemia and eventually necrosis over time.2,3
DASS is usually diagnosed in the clinical setting; however, imaging and other techniques are beneficial to evaluate the severity and monitor the progression of the disease, such as digital brachial index (DBI), pulse oximetry, electromyography, Doppler ultrasound imaging, and angiography. 1 In a physical evaluation, if benefits outweigh the risks, clinicians may choose to manually compress the AVF to assess if flow returns. If this temporary compression returns distal perfusion and relieves symptoms, high flow is likely the cause of DASS.1,4 Excessive access flow is defined as flow greater than 1500 mL/min. 1 To calculate the flow volume, spectral Doppler is the common diagnostic tool. The spectral gate is opened to include the full amount of blood flowing through the vein, in one area. To measure, select the flow volume measurement. Place calipers at the vessel walls perpendicular to its length, on the grayscale image, and then review a range of at least three waveforms, based on the spectral tracing. This takes an average of flow across those three waveforms within the diameter measured (See Figure 2). Collecting measurements at tortuous or stenotic areas of the outflow vein will lead to erroneous velocity and flow volume values; therefore, it is important to observe the outflow vein carefully to avoid these areas. 3
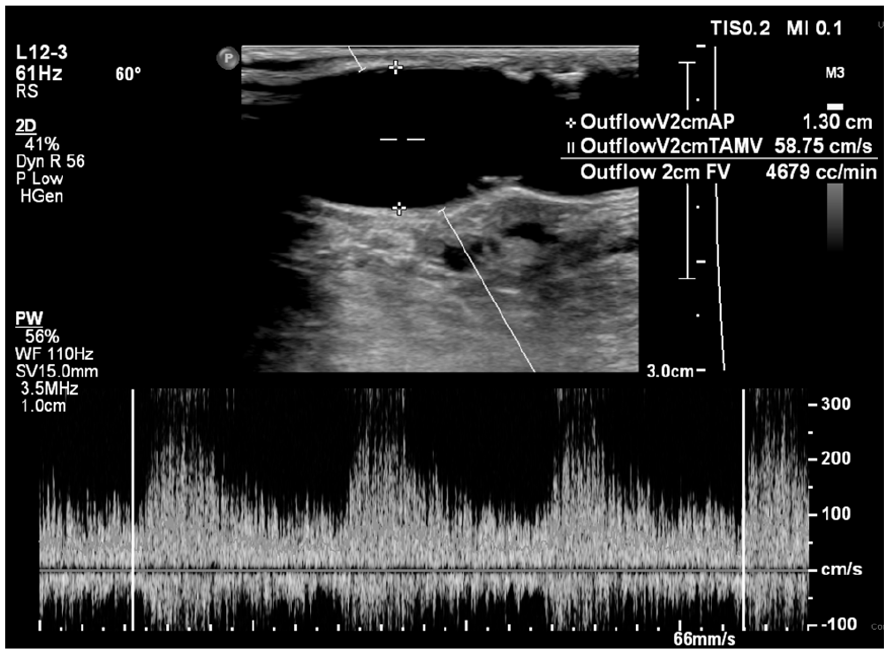
Grayscale and spectral imaging of the flow volume in a patient’s outflow vein. The flow volumes are over 1500 mL/min and are common causes of DASS.
A wrist brachial index (WBI) and DBI evaluation is useful as a non-invasive, non-ionizing screening tool in asymptomatic patients, to confirm a suspected DASS, or determine the stage or severity of the steal. 1
Photoplethysmography (PPG) detects blood waveform changes in the digits and aids in determining accurate blood pressure readings. The patient should be positioned so that their arms are flat and level with the heart. 8 The pressure cuffs are placed on the upper arm and wrist of the unaffected upper extremity. Though dependent on patient body habitus, the 12-cm cuff is recommended for the upper arm, and the 10-cm cuffs are recommended for the wrists. The smaller 2.5-cm pressure cuffs and PPG sensors are also placed on the digits bilaterally. There are no specific laboratory accreditation standards set for which fingers are recommended to be sampled in a WBI. The department protocol for this study dictated that the second and fourth digits were to be sampled, unless otherwise specified. A diagram of the recommended cuff sizes and placements is shown in Figure 3.
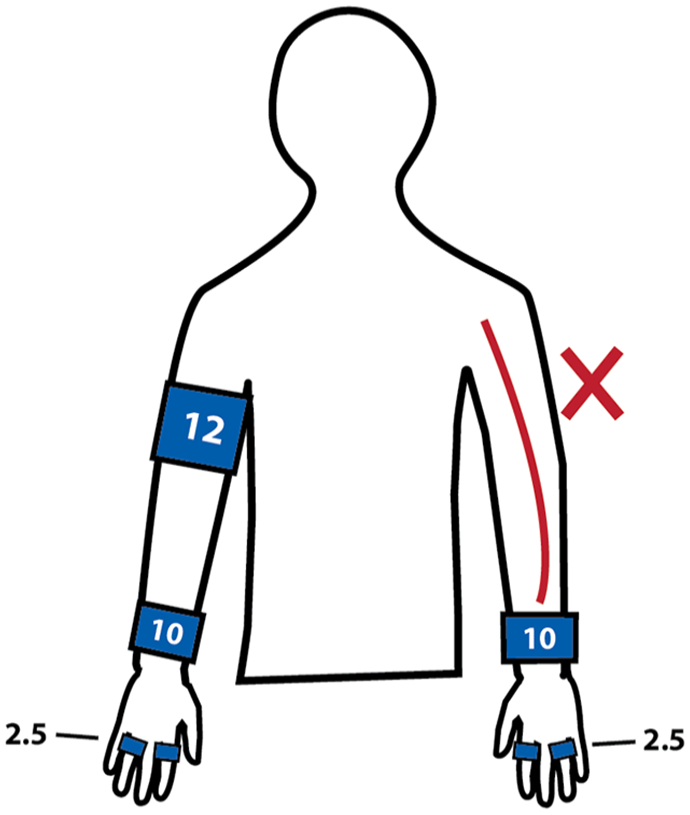
A diagram is provided, which demonstrates the recommended pressure cuff size and layout for a WBI for steal syndrome. Never place a pressure cuff over the outflow vein, which is usually the patient’s upper arm on the side of the AVF. When performing a manual compression, the sonographer should use two fingers to gently compress just beyond the AVF anastomosis.
A normal DBI and WBI are performed on the unaffected upper extremity, obtaining waveforms and pressures of the brachial artery, distal radial artery, distal ulnar artery, second digit, and fourth digit. To evaluate the affected upper extremity, the sonographer first obtains waveforms and pressure readings of the radial and ulnar arteries and second and fourth digits. The sonographer then uses their fingers to gently compress the outflow vein just beyond the AVF anastomosis. 7 Compression should never be applied far from the anastomosis as this can cause the vein to swell dangerously. Additionally, the amount of pressure applied should not compress the inflow artery. This use of temporary compression adjacent to the anastomosis to determine a DASS diagnosis may outweigh the risks of the applied compression. It is advised that the sonographer confirms with the provider that this maneuver can be performed on the individual patient prior to the exam, in consideration of unique circumstances.
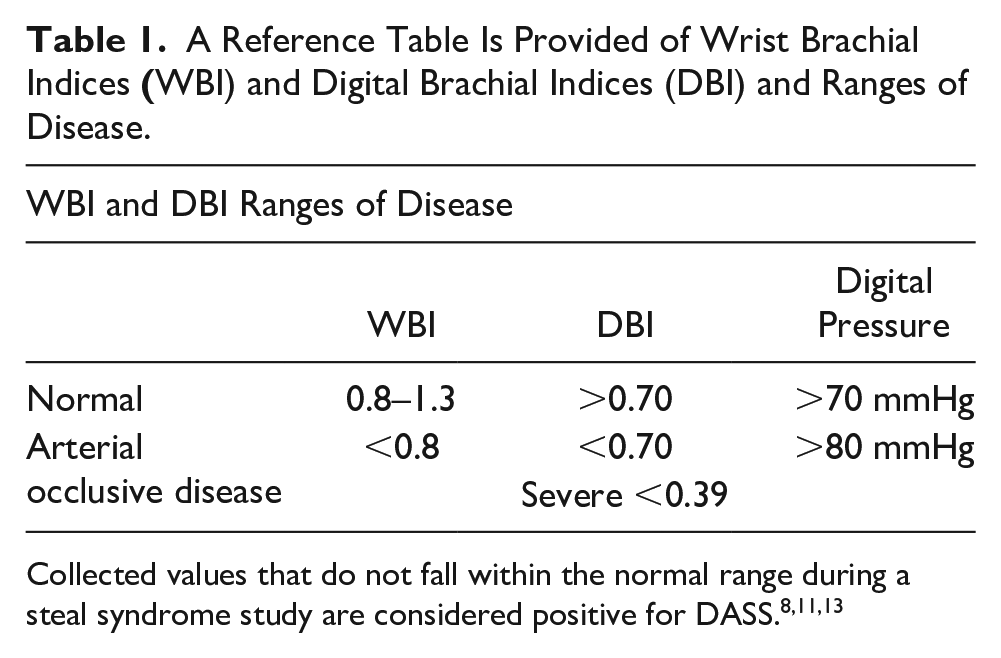
Waveforms and pressure readings of the radial and ulnar arteries with the second and fourth digits are recorded again, while the vein is compressed. When positive for DASS, the waveforms of all distal arteries and fingers should increase in amplitude, and the digital pressures will increase in value after compression. This increase in amplitude and digital pressure occurs because the compression stops flow to the outflow vein, thereby restoring it to the distal extremity. Figure 4 shows a positive DASS WBI examination in which the patient has a right upper extremity AVF. The left upper extremity waveforms demonstrate higher amplitudes compared with the waveforms of the right upper extremity. A normal brachial, radial, and ulnar waveform should appear multiphasic with a sharp upstroke. Normal digital waveform morphology should appear consistent in amplitude and should be less than 15 mmHg difference, between fingers. 9 A DBI is calculated as the digital pressure over the higher brachial pressure. In general, a normal DBI should be >0.70, with the severe disease being <0.39. 10 Patients with DASS will have a digital pressure <80 mmHg and a DBI <0.70. 1 Table 1 lists the ranges of arterial disease with WBI and DBI. The sensitivity and specificity of 80 mmHg digital pressure for DASS are 80% and 85%, respectively, and the sensitivity and specificity of 0.70 for DBI for DASS are 100% and 72.5%, respectively. 11 It is important to note that WBI sensitivity can be affected by Raynaud’s disease, scleroderma, or medial arterial calcifications. 8 Patients with these diseases will present with decreased digital pressures; therefore, they could erroneously fall into the category of DASS if their patient history is not considered. 12
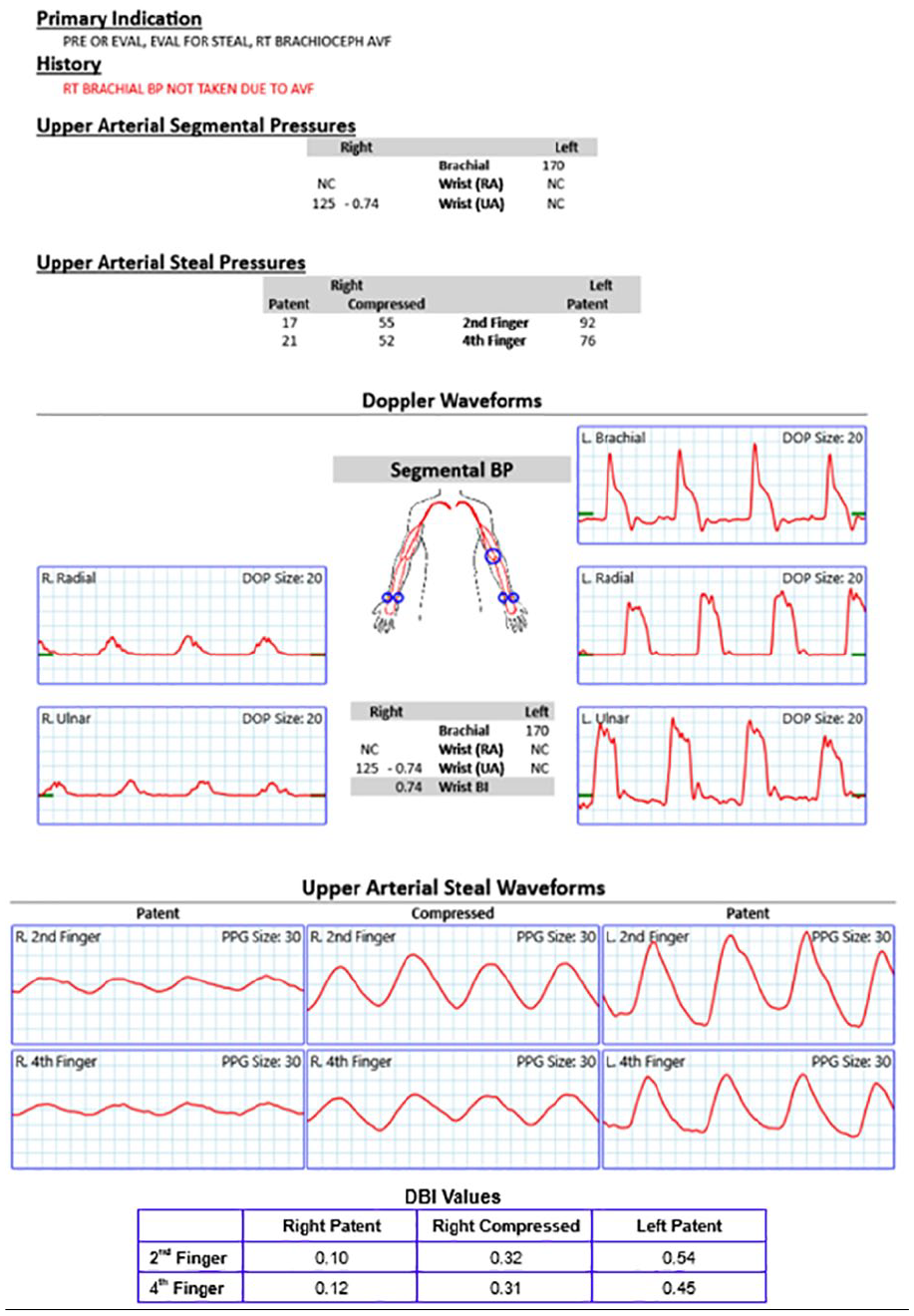
The final wrist brachial index (WBI) report, for this patient, confirmed a positive DASS diagnosis. The waveforms show the second and fourth right digits with and without compression. The digital brachial index (DBI) values are not included in the original report, but they can be calculated using the brachial and digital pressures collected.
A Reference Table Is Provided of Wrist Brachial Indices
Case Report
Collecting data with PPG and arterial indices with suspicion of DASS is demonstrated in the following patient case. A 72-year-old Hispanic male, with a history of hypertension, diabetes, smoking, and end-stage renal disease (ESRD), presented with complaints of rest pain and purulence coming from the right middle finger. His finger had been partially amputated a few months earlier for gangrene (See Figure 5). The patient’s providers were concerned that gangrene was caused by poor perfusion to the hand, due to his right upper extremity brachiocephalic AVF. Upon clinical assessment, the patient also had weakly palpable radial and ulnar artery pulses. The capillary refill time in the right digits was <2 seconds. A hemodialysis sonogram, using color and spectral Doppler, was performed. Figure 1 demonstrates the native brachial artery proximal and distal to the AVF anastomosis, and the retrograde flow in the distal native artery. Figure 2 shows the flow volume within the outflow cephalic vein, with a value at 4679 mL/min. The diagnostic findings shown in Figures 1 and 2 suggested DASS.

An image is provided of the patient’s right hand prior to AVF ligation. The third digit is seen with a prior partial amputation and persistent gangrene.
An upper extremity arterial pressure evaluation was then ordered to confirm the diagnosis. The pressure of the second digit increased from 17 to 55 mmHg, and the pressure of the fourth digit increased from 21 to 52 mmHg after compression was applied (See Figure 4). The waveforms in both digits also increased in amplitude after compression was applied. After compression, the waveform morphologies of the right digits were more like that of the asymptomatic left digits, with adequate blood flow. The patient’s providers then ordered a computed tomography angiography (CTA) of the right upper extremity, to further evaluate the vessels. The combined results of the upper extremity arterial pressure evaluation, the CTA, and the visible ischemia in the patient’s hand supported the diagnosis of DASS.
Due to the stage of the disease, the best option for this case study patient was ligation of the AVF. This decision was not taken lightly, as the patient would have needed a new route for hemodialysis. Post-procedure, the surgeons noted a successful complete loss of thrill, from the AVF and were able to palpate a radial pulse. The patient was also instructed to take oral antibiotics for the infection in the right hand. The patient had a resulting appointment with the vascular surgeon 1 week later where he reported a resolution of right-hand rest pain, since the ligation. Another subsequent visit, 2 weeks later, showed incomplete healing and persistent ischemia to the middle finger, resulting in a small area of necrosis. The providers agreed to a revision amputation of the right middle finger, 3 days later.
Discussion
Patients diagnosed with DASS will have perpetuating or worsening distal upper extremity pain and ischemia, if not treated appropriately. After a patient has been diagnosed with DASS, further imaging with digital subtraction angiography (DSA) may be ordered, to further evaluate the vessels and determine the best method of treatment.1,4 Treatment is determined by the severity of the disease and symptoms. There are many treatment options, including banding or plication, proximalization of arterial inflow (PAI), percutaneous transluminal angioplasty (PTA), anastomosis reductions, and ligation.4,14 Banding is a procedure in which a synthetic band is wrapped around the outflow vein, just beyond the anastomosis, to reduce its diameter and create a stenosis. Similarly, plication involves metal clips sutured on the outflow vein to reduce its diameter. 14 These procedures are performed with the intention of creating a stenosis in the outflow vein. 4 This causes an increase in resistance and reduces the flow, allowing adequate blood flow to return to the artery and reversing the steal. The PAI procedure uses graft material to reroute arterial flow from the axillary artery instead of the brachial or radial arteries.4,14 The larger diameter and increased pressure from the axillary artery reduce the effects of the steal. PTA is performed to correct any areas of stenosis distal to the anastomosis while keeping the AVF intact. 4 With a surgical anastomosis reduction, less flow can pass through to the outflow vein, potentially reducing the steal. If revision surgery is not indicated, urgent ligation is often the last option. 7 Since this procedure removes the dialysis access in the extremity, ligation is usually only recommended in patients with a previously failed steal-correcting procedure, gross ischemic necrosis, or in patients with a more limited life expectancy.4,14
In a similar case reported by Lim, a patient with brachiocephalic AVF and DASS symptoms underwent diagnostic testing. 15 While that study did not report on whether wrist pressures or DBI values were collected, digital finger pressures were recorded with and without AVF compression. Obtaining a brachial pressure and evaluating the DBI is considered more sensitive for a DASS diagnosis. For this reason, it is recommended to include DBI in the protocol when the indication suspects DASS. In that study, pressures increased from 36 mmHg before compression to 97 mmHg after compression. 15 This patient was also diagnosed with DASS and was treated with a surgical procedure called revision using distal inflow (RUDI). In RUDI, a harvested vein is used to redirect flow from the outflow vein to the distal extremity. 15 With this technique, dialysis access is maintained, and perfusion is restored to the distal extremity. Another study by Shemesh et al. evaluated a patient with a brachiocephalic graft. Initial assessment noted digital pressures between 35 and 48 mmHg and DBI values between 0.20 and 0.27. 16 This patient’s surgical treatment involved reducing the diameter of the entire graft to reduce the flow volume in the outflow vein. After surgery, the patient had improvement in digital pressures, reading 92–102 mmHg, and DBI values between 0.54 and 0.57. 16
In both cases, digital pressures increased above 80 mmHg after compression or correction of the vein. In comparison, the current patient only had an increase in digital pressure up to 55 mmHg after compression. Due to the severity of the disease, this patient was recommended complete ligation of the AVF instead of reconstruction. Ligation of the AVF relieved the DASS and hand pain, but the distal ischemia did not completely resolve. This is a possible outcome as even with compression, the patient’s digital pressures still did not increase above 80 mmHg. Additionally, this patient had noncompressible radial and ulnar arteries with monophasic waveforms, which suggested the possibility of underlying arterial disease that would complicate recovery of distal ischemia.
Conclusion
While DASS is an uncommon disease, early detection is crucial for the patient’s outcome. Since many cases are asymptomatic, it becomes the sonographer’s responsibility to evaluate for DASS in duplex hemodialysis studies, when ordered. With the knowledge of the symptoms and flow volume values that define DASS, a sonographer can be the first to encounter and explore this disease. Once detected, its severity can be evaluated with a DBI and treated before irreversible symptoms develop.
The utilization of PPG and arterial indices is a valuable diagnostic tool in detecting patients with DASS. A complete protocol should include brachial, radial, and ulnar artery pressures and waveforms, and digital pressures and waveforms, before and after compression of the AVF and just beyond the anastomosis. This compression reduces flow to the outflow vein, causing reperfusion of the distal upper extremity and alleviation of symptoms. In a way, compression mimics AVF ligation, which is usually the least desirable outcome when the patient still requires regular hemodialysis treatments. Revision surgeries are preferred because they restore blood flow to the distal extremity while maintaining a usable AVF.
In the present case report, Doppler evaluation of the patient’s AVF demonstrated massively increased flow volumes, and the arterial pressure indices indicated significant pressure increases, after compression. These pressure changes are palpated and often diagnosed subjectively; however, WBI and DBI allow for objective determination of DASS because they assign a numerical value to the pressure changes. Sonographers performing these exams should be aware of the recommended protocol and the significance of the collected values for the diagnosis and treatment of patients with DASS. An understanding of the significance of DASS and how to perform these uncommon studies can impact outcomes and improve a patient’s quality of life.
Footnotes
Declaration of Conflicting Interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author received no financial support for the research, authorship, and/or publication of this article.
Ethics Approval
Ethics approval was not sought for the present study because all case data were de-identified.
Informed Consent
Informed consent was not sought because all case data were de-identified and/or aggregated and followed the ethics committee or IRB guidelines (also referred to as the Honest Broker System).